
Abstract
The monocyte-derived macrophage is recognized as a critical determinant in biocompatibility, but its appearance in the chronic inflammatory phase is accompanied by the presence of lymphocytes, which have been much less studied in this regard. Here, we first present an overview of the physiologic continuum comprising host reactions to the surgical implantation of biomaterial. Secondly, we describe our collective research efforts, which indicate that lymphocytes are additional and key cellular determinants of biocompatible outcome. Thus, bioengineering advances will require that lymphocyte responses be regarded as integral components of innate inflammatory and immune/immunotoxic cell interactions at sites of biomaterial implantation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The inflammatory and wound healing responses to biomaterials
Overview
The biocompatibility of implanted biomaterials is determined by the degrees to which host homeostatic mechanisms are perturbed during surgical placement of the implant and the extents to which pathological consequences are created from the ensuing inflammatory, wound healing, and foreign body responses to surgical injury. The successful development of novel biomaterials, tissue-engineered constructs, and prostheses will require in-depth mechanistic understanding of the collective foreign body reaction.
Upon surgical implantation of a biomaterial, i.e., the introduction of a foreign body into living host tissue, a series of events ensues that is characterized by blood protein adsorption, the arrival of acute and chronic inflammatory cells, the formation of granulation tissue, the foreign body reaction, and fibrosis or fibrous encapsulation. This is outlined in Table 1. As the collective responses of vascular tissue to injury, this continuum can also be viewed as bimodal. The first phase involves the activation of host mechanisms to limit or neutralize the foreign body. The second phase is characterized by wound healing and attempts to repair and reconstitute the injured tissue at the implant site via the formation of fibroblastic scar tissue, or combinations of both of these processes.
It must be emphasized that the driving force behind this physiological continuum is the persistent presence of a non-phagocytosable foreign body. However, each participating cell type, and this is particularly known to be true for the monocyte-derived macrophage, is differentially influenced by chemically distinct material surfaces and by surface topography. Therefore, to a great extent, it is biomaterial surface chemistry that dictates the degrees to which events in the continuum proceed, ultimately determining the overall biocompatible outcome of each biomaterial application.
Protein adsorption
Biomaterial surface property-dependent blood protein adsorption occurs immediately upon surgical implantation of a biomedical device, and it is therefore this initial event that precedes all subsequent sequelae. Thus, it is the blood protein-modified biomaterial surface that all other host components, including inflammatory and immune leukocytes, encounter and/or interact with as an adhesion substrate [1, 2]. The blood protein-modified biomaterial surface is perhaps more appropriately referred to as a provisional matrix, which, depending on biomaterial surface chemistry, may also contain a milieu of chemokines, cytokines, or other bioactive agents associated with adsorbed blood protein components.
Although monocytes/macrophages express multiple receptors with potential to mediate cell/substrate interactions with blood proteins, we have identified both the β1 and β2 integrin families as necessary and sufficient mediators of adhesion during monocyte-to-macrophage development and foreign body giant cell (FBGC) formation [3, 4]. Integrins comprise a large group of heterodimeric transmembrane molecules that mediate both cell–extracellular matrix and cell–cell interactions [5, 6]. These receptors are well known as important mediators of adhesion signaling between the extracellular and intracellular environments [7].
In addition to their roles in leukocyte extravasation to inflammatory sites, the β2 integrins αMβ2 and αXβ2 are capable of interactions with multiple ligands to mediate cell–particle or cell–substrate interactions and the induction of β1 integrin expression [8, 9]. These include the blood proteins complement C3bi and fibrin(ogen) adsorbed to material surfaces [10–12]. Through the essential arginine–glycine–aspartate cell attachment sequence, β1 integrins can bind multiple protein ligands, including fibronectin, vitronectin, collagens, and laminin; the interaction between fibronectin and α5β1 integrin is a classic example [5]. Consistent with this, we have demonstrated that vitronectin-adsorbed surfaces are an optimum substrate for monocyte adhesion leading to macrophage development and FBGC formation [13]. Therefore, the propensity for vitronectin adsorption to biomaterials likely plays a critical role in the development of the foreign body reaction.
Acute inflammation
The acute inflammatory response is marked by the presence of short-lived blood-derived polymorphonuclear leukocytes (PMNs), predominantly neutrophils, less than 10% eosinophils, and 1% basophils. Depending on the extent of injury created by material implantation, PMNs that initially rapidly accumulate in response to chemotactic stimuli cease to emigrate to the site of injury within minutes to days. PMNs are professional phagocytic cells that may function to immediately remove foreign microorganisms [14]. Moreover, during this brief phase, their secretory activities may be significant to the eventual biocompatible outcome. In addition to the elaboration of reactive oxygen intermediates, PMNs are capable of releasing cytokine mediators with potentials to influence the character and degree of subsequent inflammatory cell recruitment and activation. The resultant phenotypes of monocytes/macrophages and wound healing cells in the chronic inflammatory response to biomaterials may be, at least in part, governed by the biomaterial-dependent behavior of PMNs. In this regard, certain acute activities of PMNs have been studied on several biomaterials [15–22]. We have also observed that the co-culture of PMN together with monocytes/macrophages diminishes the subsequent formation of FBGC [23]. Related to this, the degranulation of tissue mast cells is reported to mediate acute inflammatory responses in vivo [24, 25]. However, the precise roles of acute inflammatory leukocytes in influencing chronic inflammatory, foreign body, and fibrosis host responses to implanted materials remain largely unknown. Our investigations to date have demonstrated that multiple aspects of the macrophage-mediated chronic response are influenced by material surface chemistry. Therefore, we predict that this may also be extended to the case of PMNs.
Chronic inflammation
Mononuclear leukocytes, i.e., monocyte-derived macrophages and lymphocytes, as well as the presence of plasma cells, define the chronic response, which also features neovascularization and the development of connective tissue. With biocompatible materials, the chronic phase is of limited duration and is usually evident for approximately 2 weeks. Macrophages are longer-lived than PMNs, and they are also professional phagocytes with extraordinary synthetic and secretory capacities [26]. Therefore, the macrophage is believed to exert key controlling influences on the ensuing wound healing/fibrosis responses. Depending on biomaterial surface chemistry, however, our studies have indicated that adherent monocyte-derived macrophages are differently activated for cytokine production and phenotypic expression. For example, we have identified several key biomaterial-dependent chemokine and cytokine mediators, interleukin (IL)-1β, IL-6, IL-8, and tumor necrosis factor (TNF)-α, with potential to mediate multiple autocrine and paracrine effects in the chronic inflammatory and wound healing phases [27–30], as well as a time-dependent switch in cytokine secretion from acute to chronic phase phenotype [27].
The presence of lymphocytes in these scenarios is less well studied, but our findings to date and those of others suggest that lymphocytes play a far greater role in the host response to implanted biomaterials than was previously appreciated. This is more fully addressed below.
Plasma cells are a component of the humoral immune system, and, although the role of these antibody-secreting cells in biocompatibility is not known, it cannot be completely discounted. Plasma cells have been reported to be present at other sites of injury and inflammation [31], indicating an as yet unknown significance in these scenarios.
Granulation tissue
The initiation of wound healing is marked by the arrival of fibroblasts and endothelial cells. These cell types are recruited by the activities of chronic inflammatory macrophages, in the presence of which they proliferate to form granulation tissue, so-called because of its characteristic macroscopic granular appearance in healing wounds. Granulation tissue develops only when there is tissue loss or disturbance of tissue architecture such that the wound healing process cannot fully restore the injured area to its previous state. Thus, granulation tissue serves as the intermediary substrate tissue for subsequent scar formation or fibrosis. Within granulation tissue, endothelial cells proliferate from pre-existing blood vessels and organize into new capillaries in the process of angiogenesis to supply the intermediary tissue with necessary blood flow. Fibroblasts synthesize extracellular matrix proteins, initially proteoglycans and later collagens. Collagens form the basis of the fibrous capsule (see below). Specialized fibroblasts called myofibroblasts mediate wound contraction in granulation tissue.
Foreign body reaction
Another critical feature of the macrophage is its intriguing and incompletely understood propensity to undergo fusion with other macrophages, leading to the formation of multinucleated giant cells. Giant cells are a classic identifying feature of chronic inflammation arising from the persistent presence of foreign microorganisms or foreign bodies in multiple scenarios [32, 33]. Thus, the multinucleated giant cells that form on or around biomaterials are referred to as foreign body giant cells or FBGC. In the case of implanted materials, the presence of macrophages and/or FBGC together with the components of granulation tissue is called the foreign body reaction (FBR). The form and topography of the implanted material, e.g., the flat surface of breast prostheses versus the rough topographies of vascular grafts, dictate the cellular composition of the FBR. In general, smooth or flat surfaced biomaterials exhibit a thin layer of macrophages with fibrosis compared to rough, high surface-to-volume fabrics, particulates, and porous implants, which feature relatively greater numbers of macrophages and FBGCs.
It is not uncommon for biomaterial-adherent FBGCs to be quite large, with tens to even hundreds of nuclei and measuring approximately 1 mm in diameter. These remarkable giant cells have been observed to occupy up to 25% of implant surface area on retrieved materials [34]. The FBR, composed of macrophages and FBGCs, may persist for the lifetime of the biomedical material or device [31, 33, 35]. Fibrosis (see below) also develops around the tissue/material interface with its associated FBR. This fibrous capsule appears to serve as a barrier between activities related to the FBR and those of normal host tissue.
In the 1990s, biomaterial pitting and surface cracking were discovered directly underneath adherent FBGCs in vivo [36], and it was therefore inferred that FBGCs mediate biomaterial degradation through the concentration of phagocytic and oxidative activities at the giant cell/biomaterial interface. Further, FBGC may produce cytokines that bias wound healing cells toward a fibrogenic phenotype. Consistent with this, we have also discovered that cultures of fusing macrophages and FBGC strongly express connective tissue growth factor (unpublished results). Clinically, these activities appear to manifest as biomaterial degradation, fibrous encapsulation, and device failure [35, 37, 38].
In vitro, however, we originally discovered that FBGC are induced from human monocyte-derived macrophages by lymphokines that are well known to exert anti-inflammatory effects on multiple monocyte/macrophage activities [39, 40]. Later, we found that this is also the case for α-tocopherol, the major component of the antioxidant vitamin E [41]. This is more completely addressed below. We further learned that lymphokine-induced FBGC formation is highly material surface property-dependent. For example, IL-4-induced FBGC formation occurs readily on nitrogenated and oxygenated but not on fluorinated or silicone-coated model polystyrenes [42]. This phenomenon has since been confirmed with multiple types of biomaterials and engineered surfaces [43–47].
With this perspective, FBGC formation has appeared to be an undesirable phenomenon with a negative impact on biocompatibility. It was speculated that FBGC formation represented the joining of otherwise ineffective phagocytic cell forces by host mechanisms attempting to remove the implanted foreign body. Therefore, as presently perceived, the foreign body reaction in terms of macrophage adhesion and FBGC formation is believed to be undesirable and a target for intervention. A broader perspective, however, dictates that these phenomena represent partial aspects of a continuum or collective host response that is initiated and maintained by the introduction and persistent presence of a non-phagocytosable foreign body. With this view, it is clear that in order to fully understand the foreign body reaction, additional host mechanisms responding to biomaterial implantation must also be characterized.
Fibrosis
The ideal biocompatible outcome for biomaterial implantation would clearly be the restoration of normal tissue architecture and function following wound healing. With only a few exceptions, however, fibrosis with fibrous encapsulation is generally the final stage of the wound healing response to biomaterials. In most cases, the surgically injured tissue is composed primarily of permanent cell types that cannot regenerate, and the process of repair can provide only the fibrous capsule as replacement tissue
Biomaterial-induced macrophage activation
Multinucleated giant cells, formed by the fusion of macrophages, are a hallmark feature of chronic inflammation due to the persistent presence of a non-phagocytosable foreign body. As mentioned above, FBGCs are believed to be implicated in biomaterial degradation. However, of the three macrophage fusion factors that we have identified (IL-4, IL-13, and α-tocopherol) [39–41], each is well documented to down-modulate so-called “pro-inflammatory” activities of macrophages. IL-4 and IL-13 are each considered to be “alternative” macrophage activation cytokines [48], and α-tocopherol exhibits host tissue protective effects via antioxidant as well as non-antioxidant mechanisms [49, 50]. Therefore, an apparent paradox between biomaterial degradation and down-modulation of inflammation by biomaterial-adherent macrophages and FBGCs remains to be resolved, i.e., what is the biomaterial-induced macrophage activation phenotype?
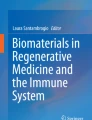
The concept of “alternative” macrophage activation was introduced to distinguish Th2 lymphokine (IL-4)-activated macrophages from “classically” activated macrophages, which develop under the influence of the Th1 lymphokine interferon (IFN)-γ [51–54]. IL-4 and IFN-γ are well documented to exert antagonistic effects on macrophages. For example, mannose receptor-mediated phagocytosis is strongly induced by IL-4 and inhibited by IFN-γ, which instead supports IgG-mediated phagocytosis. The production of pro-inflammatory cytokines (IL-1, IL-6, TNF-α) is induced by IFN-γ but inhibited by IL-4, which instead induces anti-inflammatory cytokines (IL-1 receptor antagonist and IL-10), thereby promoting wound healing and matrix deposition. Microbicidal reactive oxygen and nitrogen species are induced by IFN-γ, but IL-4 induces arginase-1 activity, which mediates collagen deposition and tissue repair. Further, our investigations have revealed that IL-4, IL-13, or α-tocopherol promotes the formation of very large foreign body-type multinucleated giant cells that are morphologically identical to those found on biomaterials [39–41]. This is illustrated in Fig. 1. For purposes of contrast, Fig. 1 also shows that, although IFN-γ together with IL-3 or granulocyte-macrophage colony-stimulating factor also induces macrophage fusion, the resulting multinucleated giant cells are the morphologically distinct Langhans-type giant cells [39], which are not found adherent to retrieved biomaterials. The functional significances of these morphological variants at various sites of chronic inflammation have yet to be established.

Alternative versus classical macrophage activation leads to morphological variants of multinucleated giant cells in vitro. The alternative activation cytokine IL-4 (or IL-13 or α-tocopherol) promotes macrophage fusion and the formation of large foreign body-type giant cells (FBGC) with randomly arranged nuclei and high degrees of cytoplasmic spreading. The classical activation cytokine IFN-γ (together with IL-3 or granulocyte-macrophage colony-stimulating factor) induces more limited degrees of macrophage fusion with resultant Langhans-type giant cells [39–41]
Our discoveries that the alternative macrophage activation cytokines IL-4 and IL-13 are potent inducers of macrophage fusion in vitro [39, 40] led to the finding that IL-4 plays an important role in FBGC formation in vivo [55]. IL-4 and IL-13 are well-recognized as Th2 lymphocyte products. However, IL-4 and IL-13 are also produced by natural killer (NK) and NKT lymphocytes. Alternatively, eosinophils, basophils, and mast cells are also potential sources of these cytokines [56]. The precise origins of FBGC-inducing cytokines at the implant site remain unclear.
More recently, the repertoire of macrophage activation has been expanded to include a state of “innate” activation in response to Neisseria, which exhibits increased production of reactive oxygen and nitrogen species, phagocytosis, and expression of co-stimulatory molecules [53]. Therefore, as studies on macrophage activation advance, it is likely that macrophage heterogeneity will be analogously advanced to reveal multiple phenotypic states of macrophage activation customized to distinct stimuli, including implanted biomaterials.
Our more recent in vitro studies have revealed several novel characteristics of IL-4-induced fusing macrophages/FBGCs. Namely, they strongly express an alternative activation marker, galectin-3, the galectin-3 ligand and lymphocyte-co-stimulatory molecule CD98, as well as additional and select lymphocyte-co-stimulatory molecules that may indicate down-modulation of lymphocyte activities (unpublished findings). These findings will be extended toward a more comprehensive characterization of the macrophage activation phenotype that ensues from interactions with implanted biomaterials, biomedical devices, and prostheses. Thereby, we may ultimately illuminate the physiological significance of FBGC formation at sites of biomaterial implantation. This, in turn, will provide clinicians with a more complete perspective on the efficacy of interventions in the foreign body reaction at implant sites.
Inflammatory cell interactions in biocompatibility
Macrophages as key determinants of biocompatible outcome
Inflammatory cell interactions significantly impact the biocompatibility and function of medical devices, prostheses, and biomaterials and can ultimately precipitate their clinical failure [1]. As subjects of extensive investigations, monocyte-derived macrophages and FBGCs are believed to exert critical effects on both tissue and implanted biomaterial. Adherent macrophages and/or FBGCs may promote clinically significant biomaterial biodegradation through the release of reactive oxygen intermediates with resultant oxidative cleavage of the soft segment in polyether polyurethanes. A classic example is the apparent macrophage and/or FBGC-mediated biodegradation of Pellethane 80A used as insulation in pacemaker leads [38]. Over time, this material undergoes oxidative biodegradation with loss of insulation integrity and ultimate pacemaker failure. A second example is the focal biodegradation of Dacron® polyester vascular grafts. Biodegradation occurs over long time periods with areas of material loss being replaced by fibrous tissue. The significant clinical outcome is focal aneurysm in the vascular graft wall, necessitating replacement surgery with its attendant problems [35].
Adherent macrophages and FBGC also possess potentials to impact host tissue responses via the production of multiple chemokines and cytokines that promote cellular accumulation and proliferation. Clinically, these phenomena are well known and documented to lead to failure mechanisms. Examples include anastomotic hyperplasia in human vascular grafts leading to blood flow turbulence and thrombosis and coronary artery stent restenosis, in which the inflammatory response to both simple and polymer-coated drug eluted stents can result into smooth muscle cell and fibroblast proliferation in the stenotic component [57, 58]. An additional example is found in aseptic loosening of joint prostheses, as in total hip or knee replacement, where the fibrotic response separates bone from either the prosthesis or its polymethylmethacrylate bone cement [35]. Fibrous capsule formation in this area then leads to micromotion that, in turn, causes aseptic loosening of the prosthesis. Related to this, one mechanism for breast implant failure involves capsular contraction, leading to pain and breast deformation [37]. Biosensor function is also compromised by biofouling and fibrous capsule formation [59]. Thus, fibroblast proliferation and enhanced extracellular matrix formation have been implicated clinically in the failure of a wide variety of medical devices and prostheses.
Modulation of adhesion and activation of macrophages and FBGC with anti-inflammatory drugs may enhance the performance of pacemaker lead electrodes by reducing the inflammatory response and ultimate fibrous encapsulation. However, in clinical application, this type of solution to reduce local inflammatory cell interactions is rare and limited. Long-term systemic use of anti-inflammatory drugs may compromise host defenses, leading to impaired inflammatory and immune responses and increased potential for infection.
Synthetic and modified natural tissue engineering scaffolds are also susceptible to the foreign body reaction, which can markedly reduce the function and usefulness of tissue-engineered constructs [60]. Predictably, surface modifications that inhibit, attenuate, or alter the progression of these events will enhance the function of these constructs. We believe that material-dependent monocyte/macrophage adhesion mechanisms, adhesion signaling, anoikis (apoptosis induced by adhesion failure), and chemokine/cytokine networks are four key acute and chronic cellular response mechanisms that, once understood, may potentially be targeted for control of biocompatible outcome. It is widely believed that attenuation of these critical monocyte, macrophage, or FBGC responses will lead to a diminished foreign body reaction and increased efficacy of medical device function.
The emerging roles of lymphocytes in biocompatibility
It is important to re-emphasize that lymphocytes appear together with monocyte-derived macrophages in the chronic phase. Therefore, their potential interactions with and influences on macrophages as well as the effects of biomaterials on lymphocytes themselves must be considered in our efforts to understand biocompatibility mechanisms.
Lymphocyte responses to conventional microbial pathogens have long been extensively studied within the context of classical immunity, which exhibits specificity and memory. Biomaterials, largely synthetic polymers or metals, are apparently not immunogenic in the classic adaptive sense. Thus, an awareness that lymphocytes react to a foreign body outside of this classical context is emerging. In this regard, we can utilize known aspects of lymphocyte biology to investigate their responses to biomaterials, but we must broaden developing perceptions on biocompatibility mechanisms to encompass possibilities beyond classical immune responses. Our recent studies, as discussed below, have demonstrated that lymphocytes play a much greater role in the inflammatory and foreign body responses to implanted biomaterials than was previously realized [61–67].
Also in support of this, lymphocyte responses to synthetic materials have been clinically observed. Patients implanted with left ventricular assist device (LVAD) experience a reduction in circulating CD4+ T lymphocyte populations, which is due to their apoptosis [68]. These patients also have a B lymphocyte hypersensitivity, which complicates their ability to receive a donor heart and has been found to be due to T lymphocyte activation of B cells. The culture of human peripheral mononuclear cells from healthy donors with LVAD biomaterial is reported to result in T lymphocyte activation. Intriguingly, activated T lymphocytes adherent to macrophages are present on LVAD surfaces retrieved from patients [69].
NK lymphocytes, which play prominent roles in host defense against viral infection, have also been found to be adversely affected by exposure to biomedical polymers materials. Patients undergoing hemodialysis exhibited reduced numbers of circulating NK cells after dialysis. Moreover, this finding was extended to demonstrate subsequent decreased NK cell activity in vitro [70, 71]. Related to this, hemodialysis patients acquire an increased susceptibility to and incidence of viral infections [72]. These collective findings clearly indicate that lymphocyte responses to biomedical polymers can lead to adverse clinical consequences and reduced biocompatibility.
Conventionally, lymphocytes become activated through interactions with antigen-presenting cells, i.e., macrophages and dendritic cells, which present processed antigen bound to major histocompatibility complex molecules on their cell surfaces [73, 74]. Characteristics of activation include expression of cell surface markers of activation, calcium flux, and production of the classic activation lymphokines IL-2 and IFN-γ. The activation markers CD40 ligand and calcium influx are induced on T lymphocytes cultured with polyurethane [75]. Activation alone, however, is not sufficient for effector function. T lymphocytes require additional cognate interactions with specific molecules on antigen-presenting cells, e.g., macrophages; these are collectively referred to as co-stimulation. Following cognate activation, lymphocytes may undergo clonal expansion by proliferation [73]. Specific types of co-stimulatory molecules also regulate functional outcomes of lymphocyte activation; lymphocyte effector function may be up- or down-regulated [76]. Alternative to cognate activation, in the presence of activation signals without co-stimulation, lymphocytes cannot acquire effector function and are referred to as anergic. Anergic responses are a mechanism for suppression of inappropriate immune reactivity, such as to self antigen [77]. A further alternative to activation is apoptosis. By this mechanism, cells which may have been inappropriately activated undergo programmed cell death and are removed by macrophages [78]. The clinical findings outlined above indicate that mechanisms of lymphocyte activation or anergy, as well as apoptosis are precipitated by lymphocyte interactions with implanted biomaterials.
Macrophage/lymphocyte interactions
The progression of inflammatory events and the foreign body reaction features the appearance of mononuclear leukocytes (monocytes/macrophages and lymphocytes) at the site of biomaterial implantation. The guided movements of these cells are mediated by cytokines and chemokines, which also participate in lymphocyte differentiation, lymphocyte proliferation, and macrophage activation. Mediators such as I-309, macrophage inflammatory protein (MIP)-1β, IL-8, MIP-3α, and IFN-γ-induced protein (IP)-10 can attract specific lymphocyte subpopulations [79] or activate/enhance activation of lymphocytes (IL-1β, MIP-1β, IL-6) [80, 81].
Lymphocytes and monocytes/macrophages are capable of activating each other through direct and indirect mechanisms. T lymphocytes can be activated by cytokines such as IFN-γ, IL-2, TNF-α, IL-6, IL-15, and IL-18 [82]. NK lymphocytes are activated and proliferate when exposed to chemokines MIP-1β, macrophage chemotactic protein (MCP)-1, and chemokine C-C motif ligand (CCL) 5 [81]. Activated T lymphocytes induce production of the pro-inflammatory cytokines IL-1, TNF-α, and IL-6, and the chemokines IL-8, MCP-1, and MIP-1β from monocytes/macrophages in a contact-dependent manner [83, 84]. Depending on the cytokine/chemokine stimulus, macrophages can be activated to produce a myriad of cytokines [85].
Cytokines that we have detected at sites of biomaterial implantation are also capable of suppressing lymphocyte and macrophage behaviors. IL-10 is an anti-inflammatory cytokine capable of inducing CD4+ T cell antigen-specific anergy [86]. Chronic TNF-α exposure can lead to T cell hypo-responsiveness by down-regulation of the T cell receptor/CD3 [87]. TNF-α also induces apoptosis [88]. We have demonstrated induction of macrophage apoptosis on biomaterial surfaces through TNF-α-mediated mechanisms and inhibition of these mechanisms by the lymphokine IL-4 [89, 90]. This indicates further influences of lymphocytes in the complex cell–cell interactions on biomaterials and presents an additional avenue for investigation of the mechanisms by which lymphocytes influence critical behaviors of macrophages and FBGCs.
NK and NKT lymphocytes are key mediators of innate host response mechanisms through cytokine production and regulation of autoimmune and inflammatory diseases [91–94]. NK cells are activated by direct receptor/ligand interactions but also indirectly by cytokines, for example, to produce IFN-γ [93, 95]. As mentioned above, there is evidence that NK lymphocyte functions are affected by exposure to dialysis membranes [70–72]. However, their responses to implanted biomaterial surfaces have not been characterized and remain unknown. Importantly, these cell types are potential sources of IL-4 and/or IL-13 [92, 96–98], which may promote the foreign body reaction by inducing macrophage fusion to form FBGCs [39, 40].
Our current data suggest that T lymphocyte-deficient mice exhibit a normal foreign body reaction to implanted material (see below) [99]. Therefore, whether NK or NKT lymphocytes are sources of IL-4/IL-13 relevant to FBGC formation remains an intriguing question. In addition, IL-13 produced by NKT lymphocytes has been implicated in the progression of fibrosis [100, 101]. Therefore, the potential participation of this lymphocyte subset in the fibrous encapsulation of implanted materials, perhaps via IL-13 stimulation of macrophages to produce transforming growth factor (TGF)-β [102], is another critical issue.
Our investigations to date have revealed further evidence that, in addition to the macrophage, it is important to consider the influences of lymphocytes on biocompatible outcome. We have discovered lymphocyte effects on macrophage adhesion and fusion as well as on biomaterial-dependent cytokine production. Interestingly, the secondary response of lymphocytes to biomaterials has been found to be distinct from the primary response in vivo. The significant findings from our investigations on lymphocyte/macrophage interactions are summarized in Table 2 and further discussed below.
Lymphocyte modulation of macrophage adhesion and FBGC formation
Despite their early and relatively transient presence at sites of biomaterial implantation, few studies have focused on how lymphocytes may influence the subsequent foreign body response. Based on our in vitro human monocyte/macrophage/FBGC system, a lymphocyte/macrophage co-culture system was developed to address these unknowns [61]. We discovered that when lymphocytes are present at an optimal ratio of 25:1 during the initial adhesion of monocytes, the rates of monocyte adhesion and subsequent macrophage fusion are significantly increased (50–60% fusion) when compared to monocytes alone (10% fusion). If lymphocytes are added at later time points (days 3 or 7), these differences are diminished, indicating that lymphocyte interactions with monocytes during early stages of adhesion and culture are critical for increasing monocyte/macrophage adhesion and subsequent macrophage fusion. Importantly, we found that 90% of adherent lymphocytes associate with adherent macrophages and not with biomaterial surfaces. In turn, these interactions led to increases in lymphocyte proliferation, which was greatest on day 3 but also significantly greater than a lectin-stimulated lymphocyte control population at later time points (days 7 and 10). These studies are the first to demonstrate that interactions between monocytes/macrophages and lymphocytes provoke responses from each cell type that are directly relevant to the foreign body reaction.
Lymphocyte/macrophage interactions are differentially influenced by material surface chemistry
Using our lymphocyte/macrophage co-culture system, we addressed the effects of different material surface chemistries on monocyte adhesion, macrophage fusion, and lymphocyte proliferation [62]. A series of poly(ethylene terephthalate) (PET)-based materials was employed to present hydrophobic, hydrophilic/neutral, hydrophilic/anionic, and hydrophilic/cationic chemistries to cells. Hydrophilic/neutral surfaces interfered with initial monocyte/macrophage adhesion (day 0), thereby precluding subsequent macrophage fusion and FBGC formation. These surfaces also were unable to support lymphocyte proliferation at later time points. In contrast, hydrophilic/anionic surfaces exhibited decreases in macrophage adhesion between days 3 and 7, but increases lymphocyte proliferation and macrophage fusion at later time points. Hydrophilic/cationic surfaces also demonstrated decreases in macrophage adhesion between days 3 and 7, but, unlike anionic materials, there were no corresponding increases in lymphocyte proliferation or macrophage fusion on the cationic surfaces. These results clearly demonstrate that differences in material surface chemistry are capable of provoking very different cellular responses. Effects on lymphocyte function as well as monocyte/macrophage adhesion and fusion resulting from interactions with lymphocytes are readily apparent in this model system.
Chemokines/cytokines in lymphocyte/macrophage interactions
The progression/continuum of inflammatory events and the foreign body reaction (Table 1) feature the appearance of mononuclear leukocytes (monocytes/macrophages and lymphocytes) at the site of biomaterial implantation. The guided movements of these cells are mediated by cytokines and chemokines, which also participate in lymphocyte differentiation, lymphocyte proliferation, and macrophage activation [54, 80, 103]. Our studies point to cytokine-mediated (indirect) signaling in lymphocyte enhancement of monocyte adhesion and macrophage fusion [61].
Utilizing cytokine protein arrays and ELISA to investigate cytokine and chemokine production from lymphocyte/macrophage co-cultures, we identified production of soluble mediators that are capable of targeting both lymphocytes and macrophages [63]. For instance, MCP-1, a chemoattractant for monocytes/macrophages, also supports macrophage fusion [104]. Other detected mediators (I-309, MIP-1β, IL-8, MIP-3α, and IP-10) can attract specific lymphocyte subpopulations [79] or activate or enhance activation of lymphocytes (IL-1β, MIP-1β, IL-6) [80, 81].
Lymphocytes and monocytes/macrophages are capable of activating each other through direct and indirect mechanisms. T lymphocytes can be activated by cytokines such as IL-2, TNF-α, IL-6, IL-15, and IL-18 [82]. NK cells are activated and proliferate when exposed to the chemokines MIP-1β, MCP-1, and CCL5 [81]. Activated T lymphocytes induce production of the pro-inflammatory cytokines IL-1, TNF-α, and IL-6, and the chemokines IL-8, MCP-1, and MIP-1β from monocytes/macrophages in a contact-dependent manner [83, 84]. Depending on the cytokine/chemokine stimulus, macrophages can be activated to produce multiple cytokines [85]. The specific soluble mediator(s), lymphocyte/macrophage cell surface molecular interactions, and lymphocyte subpopulation(s) involved in the observed enhancement of adherent monocyte, macrophage, or FBGC formation have been targets in our investigations.
Cytokines that we have detected at sites of biomaterial implantation are also capable of suppressing lymphocyte and macrophage behaviors. IL-10 is an anti-inflammatory cytokine capable of inducing CD4+ T cell antigen-specific anergy [86]. As mentioned earlier, chronic stimulation by TNF-α down-modulates the T cell receptor/CD3 and induces T cell hypo-responsiveness [87]. TNF-α also induces apoptosis [88]. Our studies have shown that the biomaterial-dependent induction of macrophage apoptosis occurs through TNF-α-mediated mechanisms; these mechanisms are blocked by IL-4 [46, 89, 90]. The significance of these cytokines in modulating lymphocyte behavior at sites of biomaterial implantation is not yet clear.
Lymphocyte/macrophage interactions and biomaterial-dependent cytokine production
To investigate the effects of biomaterial surface chemistry on the production of cytokines, chemokines and extracellular matrix metalloproteinases (MMPs) from lymphocytes and macrophages, human monocytes and lymphocytes were co-cultured on chemically distinct PET-based material surfaces as described above. Antibody array screening indicated that the majority of detected proteins are inflammatory mediators that guide the early inflammatory phases of wound healing [63]. Proteomic ELISA quantification and adherent cell analysis were performed after 3, 7, and 10 days of culture. IL-2 was not detected in any co-cultures suggesting that lymphocyte activation does not occur by classic immune response mechanisms. The hydrophilic/neutral surfaces increased IL-8 relative to the hydrophobic PET surface (p < 0.05). The hydrophilic/anionic surfaces promoted increased TNF-α over hydrophobic and cationic surfaces and increased MIP-1β compared to hydrophobic surfaces (p < 0.05). Since enhanced macrophage fusion was observed on hydrophilic/anionic surfaces, the production of these cytokines may be related to FBGC formation. The hydrophilic/cationic surface promoted IL-10 production and increased MMP-9/tissue inhibitor of MMP (TIMP) relative to hydrophilic/neutral and anionic surfaces (p < 0.05). The collective results of this study suggest that hydrophilic/neutral and anionic surfaces promote pro-inflammatory responses and reduced matrix degradation, whereas the hydrophilic/cationic surfaces induce an anti-inflammatory response and greater MMP-9/TIMP with an enhanced potential for matrix breakdown [63]. This in vitro investigation also underscores the usefulness of protein arrays in assessing the roles of soluble mediators in the inflammatory response to biomaterials and may provide perspective for future clinical assessments. How specific lymphocyte and macrophage interactions result in biomaterial-dependent cytokine production is unclear.
Direct versus indirect lymphocyte/macrophage interactions and biomaterial-dependent production of selected cytokines
Lymphocyte interactions with adherent macrophages and model surface-modified materials were further investigated by culturing monocytes alone or together with lymphocytes, either in direct co-cultures or indirectly in transwells with 0.02-μm pores to allow diffusion of soluble components [64]. The cultures were carried out on PET-based photograft co-polymerized material surfaces displaying distinct hydrophobic, hydrophilic/neutral, hydrophilic/anionic, and hydrophilic/cationic chemistries, with monocytes/macrophages seeded onto the test materials in the transwell system. After periods of 3, 7, and 10 days, cytokine production was quantified by ELISA and normalized to adherent macrophage/FBGC density to yield a measure of adherent macrophage/FBGC activation. Hydrophilic/neutral and hydrophilic/anionic surfaces evoked the highest levels of activation. Adherent macrophages/FBGCs in co-culture with lymphocytes increased production of IL-1β, TNF-α, IL-6, IL-8, and MIP-1β on the base PET, hydrophobic, and hydrophilic/cationic surfaces indicating a role for lymphocytes in the inflammatory response to biomaterials. IL-10 production was material-dependent but unaffected by direct or indirect lymphocyte interactions. At early time points (day 3), indirect signaling promoted enhanced macrophage/FBGC activation while direct interactions may inhibit that response. At later time points (10 days), direct interactions dominated and increased the activation level. Lymphocytes did not have a significant effect on MMP-9, TIMP-1, and TIMP-2 production. Biomaterial surface chemistries differentially affected lymphocyte and macrophage/FBGC interactions as the increased levels of activation were not evident on hydrophilic/neutral or entirely evident on hydrophilic/anionic surfaces. Therefore, although the majority of adherent lymphocytes in co-cultures are in direct contact with adherent macrophages and not with materials lymphocyte-mediated macrophage activation for cytokine production does not require direct interactions with lymphocytes. Whether direct interactions between these cell types actually inhibit the macrophage response is an intriguing question.
Lymphocyte/macrophage interactions induce the lymphokine interferon (IFN)-γ
Interestingly, our most recent data reveal that IFN-γ is produced in significant picogram per millilter amounts in lymphocyte/macrophage co-cultures on days 3, 7, and 10, either in direct co-cultures or when these populations are segregated in transwell cultures [65]. Essentially, no IFN-γ is detected in lymphocyte-only (or monocyte-only) cultures, suggesting that either direct or indirect interactions of lymphocytes with biomaterial-adherent monocyte-derived macrophages are required for the induction of this classical activation lymphokine. We interpret this to mean that IFN-γ production from lymphocytes requires induction by a macrophage-derived cytokine(s) or other soluble factor, but we also observed that the levels of IFN-γ in direct co-cultures is increased relative to those in indirect transwell cultures, indicating synergism of direct and indirect interactions. In addition, IFN-γ production is model surface material-dependent as follows: hydrophilic/anionic ≥ hydrophobic = base PET ≥ hydrophilic/cationic ≥ hydrophilic/neutral. Our earlier work demonstrated that IFN-γ in combination with macrophage developmental cytokines could induce limited macrophage fusion and multinucleated giant cell formation [39]. Now, we have discovered that lymphocyte interactions with biomaterial-adherent macrophages elicit the production of this classic macrophage activation cytokine from lymphocytes in vitro. As noted above, IL-2 was not detected in lymphocyte/macrophage co-cultures, indicating selective lymphokine signaling via IFN-γ. These data provide further evidence for important interactions between lymphocytes and macrophages at sites of biomaterial implantation.
In vivo secondary responses to biomaterial implantation are characterized by recruitment of T lymphocytes and phagocytic cells
Biomaterials are widely believed to be non-immunogenic, as polymer subunits are not considered to be antigens in the classic sense. Therefore, the nature of host response to implanted polymeric biomedical materials has been largely assumed to be non-adaptive or non-immune. Classic features of adaptive immunity are specificity and memory, i.e., specific antigen-driven lymphocyte responses which are more rapid and magnified upon secondary exposure, with increases in the percentages of CD4+ (helper) and CD4+/CD25+ (activated) T lymphocytes. To directly address this issue, we compared the in vivo primary and secondary host responses to three clinically-relevant biomaterials: a poly (ether urethane) (PEU), silicone rubber, and PET using our rat cage implant model [66]. Caged polymer samples were subcutaneously implanted for 14 days and then explanted. After a 2-week healing period, the identical rats were implanted a second time with cages containing new samples of the same polymers for an additional 2 weeks. Exudates were analyzed at 4, 7, and 14 days post-primary or post-secondary implantation by flow cytometry for the following cell types: CD4+ T lymphocytes, CD4+/CD25+ T lymphocytes, CD8+ T lymphocytes (suppressor), B lymphocytes, PMNs, and macrophages. At day 14 following secondary implantation, we observed significant increases in T lymphocytes, PMNs, and macrophages in the exudates compared to primary implantation for all groups. B lymphocytes were not detected. Significantly, CD4+/CD8+ ratios, percentages of CD4+/CD25+ T lymphocytes, macrophage adhesion, and FBGC formation were each comparable between primary and secondary implantations. Therefore, our results argue against an adaptive host response in the classic sense. However, following re-implantation of biomaterials, we found significant quantitative increases in both phagocytic cells and T lymphocytes with constant T cell subset distributions. This indicates recruitment of these cell types upon secondary exposure to biomedical polymers. Whether the observed secondary cellular recruitment is biomaterial-specific remains to be determined
In vivo cytokine profiles are biomaterial-dependent
To identify cytokine signals in cell–cell communication during the foreign body reaction in vivo, investigation of cytokines at biomaterial implant sites was carried out [67]. Macrophage activation cytokines (IL-1β, IL-6, TNF-α), cytokines important for macrophage fusion (IL-4, IL-13), a T cell activation cytokine (IL-2), anti-inflammatory cytokines (IL-10, TGF-β), and chemokines (GRO/KC, MCP-1) were quantified at biomaterial implant sites using a multiplex immunoassay and ELISA. Empty cages (controls) or cages containing synthetic biomedical polymer, either PEU, silicone rubber, or PET, were implanted subcutaneously in rats for 4, 7, or 14 days, and cytokines in exudate supernatants and macrophage surface adhesion and fusion were quantified. The presence of a polymer implant did not affect the levels of IL-1β, TGF-β, and MCP-1 in comparison to the control group. IL-2 was not detected in these exudate samples. However, the levels of IL-6, TNF-α, IL-4, IL-13, IL-10, and GRO/KC were modulated by polymer implantation. The levels of IL-6 and TNF-α were significantly greater in animals implanted with PEU and silicone rubber, which are materials that, conversely, do not support FBGC formation. These results confirm and extend our in vitro data to indicate that the cytokine production profiles of adherent macrophages and FBGCs in vivo are biomaterial-dependent. Further, the possibility is raised that the presence of macrophage fusion and FBGC formation on biomaterial surfaces represents host down-modulation of pro-inflammatory cytokine production, perhaps via phagocytic removal/sequestration of macrophages actively elaborating these cytokines. If so, current perception of the so-called “inflammatory giant cell” must evolve to accommodate this new concept.
Nude mice exhibit a normal foreign body reaction to implanted material
Our data with nude (i.e., athymic) mice indicate that these Th1 and Th2 lymphocyte-deficient mice are capable of forming FBGCs that are comparable to those of normal mice both in morphology and extent of formation [99]. These data suggest that Th2 lymphocytes are not the source or not the only source of relevant fusion-inducing IL-4 or IL-13. This is consistent with the common theme of redundancy in host defense systems. Other potential sources of IL-4 and IL-13 are NK or invariant NKT lymphocytes (which do not undergo maturation in the thymus), mast cells, basophils, and eosinophils [56, 98]. Furthermore, although our results confirm that IL-4 plays an important role in FBGC formation on biomaterials in vivo [55], it is very possible that additional macrophage fusion-inducing cytokines will be discovered. For example, IL-21 is a more recently discovered cytokine which exerts effects that are similar to IL-4 and IL-13 in the alternative activation of macrophages [105]. Whether IL-21 can induce FBGC formation is not yet known. Therefore, the questions raised by these preliminary results are intriguing and significant. Their answers will definitively expand our current understanding of the inflammatory response to implanted materials.
Conclusions
Host response evaluation of implants is critical to determining the safety and biocompatibility of medical devices, prostheses, and biomaterials. This chapter first presents an overview of the sequence and continuum of events in the inflammatory and wound healing responses that facilitate biocompatibility evaluation. This is followed by summaries of our results to date on lymphocyte responses to biomaterials in vitro and in vivo. Our investigations indicate that lymphocytes and lymphocyte/macrophage interactions play much more significant roles at implant sites than have been previously appreciated. Given the current and future development of tissue-engineered constructs and bioactive agent delivery systems, lymphocyte function and immunotoxicity evaluation may play a significant role in determining the safety of these respective systems. This, in turn, requires a better understanding of the mechanisms leading to immunotoxicity or acquired immunity as they relate to the specific composition of the respective tissue-engineered constructs and/or bioactive agent delivery systems under investigation. An understanding of the mechanisms and methods presented in this chapter can permit the early identification of factors that may compromise or obviate the biocompatibility of medical devices, prostheses, and biomaterials. Early identification of problems related to biocompatibility including immunotoxicity can permit new design criteria to be introduced into the research development process.
References
Anderson JM (2001) Biological responses to materials. Ann Rev Mater Res 31:81–110
Horbett T (2004) The role of adsorbed proteins in tissue response to biomaterials. In: Ratner B et al (eds) Biomaterials science: an introduction to biomaterials in medicine. Elsevier, San Diego, pp 237–246
McNally AK, Anderson JM (2002) Beta1 and beta2 integrins mediate adhesion during macrophage fusion and multinucleated foreign body giant cell formation. Am J Pathol 160:621–630
McNally AK, MacEwan SR, Anderson JM (2007) Alpha subunit partners to beta-1 and beta-2 integrins during IL-4 induced foreign body giant cell formation. J Biomed Mater Res 82A:568–574
Ruoslahti E (1996) RGD and other integrin recognition sequences for integrins. Ann Rev Cell Dev Biol 12:697–715
Gonzales-Amaro R, Sanchez-Madrid F (1999) Cell adhesion molecules: selectins and integrins. Crit Rev Immunol 19:389–429
Giancotti FG, Ruoslahti E (1999) Integrin signaling. Science 285:1028–1032
Berton G, Lowell CA (1999) Integrin signaling in neutrophils and macrophages. Cell Signal 11:621–635
Werr J, Eriksson AA, Hedqvist P, Lindbom L (2000) Engagement of beta2 integrins induces surface expression of beta1 integrin receptors in human neutrophils. J Leukoc Biol 68:553–560
Anderson JM, Ziats NP, Bonfield TL, McNally AK, Topham NS (1991) In: Akutsu T, Koyanagi H (eds) Human blood protein and cell interactions with cardiovascular materials. Artificial Heart 3. Springer, New York, pp 45–55
McNally AK, Anderon JM (1994) Complement C3 participation in monocyte adhesion to different surfaces. Proc Natl Acad Sci USA 91:10119–10123
Harbers G, Grainger DW (2006) Cell-materials interactions: fundamental design issues for tissue engineering and clinical considerations. In: Hollinger JO, Guelcher S (eds) An introduction to biomaterials. CRC, New York, pp 15–45
McNally AK, Jones JA, MacEwan SR, Colton E, Anderson JM (2008) Vitronectin is a critical adhesion protein for macrophage development and IL-4-induced foreign body giant cell formation in vitro. J Biomed Mater Res 86A:535–543
Greenberg S (1999) In: Gallin JI, Snyderman R (eds) Biology of phagocytosis. Inflammation: basic principles and clinical correlates. Lippincott, Williams, and Wilkins, Philadelphia, pp 681–701
Kaplan SS, Basford RE, Jeong MH, Simmons RL (1994) Mechanisms of biomaterial-induced superoxide release by neutrophils. J Biomed Mater Res 28:377–386
Gemmell CH, Black JP, Yeo EL, Sefton MV (1996) Material-induced up-regulation of leukocyte CD11b during whole blood contact: material differences and a role for complement. J Biomed Mater Res 32:29–35
Swartbol P, Truedsson L, Pärsson H, Norgren L (1996) Surface adhesion molecule expression on human blood cells induced by vascular graft materials in vitro. J Biomed Mater Res 32:669–676
Chang CC, Lieberman SM, Moghe PV (1999) Leukocyte spreading behavior on vascular biomaterial surfaces: consequences of chemoattractant stimulation. Biomaterials 20(3):273–281
Chang CC, Rosenson-Schloss RS, Bhoj TD, Moghe PV (2000) Leukocyte chemosensory migration on vascular prosthetic biomaterial is mediated by an integrin beta2 receptor chain. Biomaterials 21(22):2305–2313
Rosenson-Schloss RS, Chang CC, Constantinides A, Moghe PV (2002) Alteration of leukocyte motility on plasma-conditioned prosthetic biomaterial, ePTFE, via a flow-responsive cell adhesion molecule, cd43. J Biomed Mater Res 60(1):8–19
Tan J, Saltzman WM (2002) Topographical control of human neutrophil motility on micropatterned materials with various surface chemistry. Biomaterials 23:3215–3225
Gorbet MB, Sefton MB (2004) Biomaterial-associated thrombosis: roles of coagulation factors, complement, platelets and leukocytes. Biomaterials 25:5681–5703
Kirk JT, McNally AK, Anderson JM (2010) Polymorphonuclear leukocyte inhibition of monocytes/macrophages in the foreign body reaction. J Biomed Mater Res A 94:683–687
Al-Saffar N, Iwaki H, Revell PA (1998) Direct activation of mast cells by prosthetic biomaterial particles. J Mater Sci Mater Med 9:849–853
Tang L, Jennings TA, Eaton JW (1998) Mast cells mediate acute inflammatory responses to implanted biomaterials. Proc Natl Acad Sci USA 95:8841–8846
Gordon S (1999) Development and distribution of mononuclear phagocytes: relevance to inflammation. In: Gallin JI, Snyderman R (eds) Inflammation. Basic principles and clinical correlates. Lippincott, Williams & Wilkins, Philadelphia, pp 35–48
Jones JA, Chang DT, Colton E, Kwon IK, Matsuda T, Anderson JM (2007) Proteomic analysis and quantification of cytokines and chemokines from biomaterial surface-adherent macrophages and foreign body giant cells. J Biomed Mater Res 83A:585–596
Jones JA, McNally AK, Chang DT, Colton E, Kwon IK, Matsuda T, Anderson JM (2007) Matrix metalloproteinases and their inhibitors in the foreign body reaction on biomaterials. J Biomed Mater Res 84A:158–166
Brodbeck WG, Nakayama Y, Matsuda T, Colton E, Ziats NP, Anderson JM (2002) Biomaterial surface chemistry dictates adherent monocyte/macrophage cytokine expression in vitro. Cytokine 18:311–319
Brodbeck WG, Voskerician G, Ziats NP, Nakayama Y, Matsuda T, Anderson JM (2003) In vivo leukocyte cytokine mRNA responses to biomaterials is dependent on surface chemistry. J Biomed Mater Res 64A:320–329
Anderson JM, Schoen FJ (2004) Chapter 5.3. In vivo assessment of tissue compatibility. In: Ratner BD, Hoffman AS, Schoen FJ, Lemons JE (eds) Biomaterials science: an introduction to materials in medicine. Elsevier, New York, pp 360–367
Chambers TJ, Spector WG (1982) Inflammatory giant cells. Immunobiol 161:283–289
Anderson JM (2000) Multinucleated giant cells. Curr Opin Hematol 7:40–47
Zhao QH, Anderson JM, Hiltner A, Lodoen GA, Payet CR (1992) Theoretical analysis on cell size distribution and kinetics of foreign body giant cell formation in vivo on polyurethane elastomers. J Biomed Mater Res 26:1019–1038
Anderson JM, Schoen FJ, Brown SA, Merritt K (2004) Chapter 9.5. Implant retrieval and evaluation. In: Ratner BD, As Hoffman, Schoen FJ, Lemons JE (eds) Biomaterials science: an introduction to materials in medicine. Elsevier, New York, pp 771–782
Zhao Q, Topham NS, Anderson JM, Hiltner A, Lodoen G, Payet CR (1991) Foreign body giant cells and polyurethane biostability: in vivo correlation of cell adhesion and surface cracking. J Biomed Mater Res 25:177–183
Anderson JM (2004) Chapter 4.2. Inflammation, wound healing, and the foreign body response. In: Ratner BD, Hoffman AS, Schoen FJ, Lemons JE (eds) Biomaterials science: an introduction to materials in medicine. Elsevier, New York, pp 296–304
Wiggins MJ, Wilkoff B, Anderson JM, Hiltner A (2001) Biodegradation of polyether polyurethane inner insulation in bipolar pacemaker leads. J Biomed Mater Res (Appl Biomater) 58:302–307
McNally AK, Anderson JM (1995) Interleukin-4 induces foreign body giant cells from human monocytes/macrophages. Differential lymphokine regulation of macrophage fusion leads to morphological variants of multinucleated giant cells. Am J Pathol 147:1487–1499
DeFife KM, Jenney CR, McNally AK, Colton E, Anderson JM (1997) Interleukin-13 induces monocyte macrophage fusion and macrophage mannose receptor expression. J Immunol 158:3385–3390
McNally AK, Anderson JM (2003) Foreign body-type multinucleated giant cell formation is potently induced by α-tocopherol and prevented by the diacylglycerol kinase inhibitor R59022. Am J Pathol 163:1147–1156
McNally AK, Anderson JM (1996) The lymphokine interleukin-4 induces foreign body giant cell formation from human macrophages in a material surface property-dependent manner in vitro. Fifth World Biomaterials Congress, May 29-June 2, Toronto, Canada
Jenney CR, DeFife KM, Colton E, Anderson JM (1998) Human monocyte/macrophage adhesion, macrophage motility, and IL-4 induced foreign body giant cell formation on silane modified surface in vitro. J Biomed Mater Res 41:171–184
Jenney CR, Anderson JM (1999) Effects of surface-coupled polyethylene oxide on human macrophage adhesion and foreign body giant cell formation in vitro. J Biomed Mater Res 44:206–216
Jenney CR, Anderson JM (1999) Alkylsilane-modified surfaces: inhibition of human macrophage adhesion and foreign body giant cell formation. J Biomed Mater Res 46:11–21
Brodbeck WG, Patel J, Voskerician G, Christenson E, Shive MS, Nakayama Y, Matsuda T, Ziats NP, Anderson JM (2002) Biomaterial adherent macrophage apoptosis is increased by hydrophilic and anionic substrates in vivo. Proc Natl Acad Sci USA 99:10287–10292
Collier TO, Anderson JM, Brodbeck WG, Barber T, Healy KE (2004) Inhibition of macrophage development and foreign body giant cell formation by hydrophilic interpenetrating polymer network. J Biomed Mater Res A 69:644–650
Gordon S (2003) Alternative activation of macrophages. Nat Rev Immunol 3(23):25–35
Brigelius-Flohe R, Traber MG (1999) Vitamin E: function and metabolism. EMBO J 13:1145–1155
Azzi A, Stocker A (2000) Vitamin E: non-antioxidant roles. Prog Lipid Res 39:231–255
Stein M, Keshav S, Harris N, Gordon S (1992) Interleukin-4 potently enhances murine macrophage mannose receptor activity: a marker of alternative immunologic macrophage activation. J Exp Med 176:287–292
Goerdt S, Politz O, Schledzewski K, Birk R, Gratchev A, Guillot P, Hakiy N, Klemke CD, Dippel E, Kodelja V, Orfanos CE (1999) Alternative versus classical activation of macrophages. Pathobiology 67:222–226
Taylor PR, Martinez-Pomares L, Stacey M, Lin HH, Brown GD, Gordon S (2005) Macrophage receptors and immune recognition. Ann Rev Immunol 23:901–944
Mantovani A, Sica A, Locati M (2007) New vistas on macrophage differentiation and activation. Eur J Immunol 37:14–16
Kao WJ, McNally AK, Hiltner A, Anderson JM (1995) Role for interleukin-4 in foreign-body giant cell formation on a poly(etherurethane urea) in vivo. J Biomed Mater Res 29:1267–1275
Gessner A, Mohrs K, Mohrs M (2005) Mast cells, basophils, and eosinophils acquire constituitive IL-4 and IL-13 transcripts during lineage differentiation that are sufficient for rapid cytokine production. J Immunol 174:1063–1072
Drachman DE, Simon DI (2005) Inflammation as a mechanism and therapeutic target for in-stent restenosis. Curr Artheroscler Rep 7:44–49
Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold HK, Virmani R (2006) Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol 48:203–205
Wisniewski N, Moussy F, Reichert WM (2000) Characterization of implantable biosensor membrane biofouling. Fresenius J Anal Chem 366:611–621
Anderson JM (2008) Biocompatibility and bioresponse to biomaterials. In: Atala A, Lanza R, Thomson JA, Nerem RM (eds) Principles of regenerative medicine. Elsevier, New York, pp 704–723
Brodbeck WG, MacEwan M, Colton E, Meyerson H, Anderson JM (2005) Lymphocytes and the foreign body response: lymphocyte enhancement of macrophage adhesion and fusion. J Biomed Mater Res 74A:222–229
MacEwan MR, Brodbeck WG, Matsuda T, Anderson JM (2005) Monocyte/lymphocyte interactions and the foreign body response: in vitro effects of biomaterial surface chemistry. J Biomed Mater Res 74A:285–293
Chang DT, Jones JA, Meyerson H, Colton E, Kwon IK, Matsuda T, Anderson JM (2008) Lymphocyte/macrophage interactions: biomaterial surface-dependent cytokine, chemokine, and matrix protein production. J Biomed Mater Res 87A:676–687
Chang DT, Colton E, Anderson JM (2008) Paracrine and juxtacrine lymphocyte enhancement of adherent macrophage and foreign body giant cell activation. J Biomed Mater Res 89A:490–498
Chang DT, Colton E, Matsuda T, Anderson JM (2009) Lymphocyte adhesion and interactions with biomaterial adherent macrophages and foreign body giant cells. J Biomed Mater Res 91A:1210–1220
Rodriguez A, Voskerician G, Meyerson H, MacEwan S, Anderson JM (2008) T cell subset distributions following primary and secondary implantation at subcutaneous biomaterial implant sites. J Biomed Mater Res 85A:556–565
Rodriguez A, Meyerson H, Anderson JM (2008) Quantitative in vivo cytokine analysis at synthetic biomaterial implant sites. J Biomed Mater Res 89A:152–159
Ankersmit HJ, Tugulea S, Spanier T, Weinberg AD, Artrip JH, Burke EM, Flannery M, Mancini D, Rose EA, Edwards NM, Oz MC, Itescu S (1999) Activation induced T cell death and immune dysfunction after implantation of left-ventricular assist device. Lancet 354:550–555
Itescu S, Ankersmit HJ, Kocher AA, Schuster MD (2000) Immunobiology of left ventricular assist devices. Prog Cardiovasc Dis 43:67–80
Bender BS, Curtis JL, Nagel JE, Chrest FJ, Kraus ES, Briefel GR, Adler WH (1984) Analysis of immune status of hemodialyzed adults: association with prior transfusions. Kidney Int 26:436–443
Grooteman MP, Nube MJ, van Limbeek J, Schoor M, van Houte AJ (1996) Lymphocyte subsets in dialyser eluates: a new parameter of bioincompatibility? Nephrol Dial Transplant 11:1073–1080
Raij L, Kay NE (1987) Effect of hemodialysis membranes on human lymphocyte natural killer function. Contr Nephrol 59:17–25
DeFranco AL, Weiss A (1998) Lymphocyte activation and effector functions. Curr Opin Immunol 10:243–267
DiSanto JP (2006) Natural killer cell developmental pathways: a question of balance. Annu Rev Immunol 24:257–286
Schuster M, Kocher A, Lietz K, Ankersmit J, John R, Edwards N, Oz M, Itescu S (2001) Induction of CD40 ligand expression in human T cells by biomaterials derived from left ventricular assist device. Transplant Proc 33:1960–1961
Clarkson MR, Sayegh MH (2005) T cell costimulatory pathways in allograft rejection and tolerance. Transplantation 80:555–563
Guerder S, Meyerhoff J, Flavell RA (1994) The role of the T cell costimulator B7. In autoimmunity and the induction and maintenance of tolerance to peripheral antigen. Immunity 1:155–166
Reed JC (2000) Mechanisms of apoptosis. Am J Pathol 157:1415–1430
Ward SG, Westwick J (1998) Chemokines: understanding their role in T-lymphocyte biology. Biochem J 333:457–470
Houssiau FA, Coulie PG, Van Snick J (1989) Distinct roles of IL-1 and IL-6 in human T cell activation. J Immunol 143:2520–2524
Maghazachi AA, Al-Aoukaty A, Schall TJ (1996) CC chemokines induce the generation of killer cells from CD56+ cells. Eur J Immunol 26:315–319
Monaco C, Andreakos E, Kiriakidis S, Feldmann M, Paleolog E (2004) T-cell-mediated signaling in immune, inflammatory and angiogenic processes: the cascade of events leading to inflammatory diseases. Curr Drug Targets Inflamm Allergy 3:35–42
Burger D, Dayer JM (2002) Cytokines, acute-phase proteins, and hormones: IL-1 and TNF-alpha production in contact-mediated activation of monocytes by T lymphocytes. Ann NY Acad Sci 966:464–473
Beech JT, Andreakos E, Ciesielski CJ, Green P, Foxwell BM, Brennan FM (2006) T-cell contact-dependent regulation of CC and CXC chemokine production in monocytes through differential involvement of NFkappaB: implications for rheumatoid arthritis. Arthritis Res Ther 8:R168
Mantovani A, Sica A, Sozzani S, Allavena P, Vecchi A, Locati M (2004) The chemokine system in diverse forms of macrophage activation and polarization. Trends Immunol 25:677–686
Groux H, Bigler M, de Vries JE, Roncarolo MG (1996) Interleukin-10 induces a long-term antigen-specific anergic state in human CD4+ T cells. J Exp Med 184:19–29
Isomaki P, Clark JM, Panesar M, Cope AP (2005) Pathways of T cell activation and terminal differentiation in chronic inflammation. Curr Drug Targets Inflamm Allergy 4:287–293
Gupta S, Ruifen BI, Gollapudi S (2006) Central memory and effector memory subsets of human CD4+ and CD8+ T cells display differential sensitivity to TNF-α-induced apoptosis. Ann NY Acad Sci 1050:108–114
Brodbeck WG, Shive MS, Colton E, Nakayama Y, Matsuda T, Anderson JM (2001) Influence of biomaterial surface chemistry on the apoptosis of adherent cells. J Biomed Mater Res 55:661–668
Brodbeck WG, Shive MS, Colton E, Ziats NP, Anderson JM (2002) Interleukin-4 inhibits tumor necrosis factor-alpha-induced and spontaneous apoptosis of biomaterial-adherent macrophages. J Lab Clin Med 139:90–100
Zingoni A, Sornasse T, Cocks BG, Tanaka Y, Santoni A, Lanier LL (2005) NK cell regulation of T cell-mediated responses. Mol Immunol 42:451–454
O’Connor GM, Hart OM, Gardiner CM (2006) Putting the natural killer cell in its place. Immunology 117:1–10
Lodoen MB, Lanier LL (2006) Natural killer cells as an initial defense against pathogens. Curr Opin Immunol 18:391–398
Van Kaer L (2007) NKT cells: T lymphocytes with innate effector functions. Curr Opin Immunol 19:354–364
Moretta A, Marcenaro E, Parolini S, Ferlazzo G, Moretta L (2008) NK cells at the interface between innate and adaptive immunity. Cell Death Differ 15:226–233
Keegan AD (2001) IL-4. In: Oppenheim JJ, Feldman M (eds) Cytokine reference. Academic, San Diego
McKenzie ANJ, Matthews DJ (2001) IL-13. In: Oppenheim JJ, Feldman M (eds) Cytokine reference. Academic, San Diego
Kronenberg M (2005) Toward an understanding of NKT cell biology: progress and paradox. Ann Rev Immunol 26:877–900
Rodriguez A, MacEwan SR, Meyerson H, Kirk JT, Anderson JM (2009) The foreign body reaction in T-cell-deficient mice. J Biomed Mater Res 90A:106–113
De Lalla C, Galli G, Aldrighetti L, Romeo R, Mariani M, Monno A, Nuti S, Colombo M, Callea F, Porcelli SA, Panina-Bordignon P, Abrignani S, Casorati G, Dellabona P (2004) Production of pro-fibrotic cytokines by invariant NKT cells characterizes cirrhosis progression in chronic viral hepatitis. J Immunol 173:1417–1425
Fuss IJ, Heller F, Boirivant M, Leon F, Yoshida M, Fichtner-Feigl S, Yang Z, Exley M, Kitani A, Blumberg RS, Mannon P, Strober W (2004) Non-classical CD1d-restricted NK T cells that produce IL-13 characterize an atypical Th2 response in ulcerative colitis. J Clin Invest 113:1490–1497
Fichtner-Feigl S, Strober W, Kawakami K, Puri RK, Kitani A (2006) IL-13 signaling through the IL-13α2 receptor is involved in induction of TGF-β1 production and fibrosis. Nature Med 12:99–106
Santana MA, Rosenstein Y (2003) What it takes to become an effector T cell: the process, the cells involved, and the mechanisms. J Cell Physiol 195:392–401
Kyriakides TR, Foster MJ, Keeney GE, Tsai A, Giachelli CM, Clark-Lewis I, Rollins BJ, Bornstein P (2004) The CC chemokine ligand, CCL2/MCP1, participates in macrophage fusion and foreign body giant cell formation. Am J Pathol 165:2157–2166
Pesce J, Kaviratne M, Ramalingam TR, Thompson RW, Urban JF, Cheever AW, Young DA, Collins M, Grusby MJ, Wynn TA (2006) The IL-21 receptor augments Th2 effector function and alternative macrophage activation. J Clin Invest 116:2044–2055
Acknowledgment
The authors gratefully acknowledge the support of the National Institutes of Health, Institute of Biomedical Imaging and Bioengineering, Grant EB-00282.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is published as part of the Special Issue on Implanted Devices: Biocompatibility, Tissue Engineering and Infection
Rights and permissions
About this article
Cite this article
Anderson, J.M., McNally, A.K. Biocompatibility of implants: lymphocyte/macrophage interactions. Semin Immunopathol 33, 221–233 (2011). https://doi.org/10.1007/s00281-011-0244-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00281-011-0244-1