
Abstract
Purpose
The aim of this study was to evaluate whether combination of antioxidants and mesna may prevent cystitis induced by cyclophosphamide better than mesna alone.
Materials and methods
A total of 46 male Spraque-Dawley rats were divided into six groups. Five groups received single dose of cyclophosphamide (CP, 100 mg/kg) intraperitoneally with the same time intervals: group 2 received CP only, group 3 received mesna (21.5 mg/kg for three times), group 4 beta-carotene (20 mg/kg for two times) and mesna, group 5 received alpha-tocopherol (20 mg/kg for two times) and mesna, and group 6 received melatonin (5 mg/kg for two times) and mesna on the day of CP injection. Group 1 served as control.
Results
CP injection resulted in severe cystitis. Mesna has showed meaningful but not full protection against CP toxicity. Although beta-carotene did not show any additional beneficial effect when combined with mesna, alpha-tocopherol and especially melatonin with mesna resulted full protection that the pathologist, blinded to the slides, could not differ from sham control.
Conclusion
Oxidants may be important in the pathogenesis of CP-induced cystitis. Melatonin and alpha-tocopherol may help to ameliorate bladder damage along with other drugs such as mesna and diuretics.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cyclophosphamide (CP) is in the nitrogen mustard group of alkylating antineoplastic chemotherapeutic agents. It is used alone or in combination with other chemotherapeutic agents for the treatment of many neoplastic diseases [6]. Hemorrhagic cystitis (HC) is a major potential toxicity and dose limiting side effect of CP and ifosfamide, a synthetic analog of CP [19]. The incidence of this side effect is related to the dosage and can be as high as 75% in patients receiving a high intravenous dose. The urological side effects vary from transient irritative voiding symptoms, including urinary frequency, dysuria, urgency, suprapubic discomfort, and stangury with microhematuria, to life-threatening HC [8]. Bladder fibrosis, necrosis, contracture, and vesicoureteral reflux and a 4% percent mortality rate among patients with massive bladder hemorrhage have also been reported [6, 19]. The Urotoxicity of these nitrogen mustard group cytostatics is not based on a direct alkylating activity on urinary system but the formation of renally excreted 4-hydroxy metabolites, in particular acrolein, which is formed from hepatic microsomal enzymatic hydroxylation [10].
Mesna contains a sulfhydryl compound which binds acrolein within the urinary collecting system and detoxifies it; the resultant inert thioether is passed innocuously in the urine and does not induce any damage to the uroepithelium [7, 10]. Although mesna has been widely used as an effective agent against CP-induced cystitis, significant HC, defined as an episode of symptomatic (burning, frequency and dysuria), microscopic or macroscopic hematuria, has still been encountered clinically.
Recently, it has been shown that increasing nitric oxide (NO) production is responsible for the detrimental effects of CP on bladder [9, 15, 16]. This toxicity probably comes from reactive nitrogen species (RNS), in particular peroxynitrite (ONOO−) overproduction by reacting NO and superoxide (O2 •−)which appears abundantly inflammatory area [17]. Moreover it is clear that, in biological systems the primary source of all RNS is NO. The overproduction of reactive oxygen species (ROS) and RNS during inflammation leads to a considerable oxidant stress, cellular injury and necrosis via several mechanisms including peroxidation of membrane lipids, protein denaturation and DNA damage [18].
Thwarting the damage inflicted by free radicals and reactive species is the function of a complex antioxidative defense system. This system includes some enzymes such as superoxide dismutase (SOD), catalase (CAT) and glutathione peroxidase (GPx) [12] and some of the most commonly used and experimentally studied non-enzyme antioxidants, such as β-carotene, α-tocopherol and melatonin [4]. These agents are key elements in reducing molecular damage due to reactive oxygen and nitrogen species and there is extensive literature, which describes their multiple actions.
Since detoxifying acrolein with mesna cannot remove HC symptoms completely and NO has been shown to involve in the pathogenesis, CP induced HC is probably not only due to direct contact of acrolein with bladder mucosa but also related to increased ROS and RNS production. In this study we examined, whether combination of antioxidants with mesna may show better result than mesna alone in CP induced bladder damage.
Materials and methods
Animals
A total of 46 male rats, with body weights of 270–340 g were divided into six groups by “simple random sampling method” and given food and water ad libitum. Amount of water consumed by each animal was measured to avoid the hiperhydrative effect of water. The Gulhane Military Medical Academy Animal Care and Use Committee approved the experimental protocol.
Drug administrations
The drug administration schedule is presented in Table 1.
Experimental induction of HC
The animals were given urotoxic dose of 100 mg/kg CP in 2 ml saline. Group 1 animals were injected with the same amount of saline and served as control.
Mesna and antioxidants administrations
64.5 mg/kg mesna was administred 20 min before CP injection, and continued every 4 h for a total of three equal doses. Beta-carotene (2×20 mg/kg), alpha-tocopherol (2×20 mg/kg), melatonin (2×5 mg/kg) were given 12 and 1 h before CP administration. All injections were performed intraperitoneally (i.p.).
Tissue preparation
Twenty-four hours after CP administration, animals were sacrificed using high i.p. injection of ketamine HCl and xylazine HCl to prevent inadvertent bladder puncture. The bladders were removed intact, evacuated residual urine, cleaned from connective and lipoid tissue around the wall, weighed, and fixed for 24 h in 10% buffered formalin. Standart paraffin blocks, as well as hematoxylin and eosin-stained slides, were prepared. The pathologist, who had no knowledge of which of the six groups each slide belonged to, rated the mean histologic damage, including ulceration, hemorrhage and edema, on a scale of 1 (light) to 4 (severe changes). Normal bladder of control group rated as 0.
Definitions of hematuria
Hematuria was graded on a scale of 0–3 by performing dip-stick analysis in the urine specimens obtained by abdominal massage at 6, 12 and 24 h after CP injection.
Statistics
The results are expressed as the median (min–max) and p<0.05 was assessed as statistically significant. All of the numeric data were analyzed first using nonparametric Kruskal–Wallis test to find whether there is difference between groups and then Mann–Whitney U-test was performed to analyze two groups consecutively.
Results
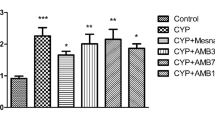
The animals in control had cytologically normal bladders with assigned scores of 0 for all three parameters, namely edema, hemorrhage, and ulceration. Animals receiving CP (group 2) had shown severe cytologic changes and higher grades of hematuria. Unscored cytologic features peculiar to the slides of this group included mucosal sloughing and hemorrhagic areas (Figs. 1, 2). Moreover, severe ulceration and erosion had been encountered in five of seven bladders as shown in Fig. 3. No ulceration was observed in any other slides.

Scale of rat bladder histology for edema from 1 (+; light) to 4 (++++; severe) (H&E, approx. 100×) (+ from group 6, ++ from group 5, +++ from group 3 and ++++ from group 2)

Scale of rat bladder histology for hemorrhage from 1 (+; light) to 4 (++++; severe) (H&E, approx. 100×) (+ from group 6, ++ from group 5, +++ from group 3 and ++++ from group 2)

Scale of rat bladder histology for ulceration from 1 (+; light) to 4 (++++; severe) (H&E, approx. 100×) (+ from group 5, ++ from group 4, +++ from group 3 and ++++ from group 2)
In treatment group received mesna only, statistically significant protection was observed for ulceration as shown in Table 2 (p<0.05 compared with CP), histologic damages were present for edema and hemorrhage (p>0.05 compared with CP) (Figs. 1, 2).
Addition of beta-carotene to mesna did not show more significant protection than mesna alone. Alpha-tocopherol (p<0.05 for hemorrhage compared with group 3) and melatonin (p<0.05 for hemorrhage and edema compared with group 3) are both revealed protective properties along with mesna. Hematuria was continued in CP group and almost disappeared in treatment groups.
Discussion
CP, an antineoplastic alkylating agent, is used to treat neoplastic, immune mediated and transplant related diseases and its use is likely to increase as new applications are discovered. HC is a major therapy-limiting side effect of CP. It is thought to be induced by acrolein, a cytotoxic metabolite of CP, which is excreted in the urine. The main futures of HC are urothelial damage, transmural edema, hemorrhage, mucosal ulceration and epithelial necrosis which could be demonstrated within 24 h of a single dose [8]. Mucosal sloughing has been associated frequently with acute and chronic hemorrhage. Within the first several hours, epithelial cells in the superficial mucosal layer of the bladder begin undergo degeneration and necrosis. At 18 h post-injection, most of the mucosal lining is eroded or ulcerated, and basal membrane damage is evident with subsequent damage of the surrounding capillaries. Thereafter, healing began with evidence of mucosal hyperplasia and bizarre papillary proliferation. Neovascularisation and leukocyte infiltration may also be seen following days [2].
Among various prophylactic and therapeutic measures to treat HC, mesna showed the most promising results. Its toxicity is negligible and oxidized to a stable inactive disulfide within minutes of parenteral administration and becomes active when excreted into the urine. Mesna combines with acrolein in the urine to form an inert, nontoxic thioester and allows maximum therapeutic effect of the alkylating oxazaphosphorine drug. In addition to neutralizing acrolein, it slows the degradation of the 4-hydroxy-metobolites of the alkylating agent [7, 10]. However, although mesna has showed an effective uroprotection, HC still occurs in 10–40% of mesna-treated patients.
CP induced HC is now known that NO is involved the pathogenesis [9] and bladder epithelial cells have also been shown to express intense reactivity to iNOS in the cytoplasm leading to peroxynitrite production [16]. Studies suggest that increased NO production, possible through iNOS activation, is responsible the cystitis since S-methylisothiourea (iNOS selective inhibitor) almost abolished bladder damage [15]. In a recent study antioxidants have been shown protective effect on bladder damage [data not shown]. This histological improvement is thought to be resulted from decreasing ROS and RNS production.
Over the last few years, the overall picture of the inflammatory process has been complicated by the potential pathogenetic contribution of ROS and RNS. A great variety of stimuli such as immune complexes, and inflammatory cytokines are able to up-regulate expression and synthesis of iNOS. Furthermore, it is now well recognized that ROS and RNS may interact with each other, resulting not only in the induction of further new reactive species, but above all, in possible changes in the concentration of these two classes of molecules [1]. There is no doubt that the overproduction of ROS and the majority of NO produced during inflammation are converted to peroxynitrite anion [13]. NO is the only currently known biological molecule produced in high enough concentrations to react fast enough with superoxide (forming ONOO−) to outcompete endogenous SOD [3].
The formation of ONOO− may be double edged sword. First, NO neutralizes a potentially deleterious species of oxygen radical, the superoxide radical. On the other hand, the reaction consumes NO and produces a potentially deleterious metabolite, ONOO−. Inflammatory cells such as PMNs and macrophages, but also endothelial cells can release superoxide and NO, potentially leading to peroxynitrite formation. Their release can be mediated and regulated by several cytokines. It is clear that overproduction or uncontrolled formation of peroxynitrite is an important factor in the tissue damaging mechanisms during pathological situations [1]. There are several experimental reports suggesting the formation of peroxynitrite during the inflammatory process including ileitis, lung injury, and endotoxemia via iNOS activation [13].
Results of this study suggest that antioxidants especially alpha-tocopherol and melatonin may be helpful to ameliorate CP induced cystitis when combined with mesna. Moreover both melatonin and vitamin E alone have also shown protective effect against CP induced cystitis [unpublished data]. Melatonin is a newly discovered antioxidant and not only itself but also chief hepatic metabolite of melatonin, namely, 6-hydroxymelatonin, is also reportedly an effective free radical scavenger [11]. A recent study has also shown that melatonin can directly scavenge the peroxynitrite [5]. Beside this antioxidant action, melatonin is an iNOS inhibitor [4] and this feature may contribute to beneficial effects of melatonin against bladder damage. The weaker protective effect of β-carotene may be due to its limited antioxidant effect that is, quenching of singlet oxygen not superoxide anion [14].
In conclusion, α-tocopherol and melatonin ameliorated bladder damage possibly through scavenging ROS and RNS. Since α-tocopherol and melatonin are safe and cheap, future studies may focus on the efficacy of antioxidants alone or combination with other therapeutic modalities such as mesna and diuretics on HC caused by CP.
References
Beckman JS, Koppenol WH (1996) Nitric oxide, superoxide and peroxynitrite: the good, the bad, and the ugly. Am J Physiol 271C:1424–1437
Brock N, Pohl J, Stekar J (1981) Studies on the urotoxicity of oxazaphosphorine cytostatics and its prevention. I. Experimental studies on the urotoxicity of alkylating compounds. Eur J Cancer 17(6):595–607
Crow JP, Beckman JS (1996) The importance of superoxide in nitric oxide-dependent toxicity: evidence for peroxynitrite-mediated injury. Adv Exp Med Biol 387:147–161
Cuzzocrea S, Reiter RJ (2001) Pharmacological action of melatonin in shock, inflammation, and ischemia/reperfusion injury. Eur J Pharm 426:1–10
Gilad E, Cuzzocrea S, Zingarelli B, Salzman AL, Szabo C (1997) Melatonin is a scavenger of peroxynitrite. Life Sci 60:169–174
Gilbert CJ, Petros WP, Vredenburgh J, Hussein A, Ross M, Rubin P, Fehdrau R, Cavanaugh C, Berry D, McKinstry C, Peters WP (1998) Pharmacokinetic interaction between ondanstetron and cyclophosphamide during high-dose chemotherapy for breast cancer. Cancer Chemother Pharmacol 42:497–503
Goren MP, McKenna LM, Goodman TL (1997) Combined intravenous and oral mesna in outpatients treated with ifosfamide. Cancer Chemother Pharmacol 40:371–375
Gray KJ, Engelmann UH, Johnson EH, Fishman IJ (1986) Evaluation of misoprostol cytoprotection of the bladder with cyclophosphamide (cytoxan) therapy. J Urol 133:497–500
Korkmaz A, Oter S, Deveci S, Ozgurtas T, Topal T, Sadir S, Bilgic H (2003) Involvement of nitric oxide and hyperbaric oxygen in the pathogenesis of cyclophosphamide induced hemorrhagic cystitis in rats. J Urol 170:2498–2502
Kurovski V, Wagner T (1997) Urinary excretion of ifosfamide, 4-hidroxyfosfamide, 3- and 2-dechloroethylifosfamide, mesna, and dimesna in patients on fractionated intravenous ifosfamide and concomitant mesna therapy. Cancer Chemother Pharmacol 39:431–439
Maharaj DS, Anoopkumar-Dukie S, Glass BD, Antunes EM, Lack B, Walker RB, Daya S (2002) The identification of the UV degradants of melatonin and their ability to scavenge radicals. J Pineal Res 32:257–261
Mates JM, Perez-Gomez P, Nunez de Castro I (1999) Antioxidant enzymes and human disease. Clin Biochem 32:595–603
Muijsers RB, Folkerts G, Henricks PAJ, Hashjin GS, Nijkamp FP (1997) Peroxynitrite: a two faced metabolite of nitric oxide. Life Sci 60:1833–1845
Olson JA (1993) Molecular actions of carotenoids. Ann N Y Acad Sci 691:156–166
Oter S, Korkmaz A, Oztas E, Yildirim I, Topal T, Bilgic H (2004) Inducible nitric oxide synthase inhibition in cyclophosphamide induced hemorrhagic cystitis in rats. Urol Res 32:185–189
Ribeiro RA, Feritas HC, Campos MC, Santos CC, Figueiredo FC, Brito GA, Cunha FQ (2002) Tumor necrosis factor-α and interleukin-1β mediate the production of nitric oxide involved in the pathogenesis of ifosfamide induced hemorrhagic cystitis in mice. J Urol 67(5):2229–2234
Szabo C (1996) The pathophysiological role of role of peroxynitrite in shock, inflammation, and ischemia-reperfusion injury. Shock 6:79–88
Virag L, Szabo E, Gergely P, Szabo C (2003) Peroxynitrite-induced cytotoxicity: mechanism and opportunities for intervention. Toxicol Lett 141:113–124
West NJ (1997) Prevention and treatment of hemorrhagic cystitis. Pharmacotherapy 17(4):696–706
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yildirim, I., Korkmaz, A., Oter, S. et al. Contribution of antioxidants to preventive effect of mesna in cyclophosphamide-induced hemorrhagic cystitis in rats. Cancer Chemother Pharmacol 54, 469–473 (2004). https://doi.org/10.1007/s00280-004-0822-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-004-0822-1