
Abstract
The aim of this study was to evaluate MR imaging findings of the associated findings in surrounding tissues of the extra-articular soft tissue ganglion cysts around the knee. We retrospectively reviewed MR images of 30 patients who had surgically confirmed extra-articular soft tissue ganglion cysts around the knee with focus on the associated findings in surrounding tissues, such as muscle, subcutaneous fat, bone, and nerve. The most common associated finding was the visualization of channel between ganglion cyst and the joint, which was demonstrated in 20 cases (continuous type in 12 cases and discontinuous type in 8 cases). Other associated findings were seen in 15 cases; pericystic edema (n=9), bony remodelling (n=3), and nerve involvement (n=3). The bony remodelling involved the proximal metaphysis of tibia in all 3 cases. Two patients with nerve involvement had deep peroneal nerve in subacute phase and one involved common peroneal nerve in chronic phase. The MR imaging is a useful imaging modality to evaluate the associated findings in extra-articular soft tissue ganglion cysts around the knee. The evaluation of these associated findings is helpful for the differentiation of ganglion cysts from other cystic lesions around the knee.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ganglion cysts in the knee were subdivided into intra-articular, extra-articular soft tissue, and intra-osseous ganglion cysts. Intra-articular ganglion cysts have been described in several articles regarding their locations and shapes with details, but extra-articular soft tissue ganglion cysts have been described only in a few articles [1, 2, 3, 4]. Because extra-articular soft tissue ganglion cysts usually appear as uni- or multi-chambered cysts on MR imaging, they have been mentioned just as differential diagnosis of the cystic lesions such as meniscal cyst, synovial cyst or have been reported with their associated findings, such as peroneal nerve palsy or bony remodelling, in several articles [5, 6, 7, 8, 9, 10, 11].
Synovial cysts (bursae) are lined by synovial cells. Bursae are not normally visible on MR images because they contain only scant amounts of fluid. Inflammation, hemorrhage, joint effusion, or internal derangement can produce accumulation of fluid within the bursa, allowing visualization on MR images.
They occur in typical anatomic sites, so knowledge regarding its anatomic location can aid the radiologist in establishing a proper diagnosis [5, 6].
Meniscal cysts are multiloculated collections of mucinous material of unknown cause that generally occur at the periphery of the meniscus and appear as a focal mass or swelling at the joint line. Meniscal cysts are invariably associated with horizontal meniscal tears. Most authors believe that they are formed by extrusion of joint fluid through a meniscal tear into the adjacent tissues [5].
Some authors have reported the channel between the cyst and the joint plays a role as a useful diagnostic marker in the differentiation between extra-articular soft tissue ganglion cyst and meniscal cyst or synovial cyst. Delayed radiography after intra-articular injection of contrast medium was reported to be a useful method for the diagnosis of ganglion [12, 13, 14, 15]. This technique could visualize the channel between ganglion cyst and joint space. The channel is gradually converted to the fibrous band but occasionally remains as patent and makes it possible to have a clear image on MR. As far as we know, there have been few articles which describe the MR imaging findings of this channel.
In this study, we reviewed 30 cases of extra-articular soft tissue ganglion cysts around the knee with the focus on the associated findings in MR imaging, including the channel between the ganglion cyst and the knee joint. Also, we describe the locations and the sizes of ganglion cysts.
Materials and methods
We retrospectively reviewed the surgically proven 30 cases of extra-articular soft tissue ganglion cysts around the knee between 1995 and 2000. There were 8 male and 22 female patients, with a mean age of 37 years (age range 6–69 years).
Magnetic resonance imaging was performed with 0.5-T (Gyroscan T5; Philips, Eindhoven, The Netherlands) and 1.0-T scanners (Magnetom Impact, Siemens, Erlangen, Germany). Imaging sequences in the axial and sagittal or coronal planes included T1-weighted spin-echo (TR 450–650 ms, TE 15–30 ms), proton-density-weighted, and T2-weighted (TR 1800–2400 ms, TE 12–40 ms/60–90 ms) sequences. The slice thickness varied from 4 to 10 mm. In all cases, T1-weighted images were obtained again after intravenous administration of 0.1 mmol/kg of body weight of gadopentetate dimeglumine (Magnevist, Schering, Berlin, Germany) for the analysis of enhancement pattern in the soft tissue mass. The MR parameters included 10- to 20-cm field of view, a 2-mm interslice gap, and 192×256 matrix.
On MR images, we analyzed the location and size of the ganglion cysts. The location of ganglion cysts were divided into five parts with center of knee, superomedial, superolateral, inferomedial, inferolateral, and others. Others included midline, popliteal (posterocentral), and lateral locations. We also evaluated visualization of channel and the associated findings in the surrounding tissues including pericystic edema, periosteal reaction, and nerve involvement. The visualization of a channel between the cyst and the adjacent joint was assessed on T2-weighted images. Visualization of channel was estimated as being continuous, discontinuous, or absent. Pericystic edema was evaluated the abnormal high intensity around cyst on T2-weighted images. We also reviewed the change of signal intensity in surrounding muscles and the distribution of involved muscle for the evaluation of nerve involvement. Plain radiographic images were examined in each case for the evaluation of cortical erosion or periosteal reaction.
Results
Ganglion cysts revealed as hypointense signal mass on T1-weighted images and hyperintense signal mass with thin low-signal intense rim and septa on T2-weighted images in all cases. Gadolinium-enhanced T1-weighted images showed thin wall enhancement in these ganglion cysts in all cases.
Table 1 summarizes the associated findings of extra-articular soft tissue ganglion cysts around the knee. The majority of cases occurred in the supero medial region (36.7%) of the knee and others were in other locations (23.3%), inferomedial (20%), and inferolateral (13.3%) regions in decreasing order. Other locations included popliteal (13.3%), midline (6.7%), and lateral (3.3%) regions. The size of the ganglion cysts ranged from 0.9 to 4.5 cm (mean 2.3 cm) in the transverse diameters, and from 1.7 to 7.7 cm (mean 4.0 cm) in the longitudinal diameters.
The most common associated finding on MR imaging was visualization of the channel between ganglion cyst and the joint in 20 cases (66.7%) with continuity in 12 cases (Fig. 1) and discontinuity in 8 cases (Fig. 2). This channel appeared as a tract or a beaded shape between the ganglion cyst and the knee joint space on MR image with hypointense signal on T1-weighted image and hyperintense signal on T2-weighted image. It was easy to detect the channel in 20 cases, but we could not find the channel in the other 10 cases. The channels of continuous type were connected with femorotibial joint (n=6), capsular attachment to the posterior aspect of the femur (n=3), and the tibiofibular joint (n=3).

Continuous channel between ganglion cyst and tibiofibular joint in a 42-year-old man with a ganglion cyst. Coronal T2-weighted image (TR/TE: 2200 ms/90 ms) shows a ganglion cyst in fibular neck area (arrowheads), with a high signal intense, beaded, continuous channel to the tibiofibular joint (arrow)

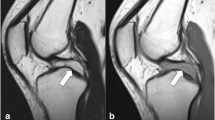
Discontinuous channel between ganglion cyst and femorotibial joint in a 63-year-old woman with a ganglion cyst. a Coronal T2-weighted image (TR/TE: 2000 ms/90 ms) reveals a high signal intensity channel (arrowheads) between the ganglion cyst (arrow) and knee joint. b Axial T1-weighted image (TR/TE: 550 ms/20 ms) at the level of the calf shows an ovoid, hypointense signal mass (arrow) in gastrocnemius muscle. c Axial T2-weighted image (TR/TE: 2000 ms/90 ms) at the level of the knee shows a small, ovoid-shaped channel (arrow), which disappeared on consecutive section, in gastrocnemius muscle
Nine cases (30%) of ganglion cysts had pericystic edema with hypointense signal on T1-weighted images and hyperintense signal on T2-weighted images in subcutaneous fat or surrounding muscles (Fig. 3). Also bony remodelling (10%) and peroneal nerve palsy (10%) were shown in three cases each. Bony remodelling involved the medial aspect of tibial metaphysis in all 3 cases (Fig. 4). All 3 patients who had nerve involvement complained of drop foot. Two ganglion cysts occurred around fibular neck, so deep peroneal nerve was minimally displaced by ganglion cyst on MR imaging. Another cyst arose along the tract of common peroneal nerve; the former showed abnormal hyperintense signal in tibialis anterior and extensor hallucis longus muscles on T2-weighted images without signal change on T1-weighted images; the latter showed decreased volume with increased fatty strands in tibialis anterior, extensor hallucis longus, and peroneus muscles on T1- and T2-weighted images (Fig. 5).

Pericystic edema in a 54-year-old woman with a ganglion cyst. Axial T2-weighted image (TR/TE: 2375 ms/100 ms) shows a ganglion cyst in vastus medialis muscle. There is a band-like hyperintense signal halo (arrowheads) around the ganglion cyst (arrow)

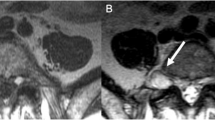
Bony remodelling in a 27-year-old woman with a ganglion cyst. a Plain radiograph shows bony remodelling (arrow) with minimal cortical thickening in the medial epi-metaphysis of tibia. b Axial T1-weighted image (TR/TE: 475 ms/20 ms) shows a low signal intensity cyst (arrowheads) at the site of bony remodelling

Common peroneal nerve palsy in a 13-year-old girl with a ganglion cyst. a Coronal T2-weighted image (TR/TE: 2100 ms/90 ms) shows a high signal intensity, tubular mass (arrowheads) through the common peroneal nerve tract. b Axial T1-weighted image (TR/TE: 520 ms/20 ms) reveals decreased volume with high signal intensity fatty strands in tibialis anterior, extensor hallucis longus, and peroneus muscles, suggesting muscle atrophy (arrowheads). The ganglion cyst (arrow) is seen around fibular neck
Two cases recurred in same location of previous mass, superomedial and inferolateral portions. These 2 cases had continuous channel to the knee and tibiofibular joints; however, we did not perform follow-up MR imaging study, and 2 cases with nerve involvement were improved in symptom after surgery. The symptoms were not improved in another case, which had nerve involvement with ganglion cyst along the common peroneal nerve. Also, this case was one of two recurrences after surgery.
Discussion
A ganglion cyst is generally considered as a benign tumor-like mass rather than a tumor, because it is not the product of proliferating cells. This cyst contains clear high viscous fluid within dense fibrous connective tissue wall without lining with synovial cells. The exact pathogenesis of ganglion cysts is controversial. Most authors report that ganglion cysts result from myxoid degeneration of connective tissues because they are usually located in the areas under continuous physical stress, such as around joints, ligaments, tendons, and periosteum, as well as within bone [1, 16, 17, 18]. With repeated activity across these areas, the collagen tissue undergoes mucoid degeneration resulting in formation of amorphous gelatinous material. Some authors postulated that the cysts resulted from displacement of synovial tissue during embryogenesis [1, 16, 17, 18]. Another theory is that ganglion cysts arise from the articular capsule, resulting in migration of synovial fluid to form the cysts, sometimes along a neurovascular bundle that enters the joint [13].
Ganglion cysts may be located near the joint or at variable distance from the joint capsule. So occasionally, it is not easy to differentiate ganglion cysts from the cystic lesions arising in periarticular area. Malghem et al.'s study showed that a communication between various ganglion cysts of the knee and the joint cavity could be revealed on arthrography by performing delayed radiography after injection of contrast medium [14]. This finding favors the pathogenetic hypothesis of an articular origin of the ganglion material. Arthrographic evidence of communication between the cyst and the joint cavity may be important for two reasons. Firstly, diffusion of intra-articular fluid within the cystic mass is diagnostic and enables exclusion of other diagnostic hypotheses. Secondly, when surgical resection of the cyst is planned, identification of the pedicle is important to perform its excision and to diminish the risk of recurrence. Although arthrography may give a discomfort to patients as an invasive technique, MR imaging reveals excellent image without such discomfort. Our MR study revealed this communication between the cyst and the joint cavity in 66.7% on MR imaging. We speculated that this limitation was caused by wide section thickness and limited sectional plane as well as replacement by fibrous tissue.
The description of whether this channel is present or not, or which direction the channel has, provides a guide for the treatment of ganglion cyst. In our cases, a ganglion cyst with common peroneal nerve involvement recurred; however, we could not perform the evaluation of the difference of the effect between the ligation of the channel and non-ligation of the channel clinically. Some authors have reported that ligation of this channel is helpful for the treatment of recurrent ganglion cyst with nerve involvement [19, 20]. The MR images performed in multi-direction can give us more detailed information of the channel, such as the direction and connection with the joint cavity.
As several articles have been described, occasionally ganglion cysts are associated with secondary changes in surrounding tissues [7, 8, 9, 10, 11]. Also, in our study, secondary changes in surrounding tissue were demonstrated in 15 cases: pericystic edema (n=9); bony remodelling (n=3); and nerve involvement (n=3). Pericystic edema appeared as a halo around the ganglion cyst. To our knowledge, there is not any report about pericystic edema in ganglion cyst. It was considered that this finding might be a secondary change by trauma because ganglion cysts usually occurred in areas under continuous physical stress. Another hypothesis may be that this edema resulted from the diffusion of water through the thin membrane of the cyst when it is under pressure. Ganglion cysts were rarely associated with bony erosion or periosteal reaction, especially periosteal ganglion. In our study, 3 cases had bony remodelling. Periosteal ganglion cyst may produce cortical erosion, scallopping and reactive bone formation without any intraosseous component. These periosteal ganglion cysts in the knee were found over the proximal metaphysis of the tibia. Plain radiography is good for the detection of these erosions. But these bony remodellings may be irregular and may appear as multilocular, with thick spicules of reactive periosteal bone extending from the scalloped area [7, 8, 15]. These radiographic appearances can mimic those of other benign surface tumors that erode the cortex, such as periosteal chondroma, cortical desmoid, and subperiosteal aneurysmal bone cyst. In these complex situations MR imaging can demonstrate the causative ganglion cyst of bony erosion, so it is the most exact modality in diagnosing periosteal ganglion differentially.
Ganglion cysts rarely compress adjacent nerve, causing nerve palsy [9, 10, 11]. But our study revealed 3 cases of peroneal nerve palsy with clinical and EMG evidence. Usually, ganglion cysts around the knee compress the common peroneal nerve, such as ganglion cysts from the proximal tibiofibular joint and intraneural ganglion. Four alternative pathomechanisms of peroneal nerve palsy have been proposed [21]: (a) stretching of nerve by the ganglion; (b) compression between the fibular neck and the peroneus longus muscle and fascia; (c) compression against the tight proximal edge of the peroneus longus muscle and fascia; and (d) compression against the fibular head. In our cases, 3 cases with nerve involvement arose from proximal tibiofibular joint. Two of them were located around fibular neck and stretched deep peroneal nerve; another arose around fibular neck and extended through common peroneal nerve tract, presenting intraneuronal ganglion cyst.
Conclusion
Magnetic resonance imaging is a useful imaging modality to evaluate the associated findings in extra-articular soft tissue ganglion cysts around the knee. It reveals the exact location of them for surgery. The MR image of channels and associated findings with ganglion cysts were detected more frequently than other cystic masses around the knee. These associated findings of pericystic edema, periosteal reaction, and nerve involvement are more common than other cystic lesions around the knee joint, so these associated findings may be useful for the differentiation from other cystic masses around the knee.
References
Bui-Mansfield LT, Youngberg RA (1997) Intraarticular ganglion of the knee: prevalence, presentation, etiology, and management. AJR 168:123–127
Kang CN, Kim DW, Kim DJ et al. (1999) Intra-articular ganglion cysts of the knee. Arthroscopy 15:373–378
Brown MF, Dandy DJ (1990) Intra-articular ganglia in the knee. Arthroscopy 6:322–323
Kim MG, Kim BH, Choi JA et al. (2001) Intra-articular ganglion cysts of the knee: clinical and MR imaging features. Eur Radiol 11:834–840
Butler MG, Fuchigami KD, Chako A (1996) MRI of posterior knee masses. Skeletal Radiol 25:309–317
Narvaez JA, Narvaez J, Aguilera C, Lama E de, Portabella F et al. (2001) MR imaging of synovial tumors and tumor-like lesions. Eur Radiol 11:2549–2560
Valls R, Melloni P, Darnell A et al. (1997) Diagnostic imaging of tibial periosteal ganglion. Eur Radiol 7:70–72
Abdelwahab IF, Kenan S, Hermann G et al. (1993) Periosteal ganglia: CT and MR imaging features. Radiology 188:245–248
Coakley FV, Finlay DB, Harper WM et al. (1995) Direct and indirect MRI findings in ganglion cysts of the common peroneal nerve. Clin Radiol 50:168–169
Kabukcuoglu Y, Kabukcuoglu F, Kuzgun U et al. (1997) Compression neuropathy of the peroneal nerve caused by a ganglion. Am J Orthop 26:700–701
Uetani M, Hashmi R, Hayashi K et al. (1998) Peripheral nerve intraneural ganglion cyst: MR findings in three cases. J Comput Assist Tomogr 22:629–632
Kligman M, Roffman M (1998) Urografin injection demonstrated soft tissue ganglion communication with an intraosseous ganglion cyst. Bull Hosp Joint Dis 57:96–98
Buckwalter JA, Dryer RF, Mickelson MR (1979) Arthrography in juxta-articular cysts of the knee: two cases diagnosed by delayed roentgenograms. J Bone Joint Surg Am 61A:465
Malghem J, van de Berg BC, Lebon C et al. (1998) Ganglion cysts of the knee: articular communication revealed by delayed radiography and CT after arthrography. AJR 170:1579–1583
de Maeseneer M, de Boeck H, Shahabpour M et al. (1999) Subperiosteal ganglion cyst of the tibia: a communication with the knee demonstrated by delayed arthrography. J Bone Joint Surg Br 81:643–646
Angelides AC, Wallace PF (1976) The dorsal ganglion of the wrist: its pathogenesis, gross and microscopic anatomy and surgical treatment. J Hand Surg Am 1:228–235
Kobayashi H, Kotoura Y, Hosono M et al. (1996) Periosteal ganglion of the tibia. Skeletal Radiol 25:381–383
Rozbruch SR, Chang V, Bohne WH et al. (1998) Ganglion cysts of the lower extremity: an analysis of 54 cases and review of the literature. Orthopedics 21:141–148
Spinner RJ, Atkinson JL, Harper CM Jr et al. (2000) Recurrent intraneural ganglion cyst of the tibial nerve: a case report. J Neurosurg 92:334–337
Dubuisson AS, Stevenaert A (1996) Recurrent ganglion cyst of the peroneal nerve: radiological and operative observations. A case report. J Neurosurg 84:280–283
Harbaugh KS, Tiel RL, Kline DG (1997) Ganglion cyst involvement of peripheral nerves. J Neurosurg 87:403–408
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kim, JY., Jung, SA., Sung, MS. et al. Extra-articular soft tissue ganglion cyst around the knee: focus on the associated findings. Eur Radiol 14, 106–111 (2004). https://doi.org/10.1007/s00330-003-1969-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-003-1969-6