
Abstract
To compare the efficacy of the addition of clarithromycin (CM) to methotrexate (MTX) and methylprednisolone (MP) in active rheumatoid arthritis (RA). 32 patients with RA consecutively randomized. Control group: sixteen patients treated for 24 months with MTX 10–15 mg i.m. weekly and MP 4–6 mg daily. CM group: sixteen patients treated with MTX 10–15 mg i.m. weekly and MP 4–6 mg daily for 24 months; CM therapy added in the first month (500 mg twice a day for the first 15 days followed by 500 mg a day for the remaining 15 days). Evaluation of the improvement following ACR criteria was performed at months 1 (primary endpoint), 3 and 6. Patients were furthermore observed after 12, 18 and 24 months from the study beginning. At month 1, following ACR70 improvement criteria, we found a significant additive value in CM group (10/16 = 63 % vs 4/16 = 25 %, p = 0.033—chi-square test). After discontinuation of CM, the difference between groups was anymore evident (month 3: CM group 10/16 = 63 % vs control group 9/16 = 56 %). At month 24, 7/16 (44 %) in control group and 12/16 (75 %) in CM group completed the follow-up. The addition of CM to MTX and MP can induce the remission ACR 70 in the majority of RA patients within 4 weeks, while MTX and MP alone need about 3 months to achieve the same result.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
It is known that clarithromycin (CM) has an anti-inflammatory action [1]; indeed, some clinical studies reported the use of CM in treating rheumatic diseases. In an open uncontrolled pilot study [2] on the use of CM in rheumatoid arthritis (RA), eighteen patients unresponsive to disease modifying anti-rheumatic drugs (DMARDs) were treated with CM for six months and successful results were obtained in 10 patients (56 %). In this study, CM showed a very rapid onset of action (10 days) as well as an ability to lower the plasma levels of soluble type II phospholipase and prostaglandin E2. More recently, CM efficacy was further confirmed in a double-blind trial versus placebo performed in 81 RA patients [3]. In 2006, Moskowitz published a report on seven patients affected by undifferentiated connective tissue disease who were successfully treated with CM in a 12-week open-label study. Also in this case, CM showed a very rapid onset of action [4]. In 2010, we have described the beneficial effect of CM in the adult onset Still’s disease (AOSD), a rare rheumatologic condition characterized by an acute systemic involvement. A small cohort of patients (n = 6) was treated by adding CM to a therapy with DMARDs and glucocorticoids (GC). After 6 months of therapy, 5 out of the 6 treated patients reached an ACR 70 improvement and stopped all therapies in 6–18 months. The clinical outcome achieved with the use of CM was very close to that obtained with anakinra [5, 6]. Other single cases of AOSD have been also successfully treated with CM [7, 8].
In the present study, we report the results of a randomized pilot study planned to compare the efficacy of CM added to methotrexate (MTX) and low-dose methyl-prednisolone (MP) for the treatment of active RA.
Objective
The primary objective of the study was to evaluate the efficacy of CM added to i.m. MTX and low-dose MP in active RA. The clinical outcome was measured after 1 month of therapy. Secondary objective was to evaluate the activity of the disease after 3 and 6 months of treatment. Patients were furthermore observed after 12, 18, and 24 months from the study beginning to evaluate the persistence to the therapy.
Methods
Participants
The present study was carried out at the Rheumatology and Rehabilitation Unit of the Salvatore Maugeri Foundation IRCCS in Castel Goffredo, Mantua, Italy, and at the Rheumatology Unit of the New Hospital San Giovanni di Dio, Florence, Italy.
The protocol was approved by an independent Ethics Committee (Comitato Etico Centrale of Salvatore Maugeri Foundation, Pavia) and all the enrolled patients gave their written, informed consent to participate in the study. Consensus was obtained according to the declaration of Helsinki and subsequent documents.
Inclusion criteria were as follows: male and female patients aged over 18 years affected by active RA, diagnosed according to ACR criteria; GC dose stabilized at 4–6 mg MP since at least 1 month, non-steroidal anti-inflammatory drug (NSAIDs) stabilized since at least 1 month (if present), no intra-articular injections of GC in the last month; DMARDs (if present) stopped at least 3 months before the inclusion in the trial. Moreover, the eligible patients must meet at least three of the following criteria: erythrocyte sedimentation rate (ESR) ≥28 mm, number of tender joints ≥6, number of swollen joints ≥3, morning stiffness ≥45 min.
Exclusion criteria were as follows: RA patients in functional class ACR IV; affected by active hepatic, renal, cardiovascular, or neoplastic diseases; presence of systemic active diseases; psychiatric or neurologic diseases; acute or chronic inflammatory diseases other than RA; drug or alcohol users; allergy to macrolide antibiotics or MTX; treatment with drugs interfering with CM or MTX (cyclosporine A, antihistaminic, carbamazepine, folic acid, statins), pregnancy or feeding.
Study design
This study is a randomized, single-blind pilot study. Controlled double-blind study versus placebo was not feasible due to the metallic taste of CM that was expected to early invalidate the blinding of the study. Indeed, it has been proved that metallic taste following CM use occurs in about 50 % of treated patients after a few days of therapy [3, 5, 9]. To preserve blinding, evaluation of patient outcome was performed by a physician blinded to the treatment.
Thirty-two patients were consecutively randomized in 1:1 ratio into two groups (control group and CM group). A randomization list was electronically generated according to a complete randomized design with block size of four units and managed by the principal investigator who was responsible for assigning participants to interventions.
Control group was treated with i.m. MTX 10–15 mg weekly and MP 4–6 mg daily for 24 months.
CM group was treated with i.m. MTX 10–15 mg weekly and MP 4–6 mg daily for 24 months. During the first month (in CM group), patients were administered with CM treatment according to the following scheme: CM 500 mg twice a day for the first 15 days and 500 mg once a day for the remaining 15 days.
During the study period, neither intra-articular infiltrations of GC nor modification in NSAIDs treatment (if present) was allowed.
All patients were evaluated at baseline and at 1, 3, 6, 12, 18, and 24 months thereafter. The following parameters were monitored: number of tender joints, number of swollen joints, morning stiffness in minutes, pain measured on a 10-cm-long horizontal visual analogic scale (VAS); global self-assessment of efficacy expressed separately by the physician and the patient using a 10-cm-long horizontal VAS scale. Patients also underwent standard urine test and blood tests to determine the following parameters: ESR, C-reactive protein (CRP), rheumatoid factor (RF), hemochrome, glycemia, transaminase, alkaline phosphatase, gamma-glutamyltransferase, creatininemia, calcemia, creatine-kinase. Anti-nuclear antibody was tested at the baseline only. Moreover, a plane X-ray of the hands was performed, whenever needed. The consolidated standards of reporting trials (CONSORT) recommendations were followed in reporting the results of this study [10].
Collection and storage of samples
Blood samples were drawn using standard venipuncture technique between 08:00 and 09:00 a.m. after overnight fasting. Peripheral venous blood was drawn into sterile vacuum blood collection tubes without any additives for serum samples and into potassium EDTA vacutainer tubes for plasma samples (Becton–Dickinson, San Jose, CA, USA). After division into aliquots, serum and plasma samples were immediately analyzed or frozen and stored at −80 °C until assay and were thawed only once.
Urine samples were collected at the same time in the morning and a standard urine analysis performed.
Biochemical measurements
Erythrocyte sedimentation rate (ESR) was measured on the automatic instrument Ves-Matic 20 (DIESSE—Diagnostica Senese, Siena, Italy). The ESR reading at the first hour is performed in 26 min including the mixing of samples.
C-reactive protein and RF levels were measured using commercially available kits (Olympus Diagnostic, Italy) run on an Olympus AU400® chemistry autoanalyser (OLYMPUS Instruments, Japan), according to the manufacturer’s protocol. The published analytical sensitivity of the CRP assay is 0.14 mg/l, with reported intra-assay and inter-assay coefficients of variation of 3.22 and 3.8 %, respectively, at a CRP concentration of 6.6 mg/l. The within run precision of the RF assay is less than 5 % CV or SD < 1 IU/mL, and the total precision is less than 10 % CV or SD < 3 IU/mL.
Monitoring of toxicity
All patients were explicitly requested to report on any eventual side effect at each visit.
Statistical analysis
Primary endpoint of the study was the ACR 70 measure after 1 month of treatment. Other measures of disease activity (ACR 20, ACR 50 at month 1 and ACR 20, ACR 50, ACR 70 at month 3 and 6) were analyzed as secondary endpoints of the study. Patients were furthermore observed after 12 and 24 months from the study beginning to evaluate the persistence to the treatment.
Percentages of subject achieving ACR 20, ACR 50, and ACR 70 at different time points (month 1–month 6) in the two groups were compared by using a chi-square test.
Descriptive statistics were calculated for all the recorded variables, reporting means and standard deviations for continuous normally distributed variables, medians, and interquartile ranges for ordinal variables, frequencies for categorical or qualitative variables. Comparison of baseline characteristics between groups were tested by applying Student’s t test (normally distributed variables), Mann–Whitney U test (ordinal variables), chi-square test, or Fisher exact test (categorical and qualitative variables). Data were analyzed using SPSS statistical software.
Results
Patient enrollment was carried out between October 2005 and August 2008
Control group consisted of 16 patients, 3 males and 13 females, mean age 68 (35–82 years); CM group consisted of 16 patients, 4 males and 12 females, mean age 61 (19–80 years).
Baseline characteristics of the enrolled patients are shown in Table 1.
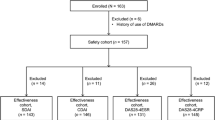
In control group, 13/16 patients (81 %) completed the 6-month follow-up, 11/16 patients (69 %) completed the 12-month follow-up, but only 7/16 (44 %) were still on treatment at 24 months (Fig. 1).

Persistence to the therapy in both groups
The reasons for withdrawal were as follows: inefficacy of the treatment (4 patients), alopecia (2 patients), severe transaminase increase (1 patient) related to MTX. Moreover, one patient stopped the treatment because of heart failure and one patient because of sudden death, being both events unrelated to treatment.
In CM group, 15/16 (94 %) patients completed the 6-month follow-up, 14/16 (88 %) patients completed the 12-month follow-up, and 12/16 (75 %) patients completed the 24-month follow-up (Fig. 1).
The reasons for withdrawal were unrelated to treatment in 3 cases: stroke (1 patient), heart surgery (1 patient), anxiety (1 patient). One more patient stopped the treatment because of a myelodisplasic syndrome which could possible be related to MTX.
Side effects in both groups are shown in Table 2.
Efficacy results are shown in Fig. 2.

Improvement in both groups following ACR criteria during 12 months of follow-up
In detail:
-
In control group, 14/16 reached ACR 20, 12/16 ACR 50, 4/16 ACR 70 (25 %) at month 1.
-
In CM group, 16/16 patients reached ACR 20, 14/16 ACR 50, and 10/16 ACR 70 (61 %) at month 1.
Comparison between the two groups (chi-square test, p = 0.033) showed a significant additive value of CM in clinical disease improvement. After discontinuation of CM (at months 3 and 6), no statistical difference between groups was anymore pointed out (Fig. 2).
Discussion
Antibacterial drugs play a historical role in the therapy of RA. Sulfasalazyn, a drug containing sulfapyridine, has been the most used DMARD in North Europe for a long time. Minocycline and doxycycline have also been used [11]. More recently, other antibiotics have been proposed for the treatment of RA: roxithromycin, levofloxacin, and ornidazole [12].
At least two different possible mechanisms of action can explain the efficacy of CM in RA: (1) the anti-inflammatory effect and (2) the antimicrobial action.
The finding that CM can exert an anti-inflammatory effect was reported both in preclinical and clinical studies, even if the anti-inflammatory mechanism of action of CM is still unclear. The response of diffuse panbronchiolitis and other chronic respiratory infections following long-term macrolide therapy is an example of the antiinflammatory and immunomodulatory activities of CM. In addition, CM has been shown to inhibit the production of interleukin-1 β (IL-1β) and α-tumor necrosis factor (TNFα) in the lungs, to modulate cell mediator release and survival as well as interleukin-8 (IL-8) levels in chronic sinusitis and asthma [13–16]. Finally, CM is effective in the treatment of relapsed/refractory myeloma, showing synergy with immunomodulatory drugs [17–19]. Since B lymphocytes are the cells involved in the pathogenesis of myeloma, we could hypothesize that B cells are the target of the anti-inflammatory activity of CM.
The idea that CM is effective in RA because of its antibacterial activity was firstly proposed by Ogrendik [3]. He hypothesized that the oral anaerobic bacteria could play an important role in the ethiopathogenesis of RA. Indeed, he proposed that CM efficacy could be related to its antibiotic activity against Gram-negative anaerobic bacteria considered responsible of the periodontitis [3, 11]. This hypothesis is also supported by other authors [20, 21] according to whom periodontopathic bacteria could contribute to the development of an autoimmune process leading to RA. This assumption could also explain why the association of immunosuppressant drugs (MTX and GC) with CM leads to a more efficacious improvement of RA.
In the present study, we demonstrated that the addition of CM to standard therapy in the first month of treatment significantly improves active RA. Noteworthy, the rapid onset of CM beneficial effect has to be underlined. This finding is in agreement with previous studies [2–5] and supports the hypothesis that CM action is able to get the disease remission in a shorter therapy time frame. The efficacy of CM can also be explained by looking at the action of other drugs in the same class of immunosuppressant macrolide antibiotics such as sirolimus, everolimus, and tacrolimus. Indeed, these drugs have been successfully used in the treatment of RA, particularly tacrolimus, approved in Japan for the treatment of RA since 2005 [22–24].
However, the study has some limitations, being the small number of patients (due to the pilot nature of the study) and single-blind method the major ones. A double-blind study involving a large sample of patients is needed in order to draw definitive conclusion concerning CM efficacy in RA.
Concerning side effects of CM, it is clear that a CM extended use could cause antibiotic resistance on bacteria. Moreover, CM could cause irreversible sensorineural ototoxicity [25]. Other side effects of CM are usually not serious, being the metallic taste the most common one, sometimes worsening during the treatment and probably explainable by the high levels of CM in the gums [9]. The present study suggests that a 4-week CM cycle added to the current treatment is efficacious in inducing the remission of the disease (or in case of flare). The treatment schedule used in our trial may represent a clinical therapeutic tool to obtain a fast onset of the beneficial clinical effect without exposing patients to severe side effects.
References
Ianaro A, Ialenti A, Maffia P, Sautebin L, Rombolà L, Carnuccio R et al (2000) Anti-inflammatory activity of macrolide antibiotics. J Pharmacol Exp Ther 292:156–163
Saviola G, Abdi-Ali L, Rossini P, Campostini L, Coppini A, Gori M et al (2002) Clarithromycin in rheumatoid arthritis patients not responsive to disease-modifying anti-rheumatic drugs: an open uncontrolled pilot study. Clin Exp Rheum 20:373–378
Ogrendik M (2007) Effects of clarithromycin in patients with active rheumatoid arthritis. Curr Med Res Opin 23:515–522
Moskowitz R, Lesko M, Hooper M (2006) Open-label study of clarithromycin in patients with undifferentiated connective tissue disease. Semin Arthritis Rheum 36:82–87
Saviola G, Benucci M, Abdi Ali L, Baiardi P, Manfredi M, Bucci MR et al (2010) Clarithromycin in adult onset Still’s disease. A study of 6 cases. Rheumatol Int 30(4):555–560. (Epub 2009 Dec 23)
Lequerré T, Quartier P, Roselini D et al (2008) Interleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in France. Ann Rheum Dis 67:302–308
Saviola G, Abdi-Ali L, Shams-Eddin S, Davoli C, Taglietti M (2004) Clarithromycin in adult-onset Still’s disease. Case report with 1 year follow-up. Clin Exp Rheumatol 22:379
Thanou-Stavraki A, Aberle T, Aksentijevich I, Bane BL, Harley JB (2011) Clarithromycin in adult-onset Still’s disease: a potentially useful therapeutic. J Clin Rheumatol 17(7):373–376
Burrel RC, Walters JD (2008) Distribution of systemic clarithromycin to gingiva. J Periodontol 79:1712–1718
Schulz KF, Altman DG, Moher D (2010) CONSORT Group. CONSORT 2010 Statemen: updated guidelines for reporting parallel group randomised trials. J Clin Epidemiol 63(8):834–840
Stone M, Fortin PR, Pacheco-Tena C, Inman RD (2003) Should tetracycline treatment be used more extensively for rheumatoid arthritis? Metaanalysis demonstates clinical benefit with reduction in disease activity. J Rheumatol 30(10):2112–2122
Ogrendik M (2009) Rheumatoid arthritis is linked to oral bacteria. Mod Rheumatol 19(5):453–456. (Epub 2009 Jun 24, Review)
Tamaoki J, Kadota J, Takizawa H (2004) Clinical implications of the immunomodulatory effects of macrolides. Am J Med 117:5S–11S
Borszcz PD, Befus D, Moqbel R, Sin DD, Adamko DJ, Man SFP et al (2005) Effects of clarithromycin on inflammatory cell mediator release and survival. Chemotherapy 51:206–210
Simpson JL, Powell H, Boyle MJ, Scott RJ, Gibson PG (2008) Clarithromycin targets neutrophilic airway inflammation in refractory asthma. Am J Respir Crit Care 177:148–155
Giamarellos-Bourboulis EJ (2008) Immunomodulatory therapies for sepsis: unexpected effects with macrolides. Int J Antimicrob Agents 32(Suppl 1):S39–S43
Morris TC, Kettle PJ, Drake M, Jones FC, Hull DR, Boyd K et al (2008) Clarithromycin with low-dose dexamethasone and thalidomide is effective in relapsed/refractory myeloma. Br J Haematol 143(3):349–354. (Epub 2008 Aug 28)
Gay F, Rajkumar SV, Coleman M, Kumar S, Mark T, Dispenzieri A, Pearse R et al (2010) Clarithromycin (Biaxin)-lenalidomide-low-dose-dexamethasone (BiRd) versus Lenalidomide-low-dose dexamethasone (Rd) for newly diagnosed myeloma. Am J Hematol 85(9):664–669
Nakamura M, Kikukawa Y, Takeya M, Mitsuya H, Hata H (2010) Clarithromycin attenuates autophagy in myeloma cells. Int J Oncol 37(4):815–820
Saviola G, Benucci M, Cirino G (2007) Comments on: effects of clarithromycin in patients with active rheumatoid arthritis. Cur Med Res Opin 23:515–522
Rugter Persson G (2012) Rheumatoid Arthritis and periodontitis-inflammatory and infectious connections. Review of the literature. J Oral Microbiol. Epub 2012 Feb 12
Tanaka Y, Suzuki K, Saito K (2007) Efficacv of tacrolimus for joint destruction in rheumatoid arthritis. Clin Calcium 17(4):593–9. Review
Bruyn GA, Tate G, Caeiro F, Maldonado-Cocco J, Westhovens R, Tannenbaum H et al. (2008) RADD Study Group. Everolimus in patients with rheumatoid arthritis receiving concomitant methotrexate: a 3–month, double blind, randomized, placebo-controlled, parallel-group, poof-of concept study. Ann Rheum Dis 67(8):1090–1095. (Epub 2007 Nov 23)
Sofroniadou S, Goldsmith D (2011) Mammalian target of rapamycin (mTOR) inhibitors: potential uses and a review of haematological adverse effects. Drug Saf 34(2):97–115
Coulston J, Balaratnam N (2005) Irreversible sensorineural hearing loss due to clarithromycin. Postgrad Med J 81:58–59
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Saviola, G., Abdi-Ali, L., Campostrini, L. et al. Clarithromycin in rheumatoid arthritis: the addition to methotrexate and low-dose methylprednisolone induces a significant additive value—a 24-month single-blind pilot study. Rheumatol Int 33, 2833–2838 (2013). https://doi.org/10.1007/s00296-013-2822-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-013-2822-0