
Abstract
Purpose
The study compared the impact of the Kirschner wires versus Herbert screw fixation on the rate of union, time to union, correction of deformity, and clinical outcome in adults with unstable scaphoid waist fracture nonunions without avascular necrosis.
Methods
We prospectively randomized 122 patients to undergo corticocancellous iliac bone grafting and internal fixation either with multiple Kirschner wires or Herbert screw. Radiographs, clinical outcome measures (pain, range of motion, and grip strength), and the Quick DASH score were taken pre- and post-operatively.
Results
The rate of the scaphoid union in the Kirschner wire group was 91% versus 88% in the Herbert group. No difference was detected between the two groups with respect to the time to union, deformity correction, pain analysis, range of motion, grip strength, return to work, and complications.
Conclusion
Using of multiple Kirschner wires as a fixation method for unstable scaphoid waist fracture nonunion that was treated by open reduction and corticocancellous iliac bone grafting had a shorter operative time and lower cost as compared with the Herbert screw fixation. Herbert screw fixation was technically more demanding in terms of technique than K-wires. However, because of easy application of Kirschner wires, and low cost, especially in developing countries, it may be a good alternative to Herbert screw.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The scaphoid is the most commonly fractured carpal bone and account for 60% of all carpal fractures [1, 2]. Approximately about 10% of undisplaced scaphoid fractures fail to unite despite appropriate immobilization [3]. The natural history of the untreated scaphoid waist fracture nonunion often involves apex dorsal angulation with bone loss and collapse (humpback or flexion) deformity [4]. The conventional treatment of scaphoid waist fracture nonunion with humpback deformity typically involves the use of bone graft and internal fixation. The goal of surgery is first adequately to reduce the scaphoid, thereby restoring the carpal height and alignment. Fernandez [5] described a method of fixation using a volar wedge bone graft secured with Kirschner wires; however, Herbert and Fisher [6] described the use of Herbert screw fixation. The purpose of this study is to compare the impact of multiple Kirschner wires versus Herbert screw fixation on the rate of union, time to union, wrist pain, grip strength, range of motion (ROM), correction of deformity, complications, and return to work in adults with unstable scaphoid waist fracture nonunions treated by corticocancellous iliac bone graft.
Materials and methods
The study received the approval of the ethics committee of our university hospital before commencement. Procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 and 2008. The inclusion criteria were patients between the ages of 18 and 60 years with unstable scaphoid waist fractures that had not healed six months after the initial injury, persistent wrist pain, ROM ≤ 70% of the healthy side, and grip strength ≤ 70% of the healthy side. The unstable scaphoid waist fracture nonunion had to have scapholunate angle ≥ 60° [7], lateral intrascaphoid angle ≥ 45° [8], radiolunate angle ≥ 15° [7], and/or with a carpal height index ratio ≤ 0.51 [4]. The exclusion criteria were bilateral scaphoid fractures, history of open fractures, trans-scaphoid perilunate or lunate dislocations, associated fractures in the hand or upper extremities, previous surgical treatment, stage II or higher scaphoid nonunion advanced collapse (SNAC), and scaphoid nonunions with avascular necrosis (AVN). One hundred seventy-three consecutive patients with scaphoid waist fracture nonunion were evaluated to participate in the study between April 2013 and December 2018. Diagnosis of the unstable scaphoid waist fracture nonunions was based on the posteroanterior and lateral radiographs of the wrist, CT scan of the wrist along the longitudinal axis of the scaphoid, and MRI of the wrist to exclude AVN.
Patients who did not meet the entry criteria were 45 patients (nine patients were less than 16 years old, 13 presented less than six months after the initial injury, five had trans-scaphoid perilunate dislocation, 11 had proximal pole nonunion with AVN, five had stage II SNAC, and two had stage III SNAC wrist). Patients who met our inclusion criteria (n = 128) were given an information sheet and informed about the risks and benefits of operative treatment. Further, full written consents were obtained from them. Six patients refused to participate in the study; therefore, 122 patients with unstable scaphoid waist fracture nonunion were randomized to undergo open reduction, corticocancellous iliac bone grafting, and internal fixation with multiple Kirschner wires or Herbert screw. Sixty-one patients were randomized to receive Kirschner wires fixation (K-wire group), and 61 patients were randomized to receive Herbert screw fixation (Herbert group). A random number sheet generated by computer, and the random numbers blocked to ensure equal distribution. Three patients discontinued the intervention and three were lost to follow-up after four weeks. Finally, 116 patients (K-wire group [n = 58] and Herbert group [n = 58]) were analyzed (Fig. 1). Patients’ demographics was listed in Table 1.

Flow chart of the study
The assessment of the clinical parameters (pain, ROM, grip strength) and the interpretations of the disabilities of the arm, shoulder, and hand (Quick DASH) scores [9] were performed pre- and post-operatively. Pain analysis was performed according to the self-reported VAS score [10]. The score was determined by measuring the distance (mm) on the 10-cm line between the “no pain” anchor and the patient’s mark, providing a range of scores from zero to 100. The total and differential arcs of motion of the wrist (extension/flexion, ulnar/radial deviation, and pronation/supination) were measured using a two-arm goniometer [11]. A hand Jamar dynamometer (Sammons Preston, Bolingbrook, Illinois, Chicago) used to evaluate the single maximal effort of grip strength correction for limb dominance [12]. Two orthopaedic surgeons with level-three experience [13] evaluated and interpreted the pre-operative clinical parameters for all the patients. Other two orthopaedic surgeons with level-three experience [13] who were blinded to the pre-operative clinical findings evaluated and interpreted the post-operative clinical parameters. The observers made the measurements independently with no interchange of information, and the average measurements were recorded. Image interpretation, radiographic measurements pre- and post-operative, and the evaluation of the radiographic union were performed by radiologist and orthopaedic surgeon with level-three experience [13]. They were blinded to the clinical findings and surgical results, and the average measurements of the two observers were recorded. The standard posteroanterior and lateral radiographic views evaluated both pre- and post-operative scapholunate angle [7], radiolunate angle [7], and the carpal height index ratio according to Youm et al. [14]. The lateral intrascaphoid angle was [8] measured pre- and post-operatively on the sagittal CT scan of the wrist along the longitudinal axis of the scaphoid.
Surgical technique
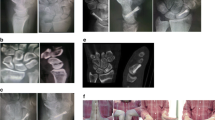
Surgery was performed under general anaesthesia with upper arm tourniquet control. The scaphoid approached through a 4-cm longitudinal volar incision centered over the tuberosity of the scaphoid lateral to the flexor carpi radialis (FCR) tendon. The bed of the FCR was incised in line with the skin incision, and the radioscaphocapitate ligament was incised longitudinally to expose the fracture. The scaphoid was inspected, and the fibrous tissue and sclerotic bone resected up to the normal-looking bone. Generous curettage of each scaphoid pole was essential to expose the healthy bleeding cancellous bone and prepare an adequate cavity to accept the graft (Fig. 2). The scaphoid reduced, and its length restored by introducing a lamina spreader in the gap. A corticocancellous wedge graft was harvested from the ipsilateral iliac crest and packed into the prepared cavity. Satisfactory scaphoid and lunate alignment confirmed by a C-arm image intensifier. In patients randomized for K-wires fixation, the scaphoid was fixed with three 0.045-in. K-wires under image intensify guidance in a retrograde manner with convergent K-wire placement (Fig. 3), and the K-wires cut off beneath the skin. In patients randomized for Herbert screw fixation, the scaphoid was fixed with Herbert bone screw 3 mm (Zimmer, Swindon, Wiltshire, UK) in a retrograde manner. The final screw position was checked and confirmed with the use of an image intensifier. Finally, the capsule and radioscaphocapitate ligament were repaired and the skin was sutured. The procedures were performed either by the senior author (G.H) with level of experience 4 [13] or under his direct supervision.

Generous curettage of each scaphoid pole to prepare an adequate cavity to accept the graft. P proximal pole and D distal pole

Fluoroscopic PA view of the wrist shows the K-wires inserted in a convergent direction
Follow-up
After surgery, each patient’s arm was placed in a dorsal plaster splint that extends above the elbow, and medication for pain control was prescribed. The patients were advised to elevate their arms as much as possible throughout the day to reduce swelling. Active finger motion and shoulder exercises were allowed immediately after surgery several times a day. Further, the skin sutures were removed two weeks after surgery, and a short arm thumb spica cast had to be worn for an additional six weeks and then a short arm removable splint until the radiographic union. In the K-wire group, the wires were removed after radiographic union. Patients commenced hand physiotherapy sessions under the supervision of a specialized hand physiotherapist with gentile hand and wrist exercises followed by aggressive wrist exercises, and heavy activities were allowed after scaphoid union. Gradual return to an office job was allowed within the confines of the cast but manual work was allowed after scaphoid union and within the limits of pain. Full return to work and recreational activities were allowed after union and pain relief. The time of immobilization of both groups, the date of bony union, the time of removal of the K-wires, return to work, and the time needed after the return to work to be able to perform work tasks comfortably documented, and the complications were recorded.
Four radiographic views of the wrist (standard PA, lateral, 45° pronation oblique, and PA with ulnar deviation) were obtained at two week intervals until union. Scaphoid union was defined on the radiographs (in at least three of the four views [15]) as the absence of adverse features such as a gap at graft interface, lucency around or shifting of the screw, or displacement of the graft. Patients underwent CT scans of the wrist along the longitudinal axis of the scaphoid at the follow-up visit when the adverse features disappeared on the radiographs to confirm the union. The time to union was recorded when the CT demonstrated > 50% trabecular bridging across the graft interface. Nonunion was defined when adverse features on the radiographs or < 50% trabecular bridging on CT scan was identified at 24 weeks after surgery.
Statistical analysis
The sample size calculation indicated that 53 patients were required in each group to provide a 95% power of detecting 10% difference with p < 0.05 in separate evaluation of ROM, grip strength, Quick DASH score, and lateral intrascaphoid angle. These four outcomes had a respective standard deviation of 13%, 14%, 20 points, and 14°. The independent t test used to compare the clinical and radiographic measures of both groups pre- and postoperative. The rate of union and complications in each group was compared using the Chi-square test. The paired t test used to compare the pre- and post-operative clinical and radiographic outcome measures for each group. The values are given as mean (range) with confidence interval 95%. p value < 0.05 is considered statistically significant.
Results
No differences were found between the K-wire group and Herbert group with respect to age, sex, hand dominance, side of injury, mechanism of injury, occupation, fracture classification, or time elapsed from initial injury to surgery (Table 1). Both groups were similar in terms of pre-operative clinical and radiographic parameters (VAS, ROM, grip strength, Quick DASH score, scapholunate angle, radiolunate angle, carpal height index, and lateral intrascaphoid angle) (Tables 2 and 3). The mean duration of the surgery for the K-wire group was 46 minutes (40 to 60), and for the Herbert group, it was 67 minutes (55 to 85) (p = 0.001). The mean follow-up period for the K-wire group was 34 months (24 to 57) and for Herbert group was 35 (24 to 39) (p = 0.643). The rate of union in the K-wire group was 91% (n = 53); however, in the Herbert group was 88% (n = 51) (p = 0.544). The two groups were similar regarding the time to union, return to work, and post-operative complications (Table 4). No statistically significant differences were found between the two groups regarding the post-operative clinical and radiographic outcomes. There was significant improvement in the clinical and radiographic outcome measures pre- to post-operative for both groups (Tables 2 and 3). Twelve patients had superficial wound infections that treated with oral antibiotics and wound cleaning. Five patients had mild complex regional pain syndrome treated with physiotherapy, NSAID, and bisphosphonates. Five patients had scar hypertrophy at the wrist wound, and three patients had sensitive scars at the graft site wounds. They were treated by a dermatologist. Nonunion was diagnosed six months post-operatively in five patients of the K-wire group versus six patients of the Herbert group. However, the computed tomography scanning showed no bony bridging across the scaphoid in one more patient of the Herbert group. The nonunions were treated by revision surgeries (open reduction and corticocancellous iliac bone graft with K-wires fixation).
Discussion
Adequate bone graft and stable internal fixation are two important factors for the surgical management of scaphoid nonunion to achieve bony union, restore scaphoid anatomy, improve wrist function, and prevent arthritis. The common sites of bone graft harvesting for scaphoid nonunion are the distal radius and iliac crest. Iliac crest graft permits greater retrieval of marrow and more osteogenic cells [16]. Therefore, iliac crest graft can provide superior osteogenic properties compared with distal radius bone graft. Although several studies [17,18,19,20] reported earlier union rate in some instance of unstable scaphoid nonunion with the use of cancellous iliac bone graft. Our preference was to use corticocancellous graft, as this may be more appropriate in the setting of large intercalary defects causing significant carpal collapse. There are three fixation methods used in the treatment of scaphoid fracture nonunion (Kirschner wires, screw, plate) but there is no study in the current literature directly compares these methods. The Herbert screw was significantly stronger in resisting bending forces as compared to paired parallel Kirschner wires but is unable to withstand cyclical multiaxis loading or rotation [21]. Therefore, our follow-up protocol was to continue immobilization until radiographic union achieved. Despite using the same post-operative immobilization protocol in two different fixation techniques decreases the confounding in determining imobilization time it can adversely affect the ROM and time for return to work in one group. However, our protocol of rehabilitation and return to work can avoid these adverse effects. Moreover, the time taken for return to work is dependent on many factors including the nature of the patient’s occupation and the attitudes of the patient, employer, and insurance company, which makes the time taken to return to work a questionable outcome measure in any event. It has reported that the union time with Kirschner wires is longer and less predictable than Herbert screw. A meta-analysis in 2002 of 36 papers reported that bone graft with screw fixation achieved 94% union, and wedge graft with Kirschner wires achieved 77% union with the average time to union as 20 weeks [3]. In contrast, our study reported no significant difference between the two groups regarding the union rate (91% union with Kirschner wires versus 88% with Herbert screw fixation [0.54]) and the mean time to union was14 weeks. The explanation of this result might relate to the use of three Kirschner wires in a convergent direction to fix the scaphoid. This allows the K-wires to pass through more surface area of the scaphoid and allows for a more targeted placement into the proximal pole, thus increasing the fracture reduction stability and accelerating the union. Meisel et al. [22] used the same fixation technique and reported 100% union rate with cancellous iliac bone grafting in the treatment of scaphoid nonunion. Moreover, our reported result regarding the union rate was consistent with Munk and Larsen [23]; they systematically reviewed 147 publications and found that in the K-wire analysis, there was a higher union rate as compared to the groups fixed with screws. The K-wire group had a higher estimated incidence of union than the screw group (91% versus 88%, respectively), a difference that persisted when used with vascularized grafts (K-wire 94% versus screw 87%). Tables 5 and 6 showed comparison between the present study and other studies in the literature. The thickness of K-wire should be taken into consideration because of the risk of breakage, and we recommend that the K-wire should be removed before mobilizing the joint. The most frequent complications after treatment of fractures with K-wires are pin track infection, pin loosening, or migration. However, migration is not usually toward the joint, it is usually toward the outside, distally from the introduction point. Careful regular follow-up may minimize the incidence of such complications. Based on the proportion of patients who achieved an osseous union and the assessment of the outcomes, the use of multiple K-wires as a fixation method for unstable scaphoid waist nonunion that was treated by open reduction and corticocancellous iliac bone grafting had a shorter operative time and lower cost as compared with the Herbert screw fixation. However, there were no differences in the impact of one method on the time to union, deformity correction, and the clinical outcomes as measured by the Quick DASH score. We thought that the Herbert screw fixation was technically more demanding in terms of technique than K-wires, and the incidence of technical errors may play an eminent role in the occurrence of nonunion. However, because of easy application of Kirschner wires, and low cost, especially in developing countries, it may be a good alternative to Herbert screw. The limitation of the study includes its single -center nature that limits its external validity. Future studies need to compare the using of corticocancellous graft against cancellous only graft in the treatment of unstable scaphoid waist fracture nonunion.
References
Kawamura K, Chung KC (2008) Treatment of scaphoid fractures and nonunions. J Hand Surg Am 33:988–997. https://doi.org/10.1016/j.jhsa.2008.04.026
Leyshon A, Ireland J, Trickey EL (1984) The treatment of delayed union and non-union of the carpal scaphoid by screw fixation. J Bone Joint Surg Br 66:124–127
Merrell GA, Wolfe SW, Slade JF III (2002) Treatment of scaphoid nonunions: quantitative meta-analysis of the literature. J Hand Surg Am 27:685–691. https://doi.org/10.1053/jhsu.2002.34372
Gupta A, Risitano G, Crawford RJ, Burke FD (1999) The ununited scaphoid: prognostic factors in delayed and nonunions of the scaphoid. Hand Surg 4:11–19. https://doi.org/10.1142/S0218810499000101
Fernandez DL (1984) A technique for anterior wedge-shaped grafts for scaphoid nonunions with carpal instability. J Hand Surg Am 9:733–737. https://doi.org/10.1016/S0363-5023(84)80025-8
Herbert TJ, Fisher WE (1984) Management of the fractured scaphoid using a new bone screw. J Bone Joint Surg Br 66:114–123
Linscheid RL, Dobyns JH, Beabout JW, Bryan RS (1972) Traumatic instability of the wrist: diagnosis, classification, and pathomechanics. J Bone Joint Surg Am 54:1612–1632
Amadio PC, Berquist TH, Smith DK, Ilstrup DM, Cooney WP III, Linscheid RL (1989) Scaphoid malunion. J Hand Surg Am 14:679–687. https://doi.org/10.1016/0363-5023(89)90191-3
Hudak PL, Amadio PC, Bombardier C (1996) Development of an upper extremity outcome measure: the DASH (disabilities of the arm, shoulder and hand). The Upper Extremity Collaborative Group (UECG). Am J Ind Med 29:602–608. https://doi.org/10.1002/(SICI)1097-0274(199606)29:6<602::AID-AJIM4>3.0.CO;2-L
Jensen MP, Chen C, Brugger AM (2003) Interpretation of visual analogue scale ratings and change scores: a reanalysis of two clinical trials of post-operative pain. J Pain 4:407–414. https://doi.org/10.1016/S1526-5900(03)00716-8
Carter TI, Pansy B, Wolff AL, Hillstrom HJ, Backus SI, Lenhoff M, Wolfe SW (2009) Accuracy and reliability of three different techniques for manual goniometry for wrist motion: a cadaveric study. J Hand Surg Am 34:1422–1428. https://doi.org/10.1016/j.jhsa.2009.06.002
Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, Sayer AA (2011) A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing 40:423–429. https://doi.org/10.1093/ageing/afr051
Tang JB, Giddins G (2016) Why and how to report surgeons’ levels of expertise. J Hand Surg Eur 41:365–366. https://doi.org/10.1177/1753193416641590
Youm Y, McMurthy RY, Flatt AE, Gillespie TE (1978) Kinematics of the wrist. An experimental study of radial-ulnar deviation and flexion-extension. J Bone Joint Surg Am 60:423–431
Clay NR, Dias JJ, Costigan PS, Gregg PJ, Barton NJ (1991) Need the thumb be immobilised in scaphoid fractures? A randomised prospective trial. J Bone Joint Surg Br 73:828–832
Jarrett P, Kinzel V, Stoffel K (2007) A biomechanical comparison of scaphoid fixation with bone grafting using iliac bone or distal radius bone. J Hand Surg Am 32:1367–1373. https://doi.org/10.1016/j.jhsa.2007.06.009
Park H, Yoon J, Jeon I, Chung H, Kim J (2013) A comparison of the rates of union after cancellous iliac crest bone graft and Kirschner-wire fixation in the treatment of stable and unstable scaphoid nonunion. Bone Joint J 95:809–814. https://doi.org/10.1302/0301-620X.95B6.31259
Kirkham SG, Millar MJ (2012) Cancellous bone graft and Kirschner wire fixation as a treatment for cavitary-type scaphoid nonunions exhibiting DISI. Hand 7:86–93. https://doi.org/10.1007/s11552-011-9375-z
Stark HH, Rickard TA, Zemel NP, Ashworth CR (1988) Treatment of ununited fractures of the scaphoid by iliac bone grafts and Kirschner wire fixation. J Bone Joint Surg Am 70:982–991
Yasuda M, Ando Y, Masada K (2007) Treatment of scaphoid nonunion using volar biconcave cancellous bone grafting. Hand Surg 12:135–140. https://doi.org/10.1142/S0218810407003468
Luria S, Hoch S, Liebergall M, Mosheiff R, Peleg E (2010) Optimal fixation of acute scaphoid fractures: finite element analysis. J Hand Surg 35:1246–1250. https://doi.org/10.1016/j.jhsa.2010.05.011
Meisel E, Seal A, Yao CA, Ghiassi A, Stevanovic M (2017) Management of scaphoid nonunion with iliac crest bone graft and K-wire fixation. Eur J Orthop Surg Traumatol 27:23–31. https://doi.org/10.1007/s00590-016-1876-6
Munk B, Larsen CF (2004) Bone grafting the scaphoid nonunion: a systematic review of 147 publications including 5,246 cases of scaphoid nonunion. Acta Orthop Scand 75:618–629. https://doi.org/10.1080/00016470410001529
Reigstad O, Thorkildsen R, Grimsgaard C, Reigstad A, Rokkum M (2010) Healing of ununited scaphoid fractures by Kirschner wires and autologous structural bone grafts. Scand J Plast Reconstr Surg Hand Surg 44:106–111. https://doi.org/10.3109/02844310903528663
Takami H, Takahashi S, Ando M (2000) Scaphoid nonunion treated by open reduction, anterior inlay bone grafting, and Kirschner-wire fixation. Arch Orthop Trauma Surg 120:134–138. https://doi.org/10.1007/pl00013760
Ritter K, Giachino AA (2000) The treatment of pseudoarthrosis of the scaphoid by bone grafting and three methods of internal fixation. Can J Surg 43:118–124
Chen CY, Chao EK, Lee SS, Ueng SW (1999) Osteosynthesis of carpal scaphoid nonunion with interpositional bone graft and Kirschner wires: a 3- to 6-year follow-up. J Trauma 47:558–563. https://doi.org/10.1097/00005373-199909000-00024
Petcu I (1998) Treatment of scaphoid nonunions by Russe bone grafting-a retrospective analysis. Rev Med Chir Soc Med Nat Iasi 102:105–114
Watanabe K (2011) Analysis of carpal malalignment caused by scaphoid nonunion and evaluation of corrective bone graft on carpal alignment. J. Hand Surg Am 36:10–16. https://doi.org/10.1016/j.jhsa.2010.10.011
Wada T, Aoki M, Usui M, Ishii S (1999) DISI deformity and post-operative symptoms of scaphoid non-union. Hand Surg 4:117–124. https://doi.org/10.1142/s0218810499000393
Inoue G, Shionoya K, Kuwahata Y (1997) Herbert screw fixation for scaphoid nonunions: an analysis of factors influencing outcome. Clin Orthop Relat Res 343:99–106
Trumble TE, Clarke T, Kreder HJ (1996) Nonunion of the scaphoid, treatment with cannulated screws compared with treatment with Herbert screws. J Bone Joint Surg Am 78:1829–1837. https://doi.org/10.2106/00004623-199612000-00005
Nakamura R, Imaeda T, Tsuge S, Watanabe K (1991) Scaphoid non-union with DISI deformity: a survey of clinical cases with special reference to ligamentous injury. J Hand Surg Br 16:156–161. https://doi.org/10.1016/0266-7681(91)90167-m
Adams BD, Blair WF, Reagan DS, Grundberg AB (1988) Technical factors related to Herbert screw fixation. J Hand Surg Am 13:893–899. https://doi.org/10.1016/0363-5023(88)90267-5
Acknowledgments
We wish to acknowledge the help and guidance provided by our Professors, Ahmed Shamma, Ibrahim Mustaffa, Mohamed Bessar, Ali Algushy, and Ismail Yassin, the members of the ethics committee of the Orthopedic department–Faculty of Medicine–Al-Azhar University–Cairo Egypt.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical considerations
Our institutional review board approved this retrospective study before commencement.
Consent
All patients were given an information sheet; the risks and benefits of operative treatment were discussed and full written consent was obtained.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Level of evidence: I
Rights and permissions
About this article

Cite this article
Hegazy, G., Alshal, E., Abdelaal, M. et al. Kirschner wire versus Herbert screw fixation for the treatment of unstable scaphoid waist fracture nonunion using corticocancellous iliac bone graft: randomized clinical trial. International Orthopaedics (SICOT) 44, 2385–2393 (2020). https://doi.org/10.1007/s00264-020-04730-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-020-04730-7