
Abstract
Background
In addition to symptom relief, the crucial objective of reduction mammoplasty is to achieve a stable and esthetically pleasing postoperative breast shape. However, the morphological changes in breasts following reduction mammoplasty have not been comprehensively understood. In this study, we applied three-dimensional (3D) scanning technology for long-term follow-up monitoring of breast morphological changes to discern their changing trends. Our goal was to provide a reliable basis for assessing postoperative effects and determining follow-up time points.
Methods
This prospective study included patients undergoing vertical-scar reduction mammoplasty. We utilized a combination of linear measurements and 3D scanning to measure various parameters, including breast volume, breast volume distribution, nipple position, and scar length at various time points: pre-surgery, immediately post-surgery, 3-month postoperative, 6-month postoperative, and 1-year postoperative.
Results
A total of 115 patients were enrolled in this study. Throughout the initial 3 months of postoperative follow-up, there was a gradual reduction in breast volume, which tended to stabilize from 3 to 12 months. The nipple position showed a gradual shift both laterally, inferiorly, and posteriorly. The volume of the lower and lateral part of the breast increased gradually. Notably, at 1 year after surgery, the scar length was approximately 6.3% shorter compared to the immediate postoperative measurement.
Conclusions
Our 3D analysis unveiled comprehensive changes in breast morphology: The overall breast volume shifted laterally and inferiorly, the nipple position moved laterally, inferiorly, and posteriorly, and there was a significant reduction in scar length. Concurrently, breast volume exhibited a gradual decrease and stabilization after 3 months, establishing it as a suitable follow-up point for assessing postoperative results. Additionally, surgical plans can be formulated based on the overall trend of changes in breast volume and distribution, combined with methods such as three-dimensional scanning, to enhance surgical outcomes and patient satisfaction.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to authors www.springer.com/00266.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Breast hypertrophy or macromastia not only leads to physical discomfort among patients but also has a profound impact on their psychological well-being. Consequently, an increasing number of patients are choosing reduction mammoplasty to improve breast shaping and simultaneously alleviate clinical symptoms [1, 2]. In 2020, the American Society of Plastic Surgeons (ASPS) reported a total of 115,895 reduction mammoplasties performed worldwide [3]. Reduction mammoplasty involves various techniques based on different incision and flap choices, including vertical-scar, inverted-T-scar, and the round block technique [4,5,6]. Among them, vertical-scar reduction mammoplasty is currently the most widely used incision method, as it is applicable to the majority of patients with breast hypertrophy. What’s more, the vertical-scar technique results in less scarring than the traditional inverted-T and is favored for its ability to provide good lift and shape with fewer incisions. Presently, the assessment of postoperative breast morphology often depends on subjective perceptions from both doctors and patients [7, 8]. However, postoperative breast morphology undergoes dynamic changes, such as edema and redistribution of breast volume. Hence, accurate measurements of breast diameters, volume, and other parameters are crucial to recognize trends in postoperative breast morphological changes. This precision is pivotal for clinical evaluations of postoperative outcomes and for determining optimal follow-up time points.
Over recent years, the field of breast plastic surgery has increasingly adopted three-dimensional (3D) scanning technology due to its exceptional precision and specificity, particularly in assessing morphological changes in breasts following breast augmentation with implants [9,10,11,12,13,14,15]. 3D scanning technology captures multiple images of the breast from various angles and collects data points based on the distortions in projected patterns caused by the breast’s surface. These data points are then utilized to generate a point cloud, which serves as the foundation for creating a 3D model of the breast. Subsequently, specialized software is applied to measure the breast volume [16,17,18]. In this study, we applied 3D scanning technology in combination with linear measurements to analyze the morphological changes in breasts following vertical-scar breast reduction surgery. Our analysis encompassed various parameters, including breast surface diameters, breast volume, distribution of breast volume, nipple position, and scar length. These parameters are essential for identifying the trends in postoperative breast morphological changes that result from reduction mammoplasty.
Materials and Methods
Patient Enrollment
This study was conducted as a prospective clinical investigation, and each aspect of the experimental design had undergone thorough review and approved by the Institutional Review Board of Plastic Surgery Hospital, Chinese Academy of Medical Sciences, and Peking Union Medical College. The prospective study enrolled patients who underwent vertical-scar reduction mammoplasty at our hospital between January 2016 and December 2022. Prior to their surgeries, the patients were provided with a comprehensive explanation regarding the study’s purpose and the utilization of 3D scan data. All surgical procedures were carried out by the same surgeon.
The inclusion criteria were as follows: (1) underwent vertical-scar reduction mammoplasty; (2) no history of significant systemic illness or prior breast-related surgeries; (3) completion of preoperative 3D scans; and (4) a minimum of 1 year of postoperative follow-up.
The exclusion criteria were as follows: (1) postoperative complications such as hematoma, nipple-areolar complex necrosis, and infections that impact breast shape and (2) failure to complete postoperative follow-up within the specified timeframe. Within this timeframe, we performed 380 vertical-scar reduction mammoplasties, of which 115 cases met the inclusion and exclusion criteria. We gathered preoperative and postoperative demographic data, including age, weight, height, and 3D scanning data. The details of patient enrollment are depicted in Fig. 1.

The details of patient enrollment
Surgical Procedure
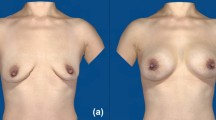
Every patient underwent vertical incision superior pedicle reduction mammoplasty. These surgical procedures were exclusively carried out by the same experienced senior surgeon, who is the corresponding author of this study. During the surgery, drainage tubes were placed, and the patient received dressing change and extubation after operation. Following discharge, the patient was instructed to attend regular follow-up appointments. Postoperatively, it measured the average weight of the excised breast tissue in patients. The preoperative and postoperative outcomes of the patients are shown in Figs. 2, 3, and 4.

Preoperative (a, b) and postoperative photos of patients at 1 year (c, d) of patient A

Preoperative (a, b) and postoperative photos of patients at 1 year (c, d) of patient B

Preoperative (a, b) and postoperative photos of patients at 1 year (c, d) of patient C
Three-dimensional (3D) Scanning Technology
We collect preoperative and postoperative (3 day, post-3D; 3 months, post-3M; 6 months, post-6M; 1 year, and post-1Y) 3D scans of the enrolled patients using a noncontact 3D body scanner (JRCB-D; Jirui, Beijing, China; accuracy B 0.1 mm) (Fig 5). The 3D data were subsequently imported into Geomagic Wrap 2021 software (3-D Systems, South Carolina, USA). We established a 3D coordinate system (X-, Y-, and Z-axes) in accordance with a previously published study [19]. This method was used to establish a coordinate system for each patient, ensuring precise positioning.

3D scan models of preoperative and postoperative follow-up time points: a preoperative 3D scan model; b post-3D, the 3rd day after operation; c post-3M, the 3rd month after operation; d post-6M, the 6th month after operation; and e post-1Y, the 1 year after operation
Breast Volume Measurement
In the Geomagic Wrap software, our methodology involved several steps. First, following established methods, we used the “lasso selection tool” to outline the breast region, then deleted the selected breast region, and used the “Filling Individual Holes” to create a simulated chest wall. Secondly, using the “Trim with Sheet” function within the original image, we selected the breast area alongside the simulated chest wall. We then generated extrusions, intersect extrusion, and implemented reverse selection to create a cylindrical shape with the breast surface. The “Filling Individual Holes” function was used to seal the bottom surface of the cylinder. To ensure proper alignment of the undersurface of the cylinder model with the simulated chest wall, we fine-tuned it using the “Object Mover” tool. The cylinder model with simulated chest wall surface was obtained by “Intersect” of “Boolean”. The breast volume on this side was determined by calculating the volume difference between the cylinder with the breast surface and the cylinder with the simulated chest wall surface, as depicted in Fig. 6 [20].

The process of breast volume measurement: a a selected breast region, b the simulated chest wall was created by deleted the selected breast region, c selected the breast region by using “Trim with Sheet”, d created a cylindrical shape with the breast as the surface, e the cylinder model was fine-tuned to achieve adequate alignment with the simulated chest wall, f obtained the cylinder model with simulated chest wall surface by “Intersect” of “Boolean”, and g the breast volume was obtained by calculating the difference between the two cylinders
Distribution of Breast Volume
We used the “Trim with Plane” function to trim the model of Fig. 6d by adjusting the XZ and YZ plane to the level of the nipple. We then removed either the lower or upper half or the lateral or medial portions of the selection and seamlessly closed the intersecting surfaces, as illustrated in Fig. 7. Subsequently, we calculated the volumes of various sections of the breast model, including the breast volume of the upper polar (BVUP), breast volume of the lower pole (BVIP), breast volume of the lateral pole (BVLP), and breast volume of the medial pole (BVMP). Following these calculations, we determined the ratios of the upper pole to lower pole breast volume (BVUP/BVIP) and the ratios of the lateral pole to medial pole breast volume (BVLP/BVMP).

Used the “Trim with Plane” function to divided the cylindrical models to two parts: a BVUP breast volume of upper polar, BVIP breast volume of inferior polar and b BVIP breast volume of inferior polar, BVLP breast volume of lateral polar, BVMP breast volume of medial polar
Nipple Position
With the measurement function available in the analysis software, we recorded the coordinate position of the nipple in alignment with the established X-, Y- and Z-axis. We then conducted an analysis of the changes in nipple position at different time points (post-3D, post-3M, post-6M, and post-1Y).
Scar Length
Since the length of the scar can be measured directly with a ruler, we adopted both two-dimensional and three-dimensional methods to measure the scar length, making the results more precise. We analyzed the changes in scar length for patients at different times after the operation (post-3D, post-3M, post-6M, and post-1Y).
Statistical Analysis
The data were subjected to analysis using SPSS Statistics for Windows, Version 26.0 (SPSS Inc., Chicago, IL). Measurement data were expressed as mean ± standard deviation (SD). We used a polynomial method to compare the trends of variation at different postoperative time intervals. An paired sample T-test was used to compare changes in breast at different time points after operation. A p-value of less than 0.05 was considered statistically significant.
Results
Study Population
Between January 2016 and December 2022, a total of 115 female patients (230 breasts) underwent reduction mammoplasty were included in this study. The patients’ demographic details are shown in Table 1. The average age of the patients was 35 years old, ranging from 17 to 55. The average BMI of the patients was 23.9 kg/m2, ranging from 18.65 to 37.58 kg/m2. The average weight of the excised breast tissue was 445.5 ± 214.3 g. None of the patients had a history of systematic disease or prior breast-related surgeries. Furthermore, there were no significant differences in the BMI values of patients at each follow-up time point.
Total Breast Volume (BV)
The mean preoperative BV was 816.1 ± 301.3 cm3, which decreased to 461.3 ± 129.9 cm3 after reduction mammoplasty. Over the follow-up period, there was a progressive reduction in breast volume, with the BV at post-3M decreasing by 54.3 cm3 (11.8%) compared to post-3D. Notably, there were no significant changes in breast volume from 3 to 6 months and from 6-month to 1-year post-surgery (Fig. 8). Changes in breast volume at various time points are presented in Table 2.

The breast volume at different follow-up periods
Percentage Volumetric Distribution
The reduction in breast volume was accompanied by a redistribution of breast volume. Specifically, in the upper and lower parts of the breast, the BVUP was gradually decreased, while the BVIP showed a gradual increase, signifying a downward redistribution of breast volume. For the lateral and medial parts of the breast, the BVMP gradually decreased, while the BVLP exhibited a gradual increase, indicating a redistribution of breast volume toward the lateral regions (Figs. 9, 10).

The volume distribution of the upper and lower parts of the breast

The volume distribution of the lateral and medial parts of the breast
Nipple Position
Compared with the preoperative coordinate values, the X-axis and the Y-axis values of the nipple position decreased, and the Z-axis value increased, suggesting medially, superiorly, and anteriorly displacement of the nipple. During the postoperative follow-up period, we observed a gradual increase in the coordinates of the X- and Y- axis, and a decrease in the Z-axis coordinates. This indicates that postoperatively, the position of the nipple gradually shifted laterally, inferiorly and posteriorly. (Table 3, Fig. 11).

Variation trend of nipple position over the follow-up period
Scar Length
The mean scar length, measured at post-3D, post-3M, post-6M, and post-1Y was 12.6 ± 1.5 cm, 12.2 ± 1.7 cm, 11.9 ± 1.2 cm, and 11.8 ± 1.1 cm, respectively (Table 4). Scar length reduced by an average of 6.3% at 1 year compared to immediately after surgery.
Discussion
Reduction mammoplasty, as the current preferred method for solving breast hypertrophy, yields postoperative outcomes and changes in breast morphology that are pivotal in influencing both patient selection and the decisions made by doctors. It is widely recognized that breast morphology undergoes significantly transformations after surgery [21]. Thus, assessing the evolving trends in breast morphology after surgery will contribute to offering valuable clinical guidance.
The introduction of 3D scanning technology has provided a novel approach to breast morphology research, and this technology has been widespread utilization in clinical practice in recent years [9,10,11,12,13]. In this study, we used 3D scanning technology to conduct comprehensively measurements of breast shape, enabling an anlysis of the dynamic changes in breast shape following breast reduction. This analysis encompassed various parameters, including breast volume, breast volume distribution, nipple position, scar length, and more.
Breast volume is a pivotal parameter for assessing the effectiveness of breast reduction surgery. Within the system of breast measurement parameters, volume can be regarded as the outcome of specific measurement indicators. As breast reduction surgery is performed, it is expected that postoperative breast volume will significantly decrease compared to the preoperative state. However, the primary focus should be on observing further changes in postoperative breast volume. Our findings revealed that in the initial 3 months, there was a gradual reduction in breast volume, with an average decrease of 54.3 cm3 (11.8%) by the 3rd-month post-surgery. This is mainly because in the short time after surgery, there will still be edema and other conditions in the breast, resulting in relatively large volume, but as time progresses, this edema gradually subsides, leading to a further reduction in breast volume. From 3 months to 1 year after the surgery, although the breast volume continued to decrease, the overall downward trend was relatively stable, with no significant statistical differences observed. This suggests that postoperative conditions such as edema may have been largely resolved before 3-month post-surgery.
Furthermore, our investigation delved into the distribution of breast volume. The breast volume was divided into upper/lower and lateral/medial parts. The results showed a gradual increase in volume in the lower and lateral parts of the breast over time, particularly within the first 3 months following surgery. This suggests that breast tissue redistributes to the lower and lateral parts. Under the influence of gravity, breast volume gradually accumulates downward, leading to an increased proportion of lower breast volume. Additionally, we observed that the progressive increase in the proportion of lateral breast volume might be attributed to the influence of gravity, as well as other factors like clothing or sleeping positions. Further exploration is required to better understand these factors.
Nipple position is also a significant indicator of breast esthetics, and thus, evaluating its trend is crucial. To assess changes in nipple position, we analyzed coordinate changes post-surgery. The X-, Y-, and Z-axis represent the lateral/medial, superior/inferior, and anterior/posterior movements of the nipple, respectively [22, 23]. Our study found that, compared to preoperative measurements, the coordinates of the nipple on the X- and Y-axis decreased, while the Z-axis coordinates increased, indicating a postoperative shift of the nipple position medially, superiorly, and anteriorly. Patients with breast hypertrophy often experience breast ptosis; thus, the preoperative position of the nipple is generally lateral and inferior, and the nipple is not at the highest point of the breast. During surgery, along with the excision of excess mammary tissue and skin, there is also an elevation of the breast, resulting in a postoperative shift of the nipple position medially, superiorly, and anteriorly. Over time, within our 1-year follow-up period, we observed that the coordinates of the nipple on the X- and Y-axis gradually increased, while the Z-axis coordinates gradually decreased. This indicates a gradual shift of the nipple position laterally, inferiorly, and posteriorly. However, the overall trend in the nipple position changes was relatively stable, with no significant statistical differences. This trend may be related to the redistribution of breast volume. The gradual lateral distribution of breast volume leads to a lateral shift in the nipple position. Although the breast volume gradually distributes downward, over time, the skin above the breast tends to relax, and coupled with the contraction of the scar from the vertical incision below, this results in a lowering of the nipple position, gradually shifting inferiorly and posteriorly [24].
Nonetheless, one of the most important factors impacting the surgical outcomes and a primary concern for patients before surgery is scar length. The extent of scarring is influenced by various factors, including factors such as race, the patient’s constitution, suture technique, and postoperative care [25, 26]. Understanding the overall trend of postoperative scar changes can provide a rational explanation to patients, which is beneficial in alleviating their concerns and can further assist in guiding the selection of incision techniques to enhance surgical outcomes. Our results revealed that scar length gradually decreased over time, with an average reduction of 6.3% compared to the immediate postoperative length after 1 year. This reduction may be attributed to the overall quality of suturing as well as the effective postoperative care provided.
This study presents several limitations, with the most notable being the small sample size. The limited number of participants may affect the generalizability of the findings. In addition, having all procedures carried out by the same surgeon is a kind of limitation. Another limitation pertains to the short follow-up period, which might result from reduced follow-up needs after the surgery due to the improved patient outcomes. Consequently, many patients may have missed follow-up appointments. Additionally, our study exclusively included cases of breast reduction with vertical incisions and superior pedicles. Further validation and investigation are required to understand the postoperative morphological changes associated with other types of incisions or pedicles.
Conclusion
Following reduction mammoplasty, the breast volume gradually decreases and redistributes downward and laterally, while the nipple position gradually moves laterally, inferiorly, and posteriorly. The length of the scar significantly shortened within 1 year post-surgery. The overall morphological changes in the breast tend to stabilize 3-month post-surgery, which can be considered a follow-up time point. Additionally, surgical plans can be formulated based on the overall trend of changes in breast volume and distribution, combined with methods such as three-dimensional scanning, to enhance surgical outcomes and patient satisfaction.
References
Nichols LM, Oranges CM, Tremp M et al (2021) Management of symptomatic breast hypertrophy and reduction mammaplasty. Rev Med Suisse 17(743):1177–1181
Pérez-Panzano E, Gascón-Catalán A, Sousa-Domínguez R et al (2017) Reduction mammaplasty improves levels of anxiety, depression and body image satisfaction in patients with symptomatic macromastia in the short and long term. J Psychosom Obstet Gynaecol 38(4):268–275
American Society of Plastic Surgeons (2020) Plastic surgery statistics report. https://www.plasticsurgery.org/documents/News/Statistics/2020/plastic-surgery-statistics-full-report-2020
Rinker B (2013) Lowering revision rates in medial pedicle breast reduction by the selective addition of “inverted-T” technique. Aesthet Plast Surg 37(2):341–348
Kemaloğlu CA, Özocak H (2018) Comparative outcomes of inferior pedicle and superomedial pedicle technique with wise pattern reduction in gigantomastic patients. Ann Plast Surg 80(3):217–222
Xue AS, Wolfswinkel EM, Weathers WM et al (2013) Breast reduction in adolescents: indication, timing, and a review of the literature. J Pediatr Adolesc Gynecol 26(4):228–233
Wampler AT, Powelson IA, Homa K et al (2021) BREAST-Q outcomes before and after bilateral reduction mammaplasty. Plast Reconstr Surg 147(3):382e–390e
Gfrerer L, Mattos D, Mastroianni M et al (2015) Assessment of patient factors, surgeons, and surgeon teams in immediate implant-based breast reconstruction outcomes. Plast Reconstr Surg 135(2):245e–252e
Yang J, Zhang R, Shen J et al (2015) The three-dimensional techniques in the objective measurement of breast aesthetics. Aesthet Plast Surg 39(6):910–915
Kovacs L, Eder M, Zimmermann A et al (2012) Three-dimensional evaluation of breast augmentation and the influence of anatomic and round implants on operative breast shape changes. Aesthet Plast Surg 36(4):879–887
Ji K, Luan J, Liu C et al (2014) A prospective study of breast dynamic morphological changes after dual-plane augmentation mammaplasty with 3D scanning technique. PLoS ONE 9(3):e93010
Becker H (2012) The role of three-dimensional scanning technique in evaluation of breast asymmetry. Plast Reconstr Surg 130(6):893e–894e
Li XR, Zeng L, Hong WJ et al (2023) Three-dimensional evaluation of results after dual-plane breast augmentation with and without internal suture mastopexy. Aesthet Plast Surg 47(4):1303–1311
Eder M, Klöppel M, Müller D et al (2013) 3-D analysis of breast morphology changes after inverted T-scar and vertical-scar reduction mammaplasty over 12 months. J Plast Reconstr Aesthet Surg 66(6):776–786
Liu Y, Luan J (2023) Breast morphological changes after transaxillary dual-plane augmentation with smooth round implants: a prospective study. Aesthet Plast Surg 47(3):966–978
Tong OLH, Chamson-Reig A, Yip LCM et al (2020) Structured-light surface scanning system to evaluate breast morphology in standing and supine positions. Sci Rep 10(1):14087
Chen L, Sun J, Mu D et al (2020) What makes a difference? three-dimensional morphological study of parameters that determine breast aesthetics. Aesthet Plast Surg 44(2):315–322
Kovacs L, Eder M, Hollweck R et al (2006) New aspects of breast volume measurement using 3-dimensional surface imaging. Ann Plast Surg 57(6):602–610
Liu C, Luan J, Mu L et al (2010) The role of three-dimensional scanning technique in evaluation of breast asymmetry in breast augmentation: a 100-case study. Plast Reconstr Surg 126(6):2125–2132
Lee HY, Hong K, Kim EA (2004) Measurement protocol of women’s nude breasts using a 3D scanning technique. Appl Ergon 35(4):353–359
Swanson E (2012) A measurement system for evaluation of shape changes and proportions after cosmetic breast surgery. Plast Reconstr Surg 129(4):982–992
Eder M, Waldenfels FV, Sichtermann M et al (2011) Three-dimensional evaluation of breast contour and volume changes following subpectoral augmentation mammaplasty over 6 months. J Plast Reconstr Aesthet Surg 64(9):1152–1160
Liu C, Luan J, Ji K et al (2012) Measuring volumetric change after augmentation mammaplasty using a three-dimensional scanning technique: an innovative method. Aesthet Plast Surg 36(5):1134–1139
Ahmad J, Lista F (2008) Vertical scar reduction mammaplasty: the fate of nipple-areola complex position and inferior pole length. Plast Reconstr Surg 121(4):1084–1091
Sun J, Mu D, Liu C et al (2016) Scar assessment after breast augmentation surgery with axillary incision versus inframammary fold incision: long-term follow-up in chinese patients. Aesthet Plast Surg 40(5):699–706
Suga H, Shiraishi T, Takushima A (2020) Scar assessment after breast reconstruction: risk factors for hypertrophy and hyperpigmentation in asian patients. Ann Plast Surg 85(3):229–232
Funding
Not applicable.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
All participants have given informed consent in writing prior to inclusion in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary file 1 (MP4 11266 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Li, H., Lin, Y., Zhang, X. et al. 3D Analysis of Breast Morphological Changes after Vertical-Scar Reduction Mammoplasty: A Prospective Study. Aesth Plast Surg (2024). https://doi.org/10.1007/s00266-024-03985-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00266-024-03985-4