
Abstract
In patients with primary breast cancer, several large, randomized prospective trials have shown that sentinel node biopsy (SNB) substantially reduces the morbidity associated with axillary surgery compared with formal axillary lymph node dissection (ALND). Moreover, the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 trial has demonstrated that when the sentinel node reveals no evidence of metastatic disease, then no further ALND is required. Recently, the results of the American College of Surgeons Oncology Group (ACOSOG) Z0011 trial have challenged the notion that all patients with metastases to the sentinel node require ALND. The results of this trial suggest that in selected sentinel node-positive patients, ALND can be potentially avoided. Yet, some concerns about the ACOSOG Z0011 trial have been raised, and these concerns may have implications in the widespread implementation of the results of this trial. Since the advent of the SNB technology, occult metastases within the sentinel node are frequently observed, and the significance of these findings remains controversial. Finally, this review considers special situations, such as pregnancy and the neoadjuvant setting, where the use of SNB should be applied judiciously. The SNB technology has dramatically improved the quality of life for women with breast cancer, and further modifications of its role in breast cancer treatment should be based on evidence obtained from randomized, controlled trials.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Historical overview
The modern management of the axilla dates back to the 19th century. The German pathologist, Rudolf Virchow, undertook meticulous postmortem dissections and postulated that breast cancer arose from epithelial cells and spread in a contiguous fashion along fascial planes and lymphatics. Subsequently, William Halsted incorporated many of the tenets of Virchow’s hypothesis and argued that breast cancer was a locoregional disease that spread in a predictable and orderly fashion first to the regional lymph nodes and then to distant sites. He hence introduced the concept of a radical mastectomy that incorporated the en bloc removal of the entire breast along with the pectoral muscles and ipsilateral axillary nodes [1].
By the early 20th century, the Halsted radical mastectomy was widely accepted as the standard treatment for primary breast cancer. Yet, it was soon apparent that 30 % of node-negative patients died from metastatic breast cancer following radical mastectomy [2]. This observation was inconsistent with the Virchow-Halsted hypothesis that the lymph nodes serve as the sole nidus for distant spread of breast cancer. Furthermore, extended lymphadenectomies that involved removal of internal mammary and supraclavicular nodes did not show any survival benefit. By the 1960s, there was rising dissatisfaction with the radical mastectomy and alternative procedures received greater interest. Devitt [3] challenged the notion that the regional lymph nodes are important way-stations in the spread of breast cancer and suggested that lymph node metastases are only the expression of basic biological factors and not the cause of the poor outlook.
Soon after, the Virchow-Halsted hypothesis was tested in several randomized prospective trials. The National Surgical Adjuvant Breast and Bowel Project (NSABP) B-04 trial randomized 1,159 clinically node negative patients to radical mastectomy versus total mastectomy with postoperative axillary radiation versus total mastectomy followed by axillary dissection for those patients who subsequently developed clinically positive nodes. There was no difference in survival between the three treatment arms [2]. In the King’s/Cambridge trial, 2,243 women with early breast cancer were randomly assigned to either total mastectomy with immediate radiotherapy to the axilla versus careful observation of the axilla [4]. In the observation arm, radiotherapy was delayed until there was obvious progression of disease in the axilla. Again, there was no difference in survival between the two arms. Taken together, the NSABP-04 and Kings/Cambridge trials seem to indicate that the axillary nodes do not serve as the nidus for distant spread of breast cancer.
In these early studies, it was noted that approximately 40 % of the patients who underwent axillary lymph node dissections (ALND) had lymph nodes harboring metastases [2]. With widespread use of mammography screening and the increase in public awareness of the benefits of early breast cancer detection, this figure is far less today [5, 6]. The morbidities associated with ALND include lymphedema, sensory disturbances, limited arm mobility, and seroma formation [5, 7–12]. If node-negative patients could be identified appropriately, then the morbidity associated with ALND could be spared. In recent years, attention has turned to the sentinel node biopsy (SNB) technology as a means of achieving this goal. The sentinel lymph node is the first node to receive lymphatic drainage from a tumor. For any nodal basin, one might assume that if the sentinel lymph node is free of metastatic tumor, then all other nodes in the basin should be free of tumor as well. Thus, determining the status of the sentinel node could identify patients who may or may not benefit from ALND.
Kett et al. took one of the first steps toward evolution of sentinel node mapping techniques in patients with breast cancer when he observed breast lymphatics by injecting blue dye around the areola [13]. They noted that this blue dye terminated in the lymphatics around the axillary vein after traversing an isolated node, which they labeled the “Sorgius” node. In 1993, Krag et al. reported the identification of sentinel nodes in breast cancer patients using radiocolloid and a gamma probe [14]. Subsequently Giuliano et al. pioneered the use of blue dye mapping of sentinel nodes in breast cancer patients [15]. These investigators initially reported a sentinel node identification rate of 65.5 % using blue dye alone and found that the status of the sentinel node accurately predicted axillary nodal status in 109 of 114 (95.6 %) cases. Albertini in 1996 reported an identification rate of 92 % using a combination of blue dye and radio colloid [16]. Cox et al. further demonstrated in their series that 32 % and 40 % of sentinel nodes were labeled only with blue dye or radiocolloid respectively, but not both [17]. Morrow et al. conducted a prospective trial comparing use of blue dye alone versus a combination of blue dye and radiocolloid for the identification of the sentinel node and demonstrated no difference in identification rates [18]. In experienced hands, use of blue dye or radiocolloid (alone or in combination) is an acceptable method of sentinel lymph node identification.
Outcomes associated with sentinel node biopsy
During the past decade, the use of sentinel node biopsy (SNB) in the management of patients with primary breast cancer has been widely implemented into routine clinical practice. The use of SNB has been validated in the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 trial [19]. This trial randomized 5,611 women with clinically node-negative breast cancer either to SNB plus ALND or to SNB alone, with ALND performed only if there was evidence of metastasis to the sentinel nodes. With a median time of follow-up of 95.6 months, the overall survival, disease-free survival, and regional control were equivalent between the two groups. Thus, when the sentinel node reveals no evidence of metastatic disease, SNB alone with no further ALND appears to be a safe and effective therapy.
In this trial, a total of 1,975 ALND and 2,008 sentinel node-negative breast cancer patients had shoulder range of motion and arm volumes assessed along with self-reports of arm tingling and numbness [19]. Significant shoulder abduction deficits were seen in the ALND group compared with the SNB group at 6 months. Arm volume differences and numbness and tingling at 36 months also were significantly worse for the ALND groups.
Reduced morbidity with SNB compared with ALND has been reported in several other randomized control trials (Table 1). In the Axillary Lymphatic Mapping Against Nodal Axillary Clearance (ALMANAC) trial, Mansel et al. randomized 1,031 patients with primary breast cancer to SNB versus standard ALND [7]. The SNB group had a lower incidence of lymphedema, shorter drain usage and hospital stay, and reduced time to resumption of everyday activities compared with the ALND group. The relative risks of lymphedema and sensory loss for the SNB group compared with the ALND group at 12 months were 0.37 (95 % confidence interval (CI), 0.23–0.6), and 0.37 (95 % CI, 0.27–0.5) respectively, and patient-recorded quality of life and arm functioning scores were significantly better in the SNB group.
In a trial conducted in Milan, Veronesi et al. randomized 516 patients with tumor size 2 cm or less in diameter to SNB + ALND versus SNB followed by ALND only for patients with metastasis to the sentinel nodes [5]. After 2 years of follow-up, patients who underwent SNB alone had significantly less pain (8 % vs. 39 %), less numbness (1 % vs. 68 %), and better arm mobility (0 % vs. 21 %) compared with patients who had a routine ALND, indicating a significant quality of life (QoL) improvement with SNB alone.
The GIVOM (Gruppo Interdisciplinare Veneto di Oncologia Mammaria) trial randomized 697 patients to SNB versus ALND and reported significantly less lymphedema, movement restrictions, and numbness in patients who underwent SNB at 24 months of follow-up [9]. In addition, the investigators found that overall quality of life was better in the SNB group.
Purushotham et al. randomly assigned 298 patients with tumors less than 3 cm to ALND (control group) versus SNB followed by ALND only if sentinel nodes were positive (study group) [10]. They reported a significant reduction in postoperative arm swelling within the study with a mean difference of 35.4 cc in the arm volume and 70 % overall reduction in odds of lymphedema (P = 0.004). The rate of seroma formation also was less with the study group: 14 % versus 21 %, which was not significant (P = 0.1); however, 12 % of patients in the study group required aspiration compared with 20 % in control group. This difference approached statistical significance (P = 0.06). There also were significant reductions in sensory deficits in the study group compared with the control group, including numbness (48 % vs. 65 %), loss of sensitivity to light touch (57 % vs. 78 %), and pinprick (55 % vs. 76 %; P < 0.001). However, with prolonged follow-up, the benefit of SNB appeared to diminish.
The Sentinel Node versus Axillary Clearance (SNAC) trial sponsored by the Royal Australasian College of Surgeons (RACS) was another large, randomized trial designed to ascertain the effect of SNB versus ALND on morbidity [11]. This trial randomly assigned 1,083 patients to SNB versus routine ALND. An average increase in arm volume of 4.2 % vs. 2.8 % (P = 0.002) and a greater impairment of arm movement of 4.4 % vs. 2.5 % (P = 0.02) in the ALND group compared with the SNB group was reported at 1-year follow up.
In a prospective study performed by McLaughlin et al. on 963 patients, arm swelling was reported in 3 % of patients who underwent a SNB alone compared with 27 % of patients who underwent a SNB followed by ALND (P < 0.001) [12]. Greater body weight, higher body mass index (BMI) and infection or injury in the ipsilateral arm since surgery were found to be significant risk factors associated with lymphedema.
Kell et al. published the results of a meta-analysis of seven, randomized, controlled trials with a total of 9,608 patients, which examined the effect of SNB on morbidity [20]. The trials included were NSABP-B32, SNAC, GIVOM, ACOSOG Z0011, ALMANC, Milan, and Purushotham’s trial. This meta-analysis demonstrated a significant reduction in the risk of postoperative seroma (odds ratio (OR) = 0.4, P = 0.0071), wound infection (OR = 0.58, P = 0.0011), lymphedema (OR = 0.3, P = 0.0028), and extremity numbness (OR = 0.25, P = 0.0018) in the SNB group compared with the ALND group.
Occult metastases in the sentinel node
The American Joint Committee on Cancer (AJCC) has incorporated the size of sentinel node metastases into its pathological staging system [21]. The AJCC refers to foci of disease ≤0.2 mm as isolated tumor cells (pN0 (i+)), >0.2–2.0 mm as micrometastases (pN1mi), and >2.0 mm as macrometastases. With increasing use of immunohistochemistry, our ability to detect these occult metastases has improved. Weaver et al. reported outcome data for patients with micrometastases within the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 trial [22]. In this study, 3,887 paraffin-embedded tissue blocks of sentinel lymph nodes obtained from patients with pathologically negative sentinel lymph nodes were centrally evaluated for occult metastases. Using both hematoxylin and eosin and immunohistochemical staining for cytokeratin, occult metastases were detected in 15.9 % of the patients (300 patients in the SNB alone group and 316 in the ALND group). The 5-year overall survival among patients with occult metastases versus those without was 94.6 % and 95.8 %, respectively. The authors argued that this small difference in outcome (1.2 %) did not support routine use of IHC to detect occult metastases.
The American College of Surgeons Oncology Group (ACOSOG) undertook a prospective study (Z0010) to evaluate the incidence and impact of sentinel node and bone marrow micrometastases on outcome in patients with early-stage carcinoma of the breast treated with breast-conserving surgery (BCS) and radiation therapy [23]. Of 3,326 H&E-negative sentinel node specimens that were examined by immunohistochemistry, 349 (10.5 %) were positive for tumor. Although bone marrow micrometastases were associated with a significantly worse overall survival, sentinel lymph node micrometastases were not.
Sentinel node biopsy in pregnancy
In pregnant women, the diagnosis of breast cancer often is delayed and the tumors tend to be more aggressive. Radiation is contraindicated during pregnancy, chemotherapy is generally considered safe during second and third trimesters, and surgery under general anesthesia is considered reasonably safe, although it has been associated with an increased risk of spontaneous abortions [24]. Breast conservation is an acceptable option only if radiation is delayed to the postpartum period, so it often is appropriate for women diagnosed with breast cancer in late pregnancy and for patients who will require adjuvant chemotherapy before radiotherapy.
Approximately half of patients with breast cancer during pregnancy are clinically node-negative and could potentially benefit from sentinel node biopsy [25]. However, there are some challenges associated with sentinel node biopsy during pregnancy. Methylene blue is teratogenic and Lymphazurin has risks of anaphylaxis, which may increase the risk of fetal loss [26, 27]. Several investigators have reported that fetal exposure to the Tc99-m used in the radiocolloid appears to be safe, so sentinel node biopsy with an intraoperative gamma probe is perhaps an acceptable method of staging the axilla in this group of patients [28–31].
Sentinel node evaluation after neoadjuvant chemotherapy
The accuracy and appropriate timing of SNB in patients receiving neoadjuvant chemotherapy are important considerations. The concerns that arise in this setting pertain to lymphatic scarring and its implications on drainage pattern and the possibility of disproportionate tumor shrinkage in the sentinel node compared with nonsentinel nodes that may lead to a higher false-negative rate. Certainly, the use of sentinel node biopsy in inflammatory breast cancer is discouraged due to high false-negative rate [26, 27].
In the clinically negative axilla, some advocate a sentinel node biopsy before initiation of neoadjuvant chemotherapy. This may be done at the time of port placement. Proponents of this approach believe that this would allow for more accurate staging, avoiding the chemotherapy effects that may cause a high false-negative rate [27]. This also might enable appropriate radiation planning. Others believe that staging the axilla after neoadjuvant chemotherapy might prevent additional surgery for SNB and spare some patients an axillary dissection [28]. No randomized control trial has evaluated this question to date.
Mamounas et al. reviewed results of patients that had received neoadjuvant chemotherapy as part of the NSABP B 2-27 trial [29]. Although a sentinel node biopsy was not part of the protocol, it was attempted before the mandated axillary dissection in 428 patients who had received neoadjuvant chemotherapy. The success rate of identification was 84.8 %. This was higher with use of radiocolloid (87.6–88.9 %) compared with blue dye alone (78.1 %, P = 0.03). The false-negative rate of sentinel node biopsy was 10.7 %, and overall accuracy of predicting axillary status was 95.6 %.
The ongoing ACOSOG Z1071 trial is designed to examine the false-negative rate of sentinel node biopsy in patients receiving neoadjuvant chemotherapy (NAC). The trial will study women with T1–4, N1–2, M0 breast cancer who will undergo preoperative NAC followed by SNB and ALND. It will help to delineate the role of SNB and ALND after NAC in women with node-positive breast cancer at initial diagnosis.
Nomograms for prediction of nonsentinel lymph node metastases
Traditionally, patients with metastases to the sentinel lymph node have undergone a completion ALND. Proponents of this approach argue that ALND is essential for optimal locoregional control, which may affect survival [30]. They also argue that ALND provides important prognostic information and may influence the use of adjuvant therapy. Critics of routine completion ALND argue that nonsentinel lymph node metastasis is absent in up to 60 % of patients who have a positive sentinel node, and thus many patients are undergoing unnecessary ALNDs [30, 31]. Degnim et al. undertook a meta-analysis of 11 studies with 1,535 patients to assess the clinicopathological features associated with metastases in nonsentinel lymph nodes [32]. They identified five factors associated with a high likelihood of metastases in nonsentinel lymph nodes. These were sentinel lymph node metastases >2 mm, extranodal extension from a sentinel node, tumor size >2 cm, more than one sentinel node with metastases, and lymphovascular invasion in the primary tumor.
Attempts have been made to develop mathematical models that could predict which patients with positive sentinel nodes may have additional nodes involved and could benefit from ALND. Van Zee et al. at Memorial Sloan Kettering Cancer Center (MSKCC) developed a nomogram to predict the likelihood of metastases to nonsentinel nodes [33]. They included pathologic size, tumor type and nuclear grade, lymphovascular invasion, multifocality, estrogen receptor status, method of detection, number of positive SLN, and number of negative SLN in the nomogram. On multivariate logistic regression analysis, pathologic size, lymphovascular invasion, method of detection, and the number of positive and negative nodes were each associated with increased likelihood of nonsentinel node metastases.
Besides the MSKCC nomogram, numerous others have been developed in recent years [34–36]. Pal et al. developed the Cambridge nomogram, which includes grade, OMS (overall metastatic tumor size, the largest size of sentinel lymph node in millimeters), and proportion of involved sentinel lymph nodes to estimate status of nonsentinel nodes [34]. Similarly the Stanford nomogram considers tumor size, lymphovascular invasion, and the size of the largest SLN [35].
A group of investigators at the MD Anderson Cancer Center developed a separate nomogram for predicting nonsentinel node metastases in patients undergoing neoadjuvant chemotherapy [37]. They reported that lymphovascular invasion, the method to detect sentinel node metastases, multicentricity, positive axillary lymph nodes at presentation, and pathologic tumor size, is predictive.
Ultimately, surgeons should understand that nomograms predict the probability of involvement of a nonsentinel node but provide no guidelines as to which patients should undergo ALND. Many surgeons find that nomograms are useful to counsel patients in regards to management options.
ACOSOG Z011 trial
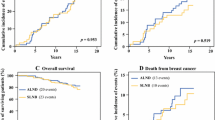
The results of the ACOSOG Z011 trial have generated considerable debate about whether ALND should remain standard practice in sentinel node-positive patients [38]. In this trial, patients with sentinel node metastases were randomized to undergo either an ALND or no further treatment. Patients in this trial were treated with lumpectomy, adjuvant systemic therapy, and tangential field whole breast radiation therapy. There was no difference in locoregional recurrence, disease-free survival, or overall survival rates between the two arms of the trial. The authors therefore argued that ALND could be avoided in selected patients with sentinel-node positive tumors who are treated with lumpectomy, particularly if radiotherapy and systemic therapy will be administered. It should be emphasized that this trial did not include patients treated with mastectomy, patients who received partial breast radiation, or whole breast radiation in the prone position where the axilla is not treated. This trial also did not include patients who received neoadjuvant chemotherapy. For all such patients with metastases to the sentinel node, ALND should remain standard practice.
However, several centers are adopting the practice of eliminating routine axillary dissection in patients who meet the inclusion criteria of the ACOSOG Z0011 trial. Many centers also are limiting the use of intraoperative sentinel node assessment [39].
Yet, several concerns about the ACOSOG Z0011 study have been raised. The study failed to meet its target accrual goal (target accrual was 1,900 patients, but only 891 patients were actually randomized). Thus, the trial may be potentially underpowered. Furthermore, the follow-up period was relatively short (median, 6.8 years), and the study also had a higher proportion of patients with estrogen receptor (ER)-positive tumors (82 %) compared with the general U.S. population (77 %). Patients with ER-positive tumors have a greater risk of recurrence after 7 years of follow-up, whereas those with ER-negative tumors are more likely to recur earlier [40, 41]. Thus, further follow-up of this trial might be required before any definite conclusions can be drawn. Finally, sentinel node-positive patients in this trial had minimal axillary disease, and the therapeutic benefit of sentinel node biopsy alone (where generally one to three nodes were removed) would have been similar to those who underwent axillary dissection, where the majority of node-positive patients had three or fewer positive axillary nodes. It is therefore questionable whether the results of this trial can be extrapolated to patients who present with more advanced disease, with more extensive involvement of the axilla.
Conclusions
The management of the axilla has continued to evolve since Halstead introduced the radical mastectomy for the treatment of primary breast cancer. SNB has spared many women the morbidity of ALND. The use of blue dye or radiocolloid alone or in combination has shown good results in identifying the sentinel node. Improved technology has increased detection of “occult metastases” in the sentinel node, although their significance is not clear. The question of optimal timing of SNB in patients receiving neoadjuvant chemotherapy remains controversial, and more data are needed to better define appropriate management. As a result of the ACOSOG Z0011 trial, several centers in the United States are now avoiding axillary dissection in selected patients with metastasis to the axillary sentinel lymph nodes.
References
Halsted WS (1907) I. The results of radical operations for the cure of carcinoma of the breast. Ann Surg 46(1):1–19
Fisher B, Montague E, Redmond C et al (1977) Comparison of radical mastectomy with alternative treatments for primary breast cancer. A first report of results from a prospective randomized clinical trial. Cancer 39(6 Suppl):2827–2839
Devitt JE (1965) The significance of regional lymph node metastases in breast carcinoma. Can Med Assoc J 93:289–293
Cancer Research Campaign Working Party (1980) Cancer research campaign (King’s/Cambridge) trial for early breast cancer. A detailed update at the tenth year. Lancet 2(8185):55–60
Veronesi U, Paganelli G, Viale G et al (2003) A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer. N Engl J Med 349(6):546–553
David NK, Stewart JA, Thomas BJ et al (2007) Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase III trial. Lancet Oncol 8(10):881–888
Mansel RE, Fallowfield L, Kissin M et al (2006) Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: The ALMANAC Trial. JNCI J Natl Cancer Inst 98(9):599–609
Zavagno G, De Salvo GL, Scalco G et al (2008) A randomized clinical trial on sentinel lymph node biopsy versus axillary lymph node dissection in breast cancer. Ann Surg 247(2):207–213
Del Bianco P, Zavagno G, Burelli P et al (2008) Morbidity comparison of sentinel lymph node biopsy versus conventional axillary lymph node dissection for breast cancer patients: results of the sentinella-GIVOM Italian randomised clinical trial. Eur J Surg Oncol 34(5):508–513
Purushotham AD (2005) Morbidity after sentinel lymph node biopsy in primary breast cancer: results from a randomized controlled trial. J Clin Oncol 23(19):4312–4321
Gill G (2008) Sentinel-lymph-node-based management or routine axillary clearance? one-year outcomes of sentinel node biopsy versus axillary clearance (SNAC): a randomized controlled surgical trial. Ann Surg Oncol 16(2):266–275
McLaughlin SA, Wright MJ, Morris KT et al (2008) Prevalence of lymphedema in women with breast cancer 5 years after sentinel lymph node biopsy or axillary dissection: objective measurements. J Clin Oncol 26(32):5213–5219
Kett K, Varga G, Lukacs L (1970) Direct lymphography of the breast. Lymphology 3(1):2–12
Krag DN, Weaver DL, Alex JC, Fairbank JT (1993) Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol 2(6):335–339 discussion 340
Giuliano AE, Kirgan DM, Guenther JM, Morton DL (1994) Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 220(3):391–398 discussion 398-401
Albertini JJ, Lyman GH, Cox C et al (1996) Lymphatic mapping and sentinel node biopsy in the patient with breast cancer. JAMA 276(22):1818–1822
Cox CE, Haddad F, Bass S et al (1998) Lymphatic mapping in the treatment of breast cancer. Oncology (Williston Park) 12(9):1283–1292 discussion 1293-1284, 1297-1288
Morrow M, Rademaker AW, Bethke KP et al (1999) Learning sentinel node biopsy: results of a prospective randomized trial of two techniques. Surgery 126(4):714–720 discussion 720-722
Ashikaga T, Krag DN, Land SR et al (2010) Morbidity results from the NSABP B-32 trial comparing sentinel lymph node dissection versus axillary dissection. J Surg Oncol 102(2):111–118
Kell MR, Burke JP, Barry M, Morrow M (2010) Outcome of axillary staging in early breast cancer: a meta-analysis. Breast Cancer Res Treat 120(2):441–447
Singletary SE, Allred C, Ashley P et al (2002) Revision of the American Joint Committee on Cancer staging system for breast cancer. J Clin Oncol 20(17):3628–3636
Weaver DL, Ashikaga T, Krag DN et al (2011) Effect of occult metastases on survival in node-negative breast cancer. N Engl J Med 364(5):412–421
Giuliano AE, Hawes D, Ballman KV et al (2011) Association of occult metastases in sentinel lymph nodes and bone marrow with survival among women with early-stage invasive breast cancer. JAMA 306(4):385–393
Duncan PG, Pope WD, Cohen MM, Greer N (1986) Fetal risk of anesthesia and surgery during pregnancy. Anesthesiology 64(6):790–794
Gentilini O, Masullo M, Rotmensz N et al (2005) Breast cancer diagnosed during pregnancy and lactation: biological features and treatment options. Eur J Surg Oncol 31(3):232–236
Stearns V, Ewing CA, Slack R, Penannen MF, Hayes DF, Tsangaris TN (2002) Sentinel lymphadenectomy after neoadjuvant chemotherapy for breast cancer may reliably represent the axilla except for inflammatory breast cancer. Ann Surg Oncol 9(3):235–242
Hidar S, Bibi M, Gharbi O et al (2009) Sentinel lymph node biopsy after neoadjuvant chemotherapy in inflammatory breast cancer. Int J Surg 7(3):272–275
Hunt KK, Yi M, Mittendorf EA et al (2009) Sentinel lymph node surgery after neoadjuvant chemotherapy is accurate and reduces the need for axillary dissection in breast cancer patients. Ann Surg 250(4):558–566
Mamounas EP, Brown A, Anderson S et al (2005) Sentinel node biopsy after neoadjuvant chemotherapy in breast cancer: results from National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J Clin Oncol 23(12):2694–2702
Reynolds C, Mick R, Donohue JH et al (1999) Sentinel lymph node biopsy with metastasis: can axillary dissection be avoided in some patients with breast cancer? J Clin Oncol 17(6):1720–1726
Krag DN (2004) NSABP-32: Phase III, randomized trial comparing axillary resection with sentinal lymph node dissection: a description of the trial. Ann Surg Oncol 11(3 Suppl):208S–210S
Degnim AC, Griffith KA, Sabel MS et al (2003) Clinicopathologic features of metastasis in nonsentinel lymph nodes of breast carcinoma patients. Cancer 98(11):2307–2315
Van Zee KJ, Manasseh DM, Bevilacqua JL et al (2003) A nomogram for predicting the likelihood of additional nodal metastases in breast cancer patients with a positive sentinel node biopsy. Ann Surg Oncol 10(10):1140–1151
Pal A, Provenzano E, Duffy SW, Pinder SE, Purushotham AD (2008) A model for predicting non-sentinel lymph node metastatic disease when the sentinel lymph node is positive. Br J Surg 95(3):302–309
Kohrt HE, Olshen RA, Bermas HR et al (2008) New models and online calculator for predicting non-sentinel lymph node status in sentinel lymph node positive breast cancer patients. BMC Cancer 8:66
Mittendorf EA, Hunt KK, Boughey JC et al (2012) Incorporation of sentinel lymph node metastasis size into a nomogram predicting nonsentinel lymph node involvement in breast cancer patients with a positive sentinel lymph node. Ann Surg 255(1):109–115
Jeruss JS, Newman LA, Ayers GD et al (2008) Factors predicting additional disease in the axilla in patients with positive sentinel lymph nodes after neoadjuvant chemotherapy. Cancer 112(12):2646–2654
Giuliano AE, Hunt KK, Ballman KV et al (2011) Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA 305(6):569–575
Caudle AS, Hunt KK, Kuerer HM et al (2011) Multidisciplinary considerations in the implementation of the findings from the American College of Surgeons Oncology Group (ACOSOG) Z0011 study: a practice-changing trial. Ann Surg Oncol 18(9):2407–2412
Jatoi I, Chen BE, Anderson WF, Rosenberg PS (2007) Breast cancer mortality trends in the United States according to estrogen receptor status and age at diagnosis. J Clin Oncol 25(13):1683–1690
Jatoi I (2011) Axillary vs sentinel lymph node dissection for invasive breast cancer. JAMA 305(22):2288 author reply 2290-2281
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kumar, A., Puri, R., Gadgil, P.V. et al. Sentinel Lymph Node Biopsy in Primary Breast Cancer: Window to Management of the Axilla. World J Surg 36, 1453–1459 (2012). https://doi.org/10.1007/s00268-012-1635-8
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-012-1635-8