
Abstract
Osteonecrosis of the femoral head is considered to occur early during the course of corticosteroid treatment. However, it remains unclear exactly how early it can develop after initiation of corticosteroid treatment. We report a case of osteonecrosis of the femoral head in which abnormal findings were observed on short-tau inversion recovery (STIR) sequence image performed 2 weeks and 4 days after initiation of high-dose corticosteroid therapy. A 45-year-old man with hemophagocytic syndrome was started on prednisolone, with a maximum dose of 40 mg/day. On day 13 after initiation of this corticosteroid therapy, he transiently experienced left hip pain with no apparent cause. STIR sequence image 5 days after the onset of pain revealed high-intensity bone marrow lesions at the femoral neck of both hips. At 3 months after initiation of corticosteroid therapy, T1-weighted magnetic resonance imaging revealed concave-shaped low-intensity bands, which corresponded to the preceding high-intensity lesions on both hips. Because of the subsequent progression to collapse of the left femoral head, he underwent prosthetic replacement surgery. The high-intensity lesions on STIR sequence image indicate the possibility that osteonecrosis can occur within 3 weeks after initiation of high-dose corticosteroid therapy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Nontraumatic osteonecrosis of the femoral head (ONFH) is often caused by high-dose corticosteroid therapy [1, 2]. An osteonecrotic lesion is usually represented as a concave-shaped low-intensity band on T1-weighted magnetic resonance imaging (MRI), which is attributed to the reparative reaction at the interface between necrotic and living bones [3, 4]. This low-intensity band has been reported to be observed on MRI around 6 weeks after initiation of corticosteroid therapy [3].
On the other hand, although several studies suggested that ONFH may occur early during the course of corticosteroid treatment, it remains unclear exactly how early it can develop after initiation of corticosteroid treatment [5–7]. Considering the passage to which the bone infarction occurs before the bone repair of the necrotic lesion, some abnormal findings indicating the bone infarction can be observed on MRI performed before the appearance of a low-intensity band.
We describe a case of ONFH in which high-intensity bone marrow lesions were observed on short-tau inversion recovery (STIR) MRI performed 2 weeks and 4 days after initiation of high-dose corticosteroid therapy.
Case report
A 45-year-old man (height 173 cm, weight 83 kg, body mass index 27.7 kg/m2) with hemophagocytic syndrome had been started on corticosteroid treatment with a maximum prednisolone dose of 40 mg/day (Fig. 1). He had an alcohol intake habit (consuming 298 g ethanol per week for the past 20 years). There was no history of traumatic hip injury or congenital hip disease.

A 45-year-old man with hemophagocytic syndrome had been started on corticosteroid treatment with a maximum prednisolone dose of 40 mg/day for 17 days (40 mg/day × 5 days; 20 mg/day × 3 days; 15 mg/day × 3 days; 10 mg/day × 3 days; 5 mg/day × 3 days)
On day 13 after initiation of corticosteroid therapy, he transiently experienced left hip pain with no apparent cause. The pain disappeared 4 days later without treatment. An anteroposterior radiograph obtained on that day showed no apparent abnormalities in the femoral head. He underwent 1.5-T system MRI examination (Philips; Achieva) 5 days after the onset of pain (2 weeks and 4 days after corticosteroid treatment was initiated), where T1-weighted images [repetition time/echo time (TR/TE) = 400–800/shortest ms] and STIR images (TR/TE = 2500–7500/60 ms) in the coronal and axial planes were obtained. T1-weighted MRI showed no obvious abnormalities, whereas STIR MRI indicated high-intensity bone marrow lesions at the femoral neck of both hips (Fig. 2). At 3 months after initiation of corticosteroid therapy, he again experienced left hip pain. T1-weighted MRI showed concave-shaped band lesions, which corresponded to the preceding bone marrow lesions on both hips (Fig. 3).

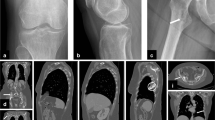
Magnetic resonance imaging (MRI) performed 5 days after the onset of left hip pain. a Coronal T1-weighted imaging [repetition time/echo time (TR/TE) 489/11 ms] reveals no abnormalities on either hip; b coronal short-tau inversion recovery (STIR) sequence image (TR/TE 2500/60 ms) reveals high-intensity bone marrow lesions at the femoral neck on both hips (white arrows)

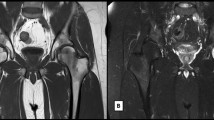
Magnetic resonance imaging (MRI) performed 3 months after initiation of corticosteroid therapy. a Coronal T1-weighted imaging (TR/TE 489/11 ms) shows concave-shaped low-intensity-band lesions, which corresponded to the preceding high-intensity lesions on both hips; b coronal short-tau inversion recovery (STIR) sequence image (TR/TE 2500/60 ms) shows demarcating high-intensity-band lesions of both hips
Based on these findings, the patient was diagnosed with ONFH. He was started on nonsurgical conservative therapy, including avoidance of weight-bearing. The hip pain did not resolve, however, and an anteroposterior radiograph obtained 4 months after initiation of corticosteroid therapy showed collapse of the left femoral head (Fig. 4). He therefore underwent prosthetic replacement surgery (1 year after initiation of corticosteroid therapy).

Radiographs of the left hip joint obtained 4 months after starting corticosteroid therapy. a Anteroposterior radiograph shows collapse of the left femoral head (white arrows); b lateral radiograph (Lauenstein view) shows collapse of the left femoral head (white arrows)
The pathology of the resected femoral head confirmed the diagnosis of ONFH. The bone marrow lesions histologically corresponded to repair tissue that had formed between the necrotic and reparative areas [8].
Discussion
The earliest appearance of a low-intensity band on T1-weighted image characteristic of ONFH has been reported to be observed around 6 weeks after initiation of corticosteroid therapy [3]. Also, in a case series with renal allograft recipients, a faint high-intensity lesion on fat suppression imaging preceded a later band lesion at 5 and 6 weeks after initiation of corticosteroid therapy in 20 % (4/20) of the patients who developed ONFH [4]. They hypothesized that these focal abnormal pattern was produced by leakage of the blood from impaired blood vessels in the necrotic area [4, 9]. In the current patient, slight high-intensity bone marrow lesions were observed on STIR MRI at 2 weeks and 4 days after initiation of corticosteroid therapy, which subsequently seemed to precede the typical low-intensity band. We suppose that the early changes observed on STIR might indicate a very early reaction to the occurrence of osteonecrosis.
High-dose corticosteroid therapy has been considered to be related to the development of ONFH [1, 2]. Concerning the etiology of steroid-induced ONFH, several mechanisms have been reported, including compartment syndrome, thrombosis, fat embolism, and vasospasm [10–13]. In addition, the molecular mechanism of steroid-induced ONFH has recently been reported, describing the importance of increased adipogenesis by the differentiation pathway of osteoprogenitor cells, decreased angiogenesis, inhibition of osteogenic gene expression, and proliferation of bone marrow stem cells [14].
In osteonecrosis, a concave-shaped low-intensity band on T1-weighted images has been considered to correspond to the reparative tissue against osteonecrosis, which histopathologically consists of appositional bone and fibrous granulation tissue. The low-intensity band has thus been included in the diagnostic criteria of ONFH [3, 15]. On the other hand, slight high-intensity bone marrow lesions on STIR observed in the case reported herein were so faint, and therefore the diagnostic utility of these early changes on STIR seems to be limited.
Recently, several animal studies have shown the possible effects of drugs in preventing corticosteroid-induced osteonecrosis, including an anticoagulant, a lipid-lowering drug, 3-hydroxymethyl-3-glutaryl-CoA (HMG-CoA) reductase inhibitor, an antiplatelet drug, and an antivasospasm drug [11, 13, 16, 17]. When applying these drugs in the clinical setting to prevent ONFH development, the timing of their administration would be important. Considering the possible occurrence of osteonecrosis within a few weeks after initiating corticosteroid therapy in our patient, a prophylactic drug should be administered as soon as practicably possible after initiating corticosteroid therapy.
In the current case, the patient had an alcohol intake habit (consuming 298 g ethanol per week for the past 20 years). Hirota et al. [18] reported a significant dose–response relation between weekly alcohol consumption and the development of ONFH. In comparison, our patient would be classified as belonging to a group with the lowest alcohol intake. In addition, in a case–control study, Fukushima et al. [19] concluded that the added effect of alcohol intake was too small to make any significant difference in the presence of the overwhelming effect of steroids. Considering both the small dose of alcohol and the history of corticosteroid use in our case, we hypothesized that ONFH of both hips was influenced by the corticosteroid.
In conclusion, the early bone marrow changes of the femoral head were observed within 3 weeks on STIR MRI, indicating that osteonecrosis can occur within 3 weeks after starting high-dose corticosteroid therapy.
References
Oinuma K, Harada Y, Nawata Y, Takabayashi K, Abe I, Kamikawa K, Moriya H (2001) Osteonecrosis in patients with systemic lupus erythematosus develops very early after starting high dose corticosteroid treatment. Ann Rheum Dis 60(12):1145–1148
Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y (2010) Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res 468(10):2715–2724
Kubo T, Yamazoe S, Sugano N, Fujioka M, Naruse S, Yoshimura N, Oka T, Hirasawa Y (1997) Initial MRI findings of non-traumatic osteonecrosis of the femoral head in renal allograft recipients. Magn Reson Imaging 15(9):1017–1023
Fujioka M, Kubo T, Nakamura F, Shibatani M, Ueshima K, Hamaguchi H, Inoue S, Sugano N, Sakai T, Torii Y, Hasegawa Y, Hirasawa Y (2001) Initial changes of non-traumatic osteonecrosis of femoral head in fat suppression images: bone marrow edema was not found before the appearance of band patterns. Magn Reson Imaging 19(7):985–991
Shimizu K, Moriya H, Akita T, Sakamoto M, Suguro T (1994) Prediction of collapse with magnetic resonance imaging of avascular necrosis of the femoral head. J Bone Joint Surg Am 76(2):215–223
Kokubo T, Takatori Y, Ninomiya S, Nakamura T, Kamogawa M (1992) Magnetic resonance imaging and scintigraphy of avascular necrosis of the femoral head: prediction of subsequent segmental collapse. Clin Orthop Relat Res 277:54–60
Takatori Y, Kokubo T, Ninomiya S, Nakamura S, Morimoto S, Kusaba I (1993) Avascular necrosis of the femoral head: natural history and magnetic resonance imaging. J Bone Joint Surg Br 75(2):217–221
Yamamoto T, DiCarlo EF, Bullough PG (1999) The prevalence and clinicopathological appearance of extension of osteonecrosis in the femoral head. J Bone Joint Surg Br 81(2):328–332
Sakai T, Sugano N, Tsuji T, Miyazawa T, Nakamura N, Haraguchi K, Ochi T, Ohzono K (1999) Contrast-enhanced magnetic resonance imaging in a nontraumatic rabbit osteonecrosis model. J Orthop Res 17(5):784–792
Ficat RP (1985) Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br 67(1):3–9
Motomura G, Yamamoto T, Miyanishi K, Jingushi S, Iwamoto Y (2004) Combined effects of an anticoagulant and a lipid-lowering agent on the prevention of steroid-induced osteonecrosis in rabbits. Arthritis Rheum 50(10):3387–3391
Jones JP Jr (1993) Fat embolism, intravascular coagulation, and osteonecrosis. Clin Orthop Relat Res 292:294–308
Ikemura S, Yamamoto T, Motomura G, Yamaguchi R, Zhao G, Iwasaki K, Iwamoto Y (2013) Preventive effects of the anti-vasospasm agent via the regulation of the Rho-kinase pathway on the development of steroid-induced osteonecrosis in rabbits. Bone 53(2):329–335
Seamon J, Keller T, Saleh J, Cui Q (2012) The pathogenesis of nontraumatic osteonecrosis. Arthritis. doi:10.1155/2012/601763
Sugano N, Atsumi T, Ohzono K, Kubo T, Hotokebuchi T, Takaoka K (1999) Diagnostic criteria for non-traumatic osteonecrosis of the femoral head. A multicentre study. J Bone Joint Surg Br 81(4):590–595
Nishida K, Yamamoto T, Motomura G, Jingushi S, Iwamoto Y (2008) Pitavastatin may reduce risk of steroid-induced osteonecrosis in rabbits: a preliminary histological study. Clin Orthop Relat Res 466(5):1054–1058
Yamaguchi R, Yamamoto T, Motomura G, Ikemura S, Iwasaki K, Zhao G, Iwamoto Y (2012) Effects of an anti-platelet drug on the prevention of steroid-induced osteonecrosis in rabbits. Rheumatology (Oxford) 51(5):789–793
Hirota Y, Hirohata T, Fukuda K, Mori M, Yanagawa H, Ohno Y, Sugioka Y (1993) Association of alcohol intake, cigarette smoking, and occupational status with the risk of idiopathic osteonecrosis of the femoral head. Am J Epidemiol 137(5):530–538
Fukushima W, Yamamoto T, Takahashi S, Sakaguchi M, Kubo T, Iwamoto Y, Hirota Y (2013) Idiopathic ONFH multicenter case–control study. The effect of alcohol intake and the use of oral corticosteroids on the risk of idiopathic osteonecrosis of the femoral head: a case–control study in Japan. Bone Joint J Br 95(3):320–325
Acknowledgments
This work was partially supported by a Research Grant for Intractable Diseases from Japan Agency for Medical Research and Development, AMED (H26-Itaku(Nan)-Ippan-031).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Informed consent
The patient was fully informed that his data would be submitted for publication, and he gave his consent.
Rights and permissions
About this article

Cite this article
Kubo, Y., Yamamoto, T., Motomura, G. et al. MRI-detected bone marrow changes within 3 weeks after initiation of high-dose corticosteroid therapy: a possible change preceding the subsequent appearance of low-intensity band in femoral head osteonecrosis. Rheumatol Int 35, 1909–1912 (2015). https://doi.org/10.1007/s00296-015-3346-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-015-3346-6