
Abstract
Introduction
Although mild bone angulation with osseous enlargement often suggests fractures with callus formation, in some cases the diagnosis is synchondrosis.
Case Report
We present a rare variation of the chest wall in a 15-year-old male with a history of lymphoma. Bilateral multi-level posterior rib enlargements revealing mild 18F-fluorodeoxyglucose uptake were detected via positron-emission tomography/computed tomography. The variations were identified as healing fractures, although the more accurate diagnosis was determined to be multi-level posterior rib synchondroses with consecutive bridgings. Although variant bone anatomies are commonly seen in radiological practice, such multiple symmetrical posterior rib synchondroses associated with consecutive bridgings and articulations have not been clearly demonstrated before.
Conclusion
Awareness of such a rare combination of a well-known variation is crucial for radiologists to exclude malignancies, possibility of fracture and suspicion of child abuse.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aberrant articulation of ribs was first identified in 1944 by Etter, who found an incidence of aberrant articulation in 1 of 1290 first ribs [3]. Bowie and Jacopson later clarified that most cases reported as isolated first-rib fractures were actually misdiagnoses of aberrant articulations [1]. Aberrant articulations in any bone form focal enlargements that mimic a callus formation, while accessory bones often mimic avulsion fractures. Aberrant articulations with or without accessory bones are, therefore, sometimes referred to as jointed bones, pseudoartrosis or synchondrosis. To the best of our knowledge, the present report is the first to identify multiple synchondroses and consecutive posterior rib bridgings misdiagnosed as healing fractures.
Case report
A 15-year-old male with a history of lymphoma originating from intraparotid lymph nodes but no history of severe trauma was under follow-up using positron-emission tomography/computed tomography (CT). In the nuclear medicine department, bilateral focal enlargements in the posterior aspects of the fourth through ninth ribs exhibiting increased 18F-fluorodeoxyglucose (FDG) uptake (maximum standardised uptake value: 2.1) were misdiagnosed as healing posterior rib fractures (Fig. 1a). Radiological evaluation revealed consecutive synchondroses in the fourth through ninth ribs with mild angulations and intercostal bridgings. Axial-view CT depicted hypodense cartilaginous segments at the articulation level of the posterior ribs as articular surfaces (Fig. 1b) and air bubbles due to vacuum phenomena (Fig. 1b) within the articulations. The parasagittal view revealed clear consecutive rib bridgings (Fig. 1c). A three-dimensional (3D) coronal-view volume-rendered CT image demonstrated multi-level posterior rib bridgings with articulations (Fig. 2). Since no cortical or medullary lytic lesion or periosteal reaction was found, skeletal lytic metastases were excluded from consideration. Due to the vacuum phenomena and partial cartilaginous segment, the condition was diagnosed as aberrant posterior rib articulations.

a Bilateral mild 18F-fluorodeoxyglucose uptake in the posterior portion of the fourth through ninth ribs (open arrows) corresponding to the cartilaginous segment of the aberrant posterior rib articulation. b Axial view of the chest CT examination demonstrating angulation in the posterior aspect of the ribs and enlargement around a linear hypodense area (open arrow) due to the cartilaginous segment of the synchondrosis. A vacuum phenomenon (closed arrow) is shown within the contralateral synchondrosis. c Parasagittal view of chest CT revealing bridgings between consecutive posterior ribs

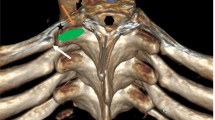
Coronal-plane 3D volume-rendered CT image demonstrating multi-level posterior rib bridgings among the consecutive ribs and articulations within the posterior part of the fourth through ninth ribs
Discussion
Embryologically, ribs originate in costal processes from thoracic somites, during whose segmentation rib anomalies can occur [7]. Both the chondrification and growth of the costae progress ventrally, and when the sternal plate meets the primordial costae, ossification begins. Thereafter, costovertebral joints develop and separate from the vertebrae. Rib anomalies, such as bifidity, fusion and bridging, all caused by aberrant segmentation, may be associated with abnormal sternal and vertebral segmentations [5]. During development of a synchondrosis, segmented unfused secondary ossification centres include a cartilaginous gap between the ossifying ends of the bones. Examples of physiological synchondroses are first-rib and manubrium sterni articulations, ischiopubic synchondroses and neonatal cranial sutures. In the case presented here, we observed a variant synchondrosis in addition to well-known variations, such as os acromiale, os odontoideum and cartilaginous tarsal coalition.
Among adolescents, the differential diagnosis of malignant processes presenting with sclerotic rib enlargements includes Ewing’s sarcoma and osteosarcoma. Patient history and the location and extension of lesions and accompanying CT findings should be evaluated together. Diffusely low-level FDG uptake in joints is more likely to be inflammatory or involve infection [6], as in the case presented, corresponding to the developmental process within the aberrant rib articulation before the fusion of the physis. A similar pitfall is an asymmetrically fused ischiopubic synchondrosis due to mild enlargement on conventional roentgenograms, increased signal on T2 weighted image and contrast enhancement on magnetic resonance imaging.
Benign tumoural entities can occur in the differential diagnosis of posterior rib enlargements, including multiple enchondromas, osteochondromas or chest wall hamartomas [8]. Hamartomas are generally heterogeneous and asymmetrical in size, shape and density. Osteochondromas are generally located in the costochondral junction and have continuance with the cortical and medullary portions of the affected bone. Deformation of the ribs can be observed in such benign entities, although the destruction of the cortex and periosteal reaction should consider malignant transformation [4]. Although 3D CT images demonstrate bridging ribs clearly, partially ossified synchondroses are better observed in thin-section images obtained perpendicularly to the articulation.
Distinguishing rib articulation anomalies from fractures is crucial in forensic medicine, especially amid suspicion of child abuse. Anterior–posterior compression is the most likely mechanism in most abused infants. When sufficient compression occurs, stress upon the ventral cortex of the posterior rib, where the rib tubercle articulates with the transverse process, results in a fracture. Multiple posterior rib fractures are believed to be quite specific to abuse [2]. The rare rib variation presented in our case can be described after the age that secondary ossification centres fuse. Otherwise, callus can form in all age groups, and history of high-energy trauma in any age group can mislead investigations, particularly in forensic medicine with patients showing such a rare variation.
Conclusion
Aberrant posterior rib articulations are extremely confusing not only for patients with malignancy but also in forensic medicine and post-traumatic investigations. In such cases, the presence of cartilaginous lines and vacuum phenomena can preclude suspicion of malignant processes and post-traumatic changes. Awareness of the variation can prevent its misdiagnosis as a severe injury as well as misguided medico-legal decisions.
References
Bowie ER, Jacobson HG (1945) Anomalous development of the 1st rib simulating isolated fracture. Am J Roentgenol 53(2):161–165
Bulloch B, Schubert CJ, Brophy PD, Johnson N, Reed MH, Shapiro RA (2000) Cause and clinical characteristics of rib fractures in infants. Pediatrics 105(4):e48-e48
Etter LE (1944) Osseous abnormalities of thoracic cage seen in forty thousand consecutive chest photoroentgenograms. Am J Roentgenol 51:359–363
Nam SJ, Kim S, Lim BJ, Yoon CS, Kim TH, Suh JS et al (2011) Imaging of primary chest wall tumors with radiologic-pathologic correlation. Radiographics 31(3):749–770
Scheuer L, Black S (2004) The juvenile skeleton. Academic Press, Cambridge
White ML, Johnson GB, Howe BM, Peller PJ, Broski SM (2016) Spectrum of benign articular and periarticular findings at FDG PET/CT. RadioGraphics 36(3):824–839
Yazici M (ed) (2011) Non-idiopathic spine deformities in young children. Springer Science & Business Media, New York
Yilmaz E, Erol OB, Pekcan M, Gundogdu G, Bilgic B, Gun F, Yekeler E (2015) Bilateral multifocal hamartoma of the chest wall in an infant. Pol J Radiol 80:283
Author information
Authors and Affiliations
Contributions
ZB Protocol/project development; Manuscript writing. RY Management. EC Editing. GB Data collection. FB Manuscript writing. SA Editing. IA Protocol/project development.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from the participant.
Rights and permissions
About this article

Cite this article
Bayramoglu, Z., Yilmaz, R., Caliskan, E. et al. A confounding rib variation: bilateral symmetric aberrant posterior rib articulations and bridgings. Surg Radiol Anat 40, 63–65 (2018). https://doi.org/10.1007/s00276-017-1937-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-017-1937-5