
Abstract
Objective
Different clinical problems may require a surgical approach to the dental arch, such as dentofacial orthopedics, implant-supported dental prothesis, maxillary orthodontics protraction, removable appliances, and posttraumatic dental reconstruction. The aim of this study is to analyze the dental arch size and type for supporting individual dental protheses.
Materials and methods
In this study, the reference measurements on the length of the bony palate, maxillary intercanine width, maxillary intermolar width, and the ratio of the maxillary to the palatinal surface were studied in 120 bony palates using a computer software program.
Results
The average length of the bony palate, maxilla, and palatine was measured as 104.4 ± 30.3, 40.05 ± 4.05, and 15.00 ± 3.03 mm, respectively. The right and left sides of average width of intermaxillary distances were measured as 13.75 ± 1.50 and 12.51 ± 1.50 mm, respectively. The average width of intermolar distance was calculated as 19.82 ± 1.61 mm (right side) and 18.89 ± 1.69 mm (left side), respectively. The maxillary dentitions were classified as square (17%), round-square (63.5%), round (14.4%), and round V-shaped arches (5.1%). The round-square ones showed no prominent principal component. Among the maxillary arches, the round arches were characterized by small values and round V-shaped ones with the largest values. Asymmetry between the right and the left bony palate was observed. The areas with equal bony palate on both sides were present in 64.4% of the cases, and in 33.1% of the cases, bony palate was dominant on the right.
Conclusions
The primary principle in reconstructive treatment should be describing geometrical forms and mathematical details of the bony palate. Three-dimensional reference values relative to the dental arch may increase the success of individual treatment of surgical procedures and reduce possible complications. With the help of certain software, this research has made possible to investigate the variability of the dental arch and calculate the variety in measurements and thereby determining the most appropriate implant position, optimizing the implant axis and defining the best surgical and prosthetic solution for the patient.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Numerous clinical problems, such as dentofacial orthopedics, implant-supported dental prothesis, maxillary orthodontics protraction, and obvious oral pathology, may require a surgical approach to the dental arch [6, 7, 16, 25]. Since hard bony palate restricts the function of swallowing and affects both the face and the chin esthetic directly, well-planned treatment is essential to improve the life quality of the patient [12, 13]. The first step is to conduct a detailed knowledge of the geometrical forms and mathematical value of the dental arch for personalized reconstruction [26, 28]. The main anatomical approach in bony palate problems is to determine the mathematical details, restore with suitable measurements, and repair the traumatic defect while preserving the bony palate area [10, 29].
It has been reported that the growth and the development period of dental arches have been influenced by a variety of causes, such as environmental factors, nutrition, and ethnic variations. Systemic, health, and individual variations could also take part during this period. In the previous studies, there have also been descriptive morphological studies differentiating upsilon, elliptique, parabolique, and hyperbolique dentitions [2, 4, 16]. The previous studies focused on morphometric types of the dental arch types and researches were limited within the anatomical landmarks [3, 23, 26]. Therefore, obtaining a standard measurement of dental arch has become more difficult in a great mixed population. Also these differences could affect the course of the clinical treatment.
While various efforts have been made to formulate a mathematical model for the dental arch in humans, the earliest description of the arch was via terms like elliptic, parabolic, etc. In addition, in terms of measurement, the arch circumference and the width were some of the previously used methods for measuring the dental arch curve (Figs. 1, 2, 3). Various experts have defined the dental arch curvature through the use of biometry by measuring the linear distances and the ratios [5, 7, 14, 26]. Researchers also maintain that important considerations in defining the human dental arch through mathematical modeling like symmetry or asymmetry, objective, landmarks used, and required level of accuracy do influence the actual choice of the model made. Factors that determine satisfactory diagnosis in orthodontic treatment include the dental arch form and size [1, 5, 7, 17, 22]. Commonly used plaster model analysis is cumbersome, whereas many scanning tools, like laser, destructive and computer tomography scans, structured light, magnetic resonance imaging, and ultrasound techniques, do exist now for accurate 3D reconstruction of the human anatomy [15, 17]. Mathematical analysis of the bony palate can be applied successfully in various issues related to dentistry thanks to the advancements in computer imaging, digitalization, and computer analysis through state of heart software programs [13, 15].

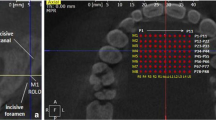
Measurement of the midpoint of the median palatine suture to posterior nasal spine using Image J 1.47 version

Measurements of the bony palate: Transverse lines; right (a) and left (b) widths of the maxilla at the incisive foramen; right (c) and left (d) widths of the maxilla at the median palatine suture. Two vertical lines intersected midpoints of the incisor edge to median palatine suture (e); midpoints of the median palatine suture to posterior nasal spine (f). a + b intercanine width, c + d intermolar width

Specimens with prominent widths in transverse lines a right dominant, b left dominant, and c equal specimen
The planning of surgical reconstruction significantly reduces functional and esthetic disorders which are reported in patients with maxillary deformity, malocclusion, and cleft lip and palate [18]. Primary repair in maxillary deformity should require orthognathic surgery. Several therapy factors, such as surgery, method of fixation, neuromuscular adaptation, and orthodontics, contribute to the treatment. The differences of the dental arch occurring as a result of growth and treatment have been interest to the orthodontist and are carefully considered during the treatment planning stage. Development in computer-aided technology has broadened diagnostic and interventional possibilities not only in general medicine, but also in implant dentistry, such as implant-supported dental prothesis, prosthetically driven implant placement and removable appliances [1, 3, 22, 27]. The electronic data, also obtained by the planning-process, can be directly transferred into the fabrication of surgical guides (stereolithography). Comprehensive knowledge on the mathematical detail of the bony palate is necessary as part of the surgical management of repairing, repositioning, reconstructing, and fabrication on the hard palate [7, 10, 13]. Treatment planning with computer-guided technique should focus on the anticipated esthetic and functional outcomes [3, 6, 28]. Many factors are considered in the planning of corrective surgery, such as dental arch, intercanine width, intermolar width, and the dentoalveolar relationship. The purpose of this article was to report the interdisciplinary collaboration of orthognathic surgery and prosthesis treatment.
Conducting a detailed oral examination is important in planning an individual treatment program for each dental patient. We have found limited studies using software program analyzing with the mathematical details and geometrical forms of the bony palate. This research aims at guiding clinical diagnosis and treatment which requires the study of dental arch forms, shape, size, and other parameters.
We proposed to analyze the dental arches with the reference measurements on the length of the bony palate, such as the intercanine width, intermolar width, ratio of the maxillary to palatinal surface, and skeletal asymmetry in adult hard palate. Using computer-assisted diagnostics in this study will enhanced the longevity of the maxillary bone, help perform implant-supported dental prothesis more effectively, and evaluate the removable application and put limitations to the three-dimensional computer technology in hypothetical indications.
Materials and methods
The study was conducted on 120 dry, unsexed, adult human skulls of the twentieth century available with the Anatolian population. None of them was affected by the maxillopalatinal abnormally or disrupted anatomically due to a previous maxillary surgery or trauma.
Photographs of the bony palate were taken with the macro model of a Nikon D 300 megapixel camera, in priority mode, with f7.1 diaphragm clarity. The bony palate was fixed horizontally and the images were taken by fixing the camera. The pictures were then uploaded onto a personal computer and software (last edition of National Institute of Health’s public software Image J 1.48v) was used to calculate the distances (Fig. 1). With the software, benchmarks were manually chosen and their distances to the maxillary bones were evaluated on the right and left sides separately (Fig. 2). In this study, we designated the midpoints of the incisor edge, median palatine suture, transverse palatine suture, posterior nasal spine, incisive foramen, and alveolar ridge to be as main reference points.
Lateral sulcus point
The point at which the lateral sulcus crosses the crest of the alveolar ridge.
Maxillary anterior arch width (a–b).
Maxillary posterior arch width (c–d).
Dental midline of the hard bony palate (e–f).
From the two vertical lines: intersected midpoints of the incisor edge to median palatine suture; midpoints of the median palatine suture to posterior nasal spine. From the transverse lines: right and left width of the maxilla at the incisive foramen (a–b); right and left width of the maxilla at the median palatine suture (c–d).
Asymmetries were measured by determining the absolute difference between homologous measurements as related to the reference lines (Figs. 2, 3). Possibility of irregularity in dental midline was also investigated. Dental midlines (e–f) were evaluated with posteroanterior photos. Correlation of dental midline to the maxilla and palatine was also evaluated (Figs. 2, 4).

Specimens with different ratio bony palate a classical ratio, b bigger maxilla, and c bigger palatine
Findings were analyzed using mean value, standard deviation, estimation of population mean with 95% confidence interval, and Student’s t test with levels of significance were set at α = 0.01 and α = 0.05).
The selection criteria were followed. The maxillary dental arches were classified as square, round-square, round, and round V-shaped arches with reference to the Thompson’s morphological descriptions [8].
The study was approved by the suitably constituted Ethical Committee at Researches Department of Ege University Hospital, within which the work was undertaken, and the study conforms to the Declaration of Helsinki (14.04.2011).
Results
The bony palate was formed by the palatine process of the maxillary and the horizontal plates of the palatine bones, meeting at a cruciform system of sutures. The median palatine suture ran anteroposteriorly and divided the bony palate into right and left halves, and it was continuous with the intermaxillary suture between the maxillary central incisor teeth. The transverse palatine sutures ran transversely across the palate between the maxillary and the palatine bones. The bony palate arched sagittally and transversely: its width and breadth were variable but were always the greatest in the molar region.
Bony palate measurements were as follows: The average length of the bony palate, length of the maxillary bone, and length of the palatine bone were as 104.4 ± 30.2, 40.05 ± 4.05, and 15 ± 3.03 mm, respectively. The mean average area of the right and the left bony palates was calculated as 520.77 ± 82.19 and 501.78 ± 72.71 mm2. The average width at intercanine distance was 13.75 ± 1.5 mm (right side) and 12.51 ± 1.5 mm (left side), respectively. The average intermolar distances were measured as 19.82 ± 1.61 mm (right side) and 18.89 ± 1.69 mm (left side). (Fig. 1b). Geometric calculations were summarized in Table 1.
As for the evaluation of the breadth of the bony palate, equal values of a–b and c–d were crucial in terms of symmetry (Figs. 2, 3). The right side was dominant in 33.1% (Fig. 3a), the left side was dominant 2.5% (Fig. 3b), and equal in 64.4% (Fig. 3c).
Maxilla palatine rate: classical ratio in 55.93% (Fig. 4a), bigger maxilla in 5.08% (Fig. 4b), and bigger palatine in 38.98% (Fig. 4c).
Maxillary dentitions were classified as square (17%), round-square (63.5%), round (14.4%), and round V-shaped arches (5.1%). Square dental arch had protruding canines with the anterior teeth and was arranged parallel bilaterally between the premolars and the molar (Fig. 5a). This type of dental arch was observed with 17% frequency. Round-square arch had a little canine protrusion resulting in a curved anterior teeth line; the posterior teeth were linearly aligned. The bilateral linearly aligned posterior teeth were nearly parallel in appearance. In this study, round-square arch was observed with 63.5% frequency (Fig. 5b). Round dental arch was seen as semicircle dental arch showing no canine protrusion and the incidence was 14.4%. This arch type was the smallest limit (Fig. 5c). Round V-shaped arch showed definite V-shaped anterior teeth arrangement (Fig. 5d) and was present in 5.1% of the specimen. Round V-shaped arch had large upper limit values (Fig. 5d).

Specimens with different alveolar arch. a Square, b round, c round-square, and d round V shape
Symmetrical hard bony palate without irregularities in dental midline was present in 51.7%, slight irregularities were in 38.1%, and asymmetry depending medium irregularity was present in 10.2% of the cases (Fig. 6 a,b).

Specimens of dental asymmetry and irregularities (arrow) of the intermaxillary suture
Discussion
The bony palate can be affected by a large number of congenital, traumatic, neo-plastic, vascular, and orthodontic disorders [6, 7, 9, 16, 18, 25]. Deformities, such as dentofacial orthopedics, implant-assisted dental reconstruction of oncology patients, and maxillary orthodontics protraction may require surgical approach to the bony palate [13].
Therefore, the ultimate goal should be the reconstruction of the bony palate with the restoration of proper anatomy, volume, function, and esthetics [9, 20, 21, 24]. Appropriate planning of surgical reconstruction significantly reduces functional and esthetic disorders in patients with maxillary deformity, malocclusion, and cleft lip and palate [18]. Orthognathic surgery, prostheses, and implants are expected to provide satisfactory results ensuring esthetic, functional, and psychological outcomes as part of the treatment [28]. Recent advances in imaging techniques and computer-aided simulation have added to the attempts to determine dental arch form [1, 13, 14, 19, 22]. Each bony palate had advantages and disadvantages, but none could exactly define the shape of the human dental arch curvature and its features like shape, symmetry/asymmetry, linear distances, and ratios. Asymmetry has been found to play a crucial role in its restoration as an essential problem in oral maxillofacial surgery [9, 11, 22]. The etiology of the asymmetry can be quite complex. In majority of the cases, it could be related to skeletal deformity. This is based on the principle that occlusal changes concerning the dental arch may lead to asymmetrical changes.
The findings of a large variation indicate that the dental arch form has no single and universal forms. These observations are strengthened by different facial patterns and stratified ethnic groups in this investigation. Some studies have reported that evaluation of the anterior teeth curvature and length-to-width ratio are determinant factors in the differentiation of maxillary dental arch forms [4]. Bishara et al. reported maxillary intercanine width as 34 ± 2.3, 32.3 ± 1.8 mm in post-eruption. Maxillary intermolar width was 53.6 ± 2.9, 48.3 ± 1.6 mm in post-eruption [4].
Nakatsuka et al. classification according to Thompson’s definition was as follows: 21.0% square, 58.1% round-square arches, 4.8% round arches, and 16.1% round V-shaped arches [23]. Square ones had prominent protrusion of canines and a linear arrangement of the anterior teeth leading to small upper and lower confidence limit values, which were significantly different from other arch types. The item showed significant differences between round V-shaped arches with long arch length. This is an essential parameter to differentiate round dental arches from the others. Another variable factor analysis on this study of the dental arch was the report that right/left ratio of the anterior teeth, the divergence of the molar segments, and the extent of the square shape of the anterior teeth had affected the dental arch forms deeply.
The appropriate timing and planning of surgical reconstruction significantly reduce functional and esthetic disorders in patients with cleft palate. The dental arch has emerged as an important part of esthetic dentistry for a variety reasons. The analyzed dental arch shapes have used conventional anatomical points on incisal edges and on molar cusp tips so as to classify forms of the dental arch through various mathematical details. The differences of teeth forms, such as shape, size, arch spacing, and curvature characterize a given sample for mathematical analysis, and also essentially vary with the nationality and ethnic origin of a child. Factors that determine satisfactory diagnosis in orthodontic treatment include teeth spacing and size, and the dental arch form and size. Anatomical details are important considerations in defining the human dental arch through mathematical modeling like symmetry or asymmetry, objective, landmarks used, and required level of accuracy which do influence the actual choice of model made. The computer-guided system of stereolithography used manages maxillary deformity, malocclusion, residual oronasal fistula, and bone defects in these patients and enhanced quality of life. Mathematical analysis can be applied satisfactory in various issues relating to dentistry and the advances in computer imaging, digitalization, and computer analysis through state-of-the-art software programs. The paper reports individual measurements which may present esthetic, functional, and psychological problems.
Using computer-guided technology in implant dentistry is more advantageous and safe in planning and controlling prospective implant axis in relation to the prosthetic bony palate position [10, 29]. It also leads to a higher quality of the treatment outcome with subsequent better patient information, fast implant placement, reduced cost, reduced chair side time, and a reduction of follow-up visits of the patients. Computer-guided system of stereolithography consists of three stages: (a) photographic analysis, including virtual implant planning; (b) formation of the surgical flapless procedure; and (c) immediate loading of a temporary prosthesis, within “1 h” as boosted by current marketing [6, 13, 15, 24]. In this study, computer-aided photometric methods were used to evaluate linear, area, and asymmetrical data of the bony palate. Given geometric values of the anatomical landmarks were defined (Fig. 1a, b). This study was conducted to evaluate longitudinal and transverse distances in dental asymmetry and to expand the knowledge on dental arch changes. Therefore, it is important to have extensive knowledge on the structure of the bony palate, observe the mathematical details of the curve and the area, and calculate linear distances, asymmetry, and their effect on bony palate reconstruction. In this study, we conducted analysis of items to standardize and summarize the dental arch form to be represented by three principal components. The results revealed that the first principal component was the parameter of intercanine distance, which was strongly affected by parameters. The second principal component, type of the dental arch, was mainly composed of the curvature of the anterior teeth. The third principal component was the dental asymmetry affected by the anterior maxillary region. In future, the research will be planned to analyze using structure sensor 3D scanner in patients with cleft palate population.
Different arch patterns or the existence of asymmetry may help reduce functional and esthetic disorders. The conclusion drawn out of this study may be individual modeling of reconstruction. Figure 7 devised for the results of study can be used to redesign and treat asymmetry with removable appliances of the bony palate [1, 6, 17, 24].

Round V-shaped arch palate (a) after the treatment with a removable appliance (b)
Conclusion
This study made possible to investigate the form and the arch dimensions of the hard palate, to provide detailed information on the characteristics of dental asymmetry, and to calculate the distances of palatal reference points with the help of using software. Final decision-making in implant prosthodontic treatment can be facilitated by an efficiently planned tool-based new computer technology. In compromised situations, this allows the surgeon to determine and evaluate the best position for the placement of the implant and the need for an additional surgical intervention. Using the computer technology also lets the surgeon predict the outcome of the treatment, allows for a better risk management, and assists to obtain more individual information for the patient. All in all, advanced technology contributes to set up higher quality standards in implantology.
References
Alcan T, Ceylanoglu C, Baysal B (2009) The relationship between digital model accuracy and time-dependent deformation of alginate impressions. Angle Orthod 79:30–36
Arslan SG, Kama JD, Sahin S, Hamamci O (2007) Longitudinal changes in dental arches from mixed to permanent dentition in a Turkish population. Am J Orthod Dentofac Orthop 132:e15–e21
Biggerstaff RH (1972) Three variations in dental arch form estimated by a quadratic equation. J Dent Res 51:1509
Bishara SE, Treder JE, Damon P, Olsen M (1996) Changes in the dental arches and dentition between 25 and 45 years of age. Angle Orthod 66(6):417–422
Camporesi M, Franchi L, Baccetti T, Antonini A (2006) Thin-plate spline analysis of arch form in a Southern European population with an ideal natural occlusion. Eur J Orthod 28:135–140
Chen ST, Buser D (2014) Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants 29(Suppl):186–215
Cheon S, Park Y, Paik K, Ahn S, Hayashi K, Yi W, Lee S (2008) Relationship between the curve of Spee and dentofacial morphology evaluated with a 3-dimensional reconstruction method in Korean adults. Am J Orthod Dentofacial Orthop 133:640.e7–640.e14
Currier JH (1969) Computerized geometric analysis of human dental arch form. Am J Orthod 56:164–179
Ferrario VF, Sforza C, Miani A Jr et al (1993) Dental arch asymmetry in young healthy human subjects evaluated by Euclidean-distance matrix analysis. Arch Oral Biol 38:189–194
Garino F, Garino GB (2002) Comparison of dental arch measurements between stone and digital casts. World J Orthod 3:250–254
Hunter WS (1953) Lateral asymmetries of 93 maxillary arches. Acta Odontol Scand 11:95–99
Janson GR, Metaxas A, Woodside DG, de Freitas MR, Pinzan A (2001) Three-dimensional evaluation of skeletal and dental asymmetries in class II subdivision malocclusions. Am J Orthod Dentofac Orthop 119(4):406–418
Katsoulis J, Pazera P, Mericske-Stern R (2009) Prosthetically driven, computer-guided implant planning for the edentulous maxilla: a model study. Clin Implant Dent Relat Res 11:238–245
Knott VB (1972) Longitudinal study of dental arch widths at four stages of dentition. Angle Orthod 42:387–394
Kupeyan HK, Shaffner M, Armstrong J (2006) Definitive CAD/CAM-guided prosthesis for immediate loading of bone-grafted maxilla: a case report. Clin Implant Dent Relat Res 8:161–167
Lagravere MO, Major PW, Flores-Mir C (2005) Long-term dental arch changes after rapid maxillary expansion treatment: a systematic review. Angle Orthod 75:155–161
Lombardo L, Saba L, Scuzzo G, Takemoto K, Oteo L, Palma JC, Siciliani G (2010) A new concept of anatomic lingual arch form. Am J Orthod Dentofacial Orthop 138:260.e1–260.e13
Lopes JF, Pinto JH, Lopes MM, Mazottini R, Soares S (2015) Interrelationship between implant and orthognathic surgery for the rehabilitation of edentulous cleft palate patients: a case report. J Appl Oral Sci 23(2):224–229
Louly F, Nouer PRA, Janson G, Pinzan A (2011) Dental arch dimensions in the mixed dentition: a study of Brazilian children from 9 to 12 years of age. J Appl Oral Sci 19(2):169–174
Lundström AS (1981) Intermaxillary tooth-width ratio analysis. Eur J Orthod 3:285–287
Lundström A, McWilliam JS (1984) Dento-alveolar compensation for antero-posterior variations between the upper and lower apical bases. Eur J Orthod 6:116–122
Minich CM, Araújo EA, Behrents RG, Buschang PH, Tanaka OM, Kim KB (2013) Evaluation of skeletal and dental asymmetries in angle class II subdivision malocclusions with cone-beam computed tomography. Am J Orthod Dentofac Orthop 144(1):57–66
Nakatsuka M, Iwai Y, Jue SS, Oh SH, Guo L, Tominaga Y, Kumabe S (2004) A morphological study on the classification of maxillary dental arches. Okajimas Folia Anat Jpn 81(1):5–13
Okunami TR, Kusnoto B, BeGole E, Evans CA, Sadowsky C, Fadavi S (2007) Assessing the American Board of Orthodontics objective grading system: digital vs plaster dental casts. Am J Orthod Dentofac Orthop 131:51–56
Ostman PO, Hellman M, Sennerby L (2005) Direct implant loading in the edentulous maxilla using a bone density-adapted surgical protocol and primary implant stability criteria for inclusion. Clin Implant Dent Relat Res 7(Suppl 1):S60–S69
Sampson PD (1981) Dental arch shape: a statistical analysis using conic sections. Am J Orthod 79:535–548
Shimada T (1988) A critical study on the classification of human dental and alveolar arches. J Antrop Soc Nippon 96:267–288
Zhang W, Skrypczak A, Weltman R (2015) Anterior maxilla alveolar ridge dimension and morphology measurement by cone beam computerized tomography (CBCT) for immediate implant treatment planning. BMC Oral Health 10(15):65
Zilberman O, Huggare JA, Parikakis KA (2003) Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod 73(3):301–306
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors certify that they have no potential conflicts of interest with any entity mentioned in this manuscript and that they received no specific financial support for this work.
Rights and permissions
About this article

Cite this article
Cagimni, P., Govsa, F., Ozer, M.A. et al. Computer-guided technique evaluation of the bony palate for planning individual implant placement. Surg Radiol Anat 39, 517–523 (2017). https://doi.org/10.1007/s00276-016-1765-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-016-1765-z