
Abstract
The umbilicus has a paramount aesthetical function for the abdomen and when removed due to a surgical procedure, an umbilicoplasty is mandatory: indeed, its absence could contribute to the development of psychological disorders, especially in childhood. Herein, we describe a straightforward technique to obtain a seemingly natural umbilical scar. This technique, easily taught in a general pediatric surgery environment, may be amenable for any kind of umbilical reconstruction.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The umbilicus represents the only aesthetic scar on the surface of the body on the anterior abdominal wall which is the evolution of umbilical cord detachment that occurs about 2 weeks after birth. In patients in whom the umbilicus is deformed or removed because of a surgical procedure, umbilical reconstruction can be amenable because its absence may contribute to psychological disorders [1], especially in pediatric patients. Umbilical reconstruction has been envisioned for several pathologies such as urachal sinus (Fig. 1) [2], urachal cyst [3], umbilical hernia [4], bladder exstrophy [1], omphalocele undergone surgical correction [5], malignant melanoma [6], and Cantrell’s syndrome [7]. Whenever sacrificed, cosmesis is a priority, hence a procedure which entails a reconstruction of a resemblant umbilicus should be offered [1] either during the same operative time or at a later stage. Although far from ideal, various methods have been devised to reconstruct the umbilicus [5]. When in need of an umbilical surgical reconstruction, it is considered preferable to perform this operation before school age: making sure to devote special attention to both patients’ self-esteem and their parents’ sensibilities, although it should be noted that it is more challenging to recreate a deep umbilicus in toddlers rather than in older children [11]. In this technical report, we describe a straightforward umbilical reconstruction method which would be easily taught in a general pediatric surgery environment.

A case of a two-year-old baby girl who presented to our department with a complicated congenital urachal sinus, resulting in an oozing umbilicus with purulent secretion. This condition lead within time to the development of an umbilical granuloma which was occupying the whole navel area
Operative Technique
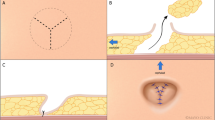
The skin is incised very close to the umbilical edge in order to excise the least skin possible, and suspended 3.0 or 4.0 polydioxanone stitches are applied laterally to pull the umbilical scar (Fig. 2a, b). The access to the abdominal cavity allows complete excision of the umbilical stump (Fig. 2c, d). Abdominal fascia is then sutured by transversal interrupted polyglactin 2.0 stitches (Fig. 2e). To create a neoumbilicus, a crosswise hook 4.0 PDS stitch is applied in the fascia, right where the inner part of the neoumbilicus should reside (Fig. 3b, c). This stitch anchors both the opposite cutaneous edges and the abdominal fascia (Fig. 3d item 2). An intradermic purse string (Fig. 3b–d) is fashioned all around the dermic edge in 4.0 PDS (Figs. 2f, 3d item 1). In sequence, the purse string is pulled and secured and then the perpendicular stitch is tied: this maneuver allows the progressive circular shrinkage of the skin edges which converge toward the fascia thus giving to the newly formed umbilicus a look similar to a physiological umbilical scar (Fig. 2g, h).

The operative technique

Schematic illustration of the operative technique
Discussion
The umbilicus is a cosmetic scar which consists of an ideal front-facing depression, usually located between the median sagittal and the bisiliac line [8]. To preserve the aesthetic look of the umbilicus, surgeons have to consider its anatomical features consisting of a ring, a tubular wall, a groove, and a bottom without any skin excess [9]. The surgical reconstruction of the umbilicus is performed in highly varying situations: from an extreme inadequacy to abundance of available skin or in the presence of scarred tissue.
For example, in giant omphaloceles, it is possible to reconstruct the abdominal wall without the need for prosthetic material, resulting in lower infection rates and reducing the formation of dense adhesions [10]. When the presence of adequate skin allows for reconstruction (i.e., umbilical hernia or urachal sinus), various operative techniques have been proposed. Among these, it is worth mentioning the “tubularized trapezoid flap neoumbilicoplasty”, primarily used in bladder exstrophy [1], umbilical reconstruction using a “reverse fan-shaped flap” [11], a technique with two opposing skin flaps, an upper inverted omega-shaped flap and a lower “Lazy M”-shaped flap [12], another technique using three triangular skin flaps and an excision of a diamond-shaped skin flap [4]. However, these procedures require certain acquaintance with proportions as well as additional incisions. As the level of complexity of the procedure increases, so does the risk of complication and this may have a direct effect on the final aesthetic outcome due to external incisions.
With this technique, we successfully operated on more than ten children reporting no complications (Fig. 4). In our description, the “purse string” technique gives a three-dimensional natural umbilicus without external scarring in which adequate depth is easily and safely obtained and a satisfactory outcome is achieved from an aesthetic standpoint.

The umbilical scar 6 months after the operation
References
Kureel SN, Rashid KA, Rawat J (2009) Tubularized trapezoid flap neoumbilicoplasty–simple technique for umbilical reconstruction in bladder exstrophy. Urology 73(1):70–73
Li Destri G et al (2011) The urachal pathology with umbilical manifestation: overview of laparoscopic technique. J Laparoendosc Adv Surg Tech A 21(9):809–814
Omori M et al (2013) One-stage umbilicus reconstruction after resection of urachal cyst. Ann Plast Surg 71(1):93–95
Takasu H, Watanabe Y (2010) Umbilicoplasty with 3 triangular skin flaps and excised diamond-shaped skin flap. J Pediatr Surg 45(10):2041–2044
Lee Y, Lee SH, Woo KV (2013) Umbilical reconstruction using a modified inverted CV flap with conjoint flaps. J Plast Surg Hand Surg 47(4):334–336
Navysany S et al (2013) Reconstruction of the umbilicus after malignant melanoma. J Dtsch Dermatol Ges 11(5):462–464
Kinoshita M et al (2012) Thoracoabdominoplasty with umbilicoplasty for Cantrell’s syndrome. J Plast Surg Hand Surg 46(5):367–370
Kajikawa A et al (2012) How to reconstruct a natural and deep umbilicus: three methods of umbilicoplasty for five types of umbilical deformities. Ann Plast Surg 68(6):610–615
Gera P, Henry G (2013) Double purse string makes a nice umbilical ring: a novel technique for umbilicoplasty. Eur J Pediatr Surg 23(2):164–166
Van Eijck FC et al (2008) Closure of giant omphaloceles by the abdominal wall component separation technique in infants. J Pediatr Surg 43(1):246–250
Masuda R et al (2003) Reconstruction of the umbilicus using a reverse fan-shaped flap. Aesthetic Plast Surg 27(5):349–353
Tamir G, Kurzbart E (2004) Umbilical reconstruction after repair of large umbilical hernia: the “lazy-M” and omega flaps. J Pediatr Surg 39(2):226–228
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Author information
Authors and Affiliations
Corresponding author
Additional information
Martina Bongini and Sara Tanini have equally contributed to the manuscript.
Rights and permissions
About this article

Cite this article
Bongini, M., Tanini, S., Messineo, A. et al. Umbilical Reconstruction in Children: A Simplified Operative Technique. Aesth Plast Surg 39, 414–417 (2015). https://doi.org/10.1007/s00266-015-0465-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-015-0465-0