
Abstract
Purpose
The treatment of vertical femoral neck fractures in young patients is a worldwide challenge. The purpose of this study is to introduce a new configuration of cannulated screw fixation in vertical femoral neck fractures by comparing with using ordinary cannulated compression screw (OCCS) alone biomechanically and clinically.
Material and method
Biomechanically, 20 synthetic femur models of femoral neck fractures with 20° of VN angle were divided into two groups. The first group was fixed with three ordinary cannulated compression screws defined as OCCS group; the second group was fixed with two Headless Cannulated Compression Screws (HCCS) plus an OCCS, defined as combination group and tested for axial stiffness and load to failure. Clinically, a prospective study was designed with 59 patients who have vertical femoral neck fractures and were treated with cannulated screw, including 31 patients with three ordinary cannulated compression screws alone and 28 patients with an ordinary cannulated compression screw plus two headless cannulated compression screws.
Results
Biomechanically, our results showed that there was no significant difference of axial stiffness between OCCS group and combination group (109.92 ± 10.81 vs. 123.49 ± 15.13 N/mm, P = 0.145). But, the maximum load to failure of the combination group performed significant advantages than that of the OCCS group (446.85 ± 76.25 vs. 302.92 ± 80.46 N, P = 0.007). Clinically, the rates of fixation failure in the group treated with OCCS alone were 41.9%, while in the group treated with two types of screws were14.3% (P = 0.048).
Conclusion
Our results suggested that using new configuration of an OCCS plus two HCCSs improved the outcome of vertical femoral neck fractures (FNF) patients compared to those using OCCS alone, which provides a new choice for treatment of FNF.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High-energy trauma often causes femoral neck fractures (FNF), of which the preservation of the femoral head is the most important factor to consider in treatment, especially in young patients [1]. Anatomic reduction and stable internal fixation are two significant favorable prognostic factors in FNF [2]. However, in vertical femoral neck fractures, although treatment with internal fixation has been reported satisfactory outcome in many studies [2], the consequences of the complications such as osteonecrosis or nonunion often exert much financial pressure on young patients and their families. Cannulated compression screw (CCS) has been introduced to be an internal fixation device for many years, of which the advantages are obvious [3]. But for certain vertical FNFs, with higher shear angle and bigger shear force, fixation failure rate in patients who treated with fixed angle device was 8%, which performed much better than using CCS alone [1]. Although using the fixed angle devices has shown positive outcomes, the defects like more soft tissue invasion are also difficult to overcome [4].
Then, is there a device which has the advantages of CCS and performs more stability in the treatment for vertical FNF? The headless cannulated compression screw (HCCS) (Acumed Co.) (Fig. 1) has been introduced to be a new type of CCS to treat FNF in recent years. The whole thread design does not only make it obtain better static stability but also restrain the effects of pull strength. On the contrast, the design of ordinary cannulated compression screw (OCCS) (Stryker Co.) (Fig. 1) is half thread with half screw. So theoretically, it provides the OCCS infinite pull strength between the fracture sites by counter against the cortex, but also a finite support. Then, if we make a combination of these two types of screw, we might get both of their benefits. The purpose of this study is to evaluate this new configuration of cannulated screw fixation in vertical femoral neck fractures by comparing with fixation with OCCS biomechanically and clinically.

Application of OCCS and HCCS in femoral neck fractures. a Headless cannulated compression screw. b Ordinary cannulated compression screw
Materials and methods
This is a study in two parts—biomechanical model and clinical study.
Specimen preparation
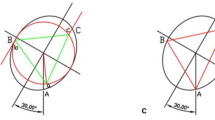
Twenty simulated young men’s synthetic femur models with the same shape (ENOVO, China) were equally divided into two groups. The initial implant placement of each group was pre-drilled before being made into model. The 3D print guiding plates were made to ensure the accurate entrance and the standard position for screws. (Fig. 2).

The 3D print guiding plate for the accurate position of screws and biomechanical testing process. a The 3D print guiding plate. b The position of screws is being triangular by using the guiding plate. c The process of biomechanical testing
Pauwels classification, which is the classic classification, has been used for many years. But, problems like the difficulty to measure the Pauwels angle because of the limb deformity have made it contradictory for a long time [5]. To figure out the relationship between the methods of internal fixation and vertical FNF accurately, VN angle, which is easy to measure and illuminated the relevance between the fracture line and the axis of femoral neck, was applied in this study [6].
A vertical FNF was made with medical pendulum saw at the VN angle of 20°. Further, a 3D print guiding plate was also applied to ensure the fracture line being exactly from the superior of the femoral neck to the above lesser trochanter. After fracture models were established, three parallel guide pins were placed into the initial holes first. Group A (OCCS group): Three parallel OCCSs of 85 mm length and 6.5 mm width were placed. The first one was placed just through beneath of the superior of the femoral neck, the second screw was placed near posterior cortex, and the third one near anterior cortex both beneath the first screw. Group B (combination group): One OCCS and two HCCSs of 85 mm length and 6.5 mm width were placed in the triangle pattern. Firstly, The OCCS was placed just through beneath of the superior of the femoral neck to eliminate the gap between the fragments. Then, the other two HCCSs were placed near the anterior and posterior cortex beneath the OCCS to provide as much stability of medial column as possible. Finally, before the biomechanical testing, the models were fluoroscoped under the C-arm fluoroscopy to make sure the ideal position (Fig. 3).

The models were fluoroscoped under the C-arm fluoroscopy to make sure the ideal position. a OCCS with HCCS. b OCCS
Biomechanical testing
Biomechanical test was done using an Instron test system (Instron, Norwood, MA, USA). To record the displacement of the two sides of the fracture, two magnets were placed on the femoral head and proximal femur. To simulate the femur form in normal walking, the distal femur was fixed with shaft adduction angle of 7°. With a loading rate of 2 mm/minutes, each model was tested the axial compressive load and the maximum load to failure (Fig. 2). The maximum load to failure was defined as a marked decrease after an absolute maximum load [7, 8].
Patients and methods
This study was approved by Ethics Committee. A written informed consent was obtained from the recruited patients. Two hundred nine adult femoral neck fracture patients (ages between 20 and 65, averaged 47.6) who underwent internal fixation were conducted with prospective study from December 2015 to May 2016. Case exclusion criteria were as follows: (1) Other internal fixations were performed, including three locking cannulated compression screws (LCCSs, n = 47), three headless cannulated compression screws (n = 76), and sliding hip screw plus an anti-rotation screw (n = 12); (2) femoral neck fractures together with other lower limb fractures (n = 9); (3) the more horizontal fracture (VN angle < 0°, n = 104); (4) Basicervical fractures (n = 47); (5) factors leading to osteoporosis, such as chronic renal failure, metabolism disorder of parathyroid hormone(n = 9); and (6) the fracture without adequate reduction (n = 26). We defined the criteria of adequate reduction: < 5 mm of displacement and < 10° of angulation in any plane [1].
Finally, 62 patients with vertical femoral neck fractures (VN angle > 0°) were selected in this study, including 33 fractures fixed with OCCS alone, 29 fractures fixed with an OCCS, and two HCCSs. Post-operative treatment was identical in two groups: strict prohibition of weight bearing with affected limb within 3 weeks and toe-touch weight bearing started. After the review at three months, the patients would be given the instruction whether they could do partial weight bearing or totally weight bearing.
Radiographic analysis
Patients were taken standard anteroposterior pelvic and lateral radiographs in operation just after finishing the fracture reduction and were followed up at six weeks, three months, six months, nine months, and 12 months after the surgery, and at any time when they feel uncomfortable with the affected limb (Fig. 4). Compared with initial reduction, fracture displacement (> 5 mm) and femoral neck shortening (> 10 mm), nail withdrawal, and varus deformity (> 10°) were defined as fixation failure [1, 9, 10]. Nonunion was observed and osteonecrosis was identified using the method of Ficat Classification radiographically [11]. All radiographs were analyzed by one of the authors.

Typical radiographs of vertical femoral neck fracture with the combination group and fixation failures in OCCS and combination group. a Just finished the reduction in the operation. b Anteroposterior pelvic radiographs after the fixation in operation. c The anteroposterior pelvic radiographs after the operation in 1 month. d Fixation withdrawal of OCCS. e Fixation withdrawal of the OCCS with HCCS. f Femoral neck shortening of the OCCS with HCCS
Statistical analysis
Statistical comparisons were showed using Statistical Package for Social Sciences (SPSS) 20.0. With the biomechanical study, statistical analysis was carried out using t test and significant difference was considered when P < 0.05 (two-sided). And, the data of clinical study was performed with Fisher’s test.
Results
The results of biomechanical study
The biological results showed that with the VN angle of 20°, the combination group (CG) had a better performance in biomechanical stability than the OCCS group (OG), especially with respect to maximum load to failure (302.92 ± 80.46 vs. 446.85 ± 76.25, P = 0.007) (Table 1, Fig. 5).

The biomechanical results clearly expressed that the method using a OCCS plus two HCCSs performed better biomechanical stability than using three OCCSs alone. a The axial stiffness in the OG is 109.92 ± 10.81 N/mm, and the result in the CG is 123.49 ± 15.13 N/mm, P = 0.145. No statistic significant difference to be found in this comparison. b The maximum load to failure in the two group is 302.92 ± 80.46 and 446.85 ± 76.25 N, respectively, P = 0.007. The difference between the two groups was statistically significant
The results of clinical study
After the verification of biomechanical experiment, we used the configuration clinically and performed the prospective study. Basic characteristics of patients are described in Tables 2 and 3 of the 62 patients lost to follow-up. And, there were 31 performed with OCCS alone and 28 performed with the combined screws. The mean follow-up time was 10.4 ± 4.9 months in OG and 10.7 ± 3.2 months in the CG. Then, the mean VN angle of these fractures is 19.6 ± 10.2° in OG and 21.4 ± 11.6° in CG (Table 2).
Thirty-seven of 59 patients had better outcome after the operation, with no obvious evidence of osteonecrosis, nonunion, or fixation failure. And, among the 22 failed cases, no osteonecrosis occurred. There was only one nonunion occurred in the CG, but the number of the OG was 7 (P = 0.080). As for the situation of fixation failure, the rate is 41.9% (n = 13) and 14.3% (n = 4) of the two groups, respectively (P = 0.048). Of which the rate of nail withdrawal appeared the highest and there were 12 cases totally, ten of which occurred in OG and 2 in the CG (P = 0.039). Nine femoral neck shortening observed in the OG and two in the CG (P = 0.031). Varus deformity also happened with several patients, including seven in the OG and one in the CG (P = 0.033). Fracture displacement was rare, only three in the OG and one in the CG (P = 0.680). The only revision case was happened in the OG (P = 1.000) (Fig. 4).
There is statistical significance with the difference between the two groups of the occurring rate of fixation failure, nail withdrawal, femoral neck shortening, and varus deformity. And, no difference statistical significance was found of the rate of nonunion, fracture displacement, and revision (Table 3).
Discussion
In this study, we introduced a new configuration using CCS to treat for vertical FNF. The biomechanical study was presented first and the results of the maximum load to failure were 446.85 ± 76.25 and 302.92 ± 80.46 N (P = 0.007), respectively. To further estimate the performance of this new configuration, we performed the prospective clinical study and analysis. The results showed that the rates of fixation failure were 14.3% in the CG which had distinct advantages than that in the OG (41.9%).
Compared with horizontal FNF, the treatment of vertical FNF often results in poor outcomes, including osteonecrosis, nonunion, and especially fixation failure [12,13,14]. CCS has been introduced for an internal fixation for many years, whose advantages, including less tissue invasive, less blood loss, shorter hospital stay, and shorter operation time, made it a very common choice for surgeons to treat with FNF [15, 16]. However, the vertical FNFs with a higher “shear angle” are more unstable so that they have a higher rate of fixation failure and nonunion. So, many fixed-angle devices including Dynamic Hip Screw, cephalomedullary nail, and so on were used for the treatment in vertical FNF. Compared to CCS, the fixed angle devices showed advantages including lower osteonecrosis and nonunion rate, and the biomechanical stability was also better [16]. Despite all these advantages, the weakness is also obvious, including more tissue invasive, more blood loss, more complicated operation process, and longer surgery time. Therefore, there is no standard form of surgical stabilization up to now for vertical FNFs.
OCCS is one type of the most common CCS used in the treatment in FNF [17]. Its design of half thread with half screw made it obtain infinite pull strength by countering against the cortex theoretically. But, the method of dynamic compression also increased the rate of fixation failure especially nail withdrawal in vertical FNF; therefore, the rate of femoral neck shortening, varus deformity, and nonunion would increase accordingly. In our biomechanical study, the OG performed limited axial stiffness (109.92 ± 10.81 N/mm) and load to failure (302.92 ± 80.46 N). And, the prospective study also strongly confirmed this viewpoint, the nonunion rate in OG is 22.6% (7 of 31), the rate of nail withdrawal is 32.3% (10 of 31), and there are 9 (29.0%) femoral neck shortening cases happened.
HCCS was introduced as a method to treat with fracture recent years. The headless and full-thread design made it obtain more stable support to counter against the shear force and less muscle irritation. There are a few biomechanical studies that verified that the HCCS had better performance used in the treatment of scaphoid fractures [18]. Similar results were shown with the study of Jonathan H. Capelle et al. [19], and the conclusion was that the HCCS did well in failure displacement. However, the design has deficiencies; full-thread means that the number of thread is certain so that the pull strength cannot change. Whatever the type of the fracture, how much pull strength does the fracture need to maintain stability, after the screw goes in, the pull strength is unchangeable. Therefore, as for the more vertical FNF, using HCCS alone probably cannot achieve the ideal fixation effect.
Due to the limitations of the OCCS and HCCS, using any type of both alone in vertical FNF could not get the ideal fixation result, so we combine them. The basic principle is that one OCCS plus two HCCSs fixed with the configuration of triangle. After the reduction, the OCCS was used first and positioned in the upper vertex of a triangle to provide adequate compression and eliminate the gap between the fragments to stabilize the fracture. Then, the two HCCSs were positioned below the OCCS and played the role in providing the support to the medial cortex to counter against the shear force. The reason why there was no HCCS on the top was because once the osteonecrosis happened, the HCCS tends to cut into the acetabulum. The result of biomechanical test was that the axial stiffness was 123.49 ± 15.13 N/mm and the failure to load was 446.85 ± 76.25 N; both performed better than them in OG. Compared to the biomechanical study, the results in prospective study were more convictive. The rate of fixation failure, and especially the rate of nail withdrawal, femoral neck shortening, and varus deformity. The results clearly expressed the significant advantages using the OCCS plus HCCS. Because of the short follow-up time (less than 2 years), the rate of osteonecrosis did not allow us to make any conclusions.
The weakness of this study includes the bone being synthetic femur models rather than cadaveric femur bone and the small number of patients available for radiographic follow-up; multiple surgeon involvement in the surgery and short follow-up time. However, this study also has innovation, for instance, the 3D printing guide plates were made for assuring the same position, using the VN angle instead of the Pauwels angle and measure the angle after the reduction in operation to guarantee the accurate angle. Therefore, the data in the study is relatively precise.
In conclusion, this study provides us a new thinking of treating vertical FNF using the existing devices. And, the results demonstrate that using one OCCS plus two HCCSs in the treatment of vertical FNF produced better outcome than using OCCS alone. However, further investigation with larger scale of patients is needed in the future.
References
Liporace F, Gaines R, Collinge C, Haidukewych GJ (2008) Results of internal fixation of Pauwels type-3 vertical femoral neck fractures. J Bone Joint Surg Am 90(8):1654–1659
Haidukewych GJ, Rothwell WS, Jacofsky DJ, Torchia ME, Berry DJ (2004) Operative treatment of femoral neck fractures in patients between the ages of fifteen and fifty years. J Bone Joint Surg Am 86:1711–1716
Saglam N, Kucukdurmaz F, Kivilcim H, Kurtulmus T, Sen C, Akpinar F (2014) Biomechanical comparison of antirotator compression hip screw and cannulated screw fixations in the femoral neck fractures. Acta Orthop Traumatol Turc 48:196–201
Lee YS, Chen SH, Tsuang YH, Huang HL, Lo TY, Huang CR (2008) Internal fixation of undisplaced femoral neck fractures in the elderly: a retrospective comparison of fixation methods. J Trauma 64:155–162
van Embden D, Roukema GR, Rhemrev SJ, Genelin F, Meylaerts SA (2011) The Pauwels classification for intracapsular hip fractures: is it reliable? Injury 42:1238–1240
Zhang YL, Zhang W, Zhang CQ (2017) A new angle and its relationship with early fixation failure of femoral neck fractures treated with three cannulated compression screws. Orthop Traumatol Surg Res 103(2):229–234
Nowotarski PJ, Ervin B, Weatherby B, Pettit J, Goulet R, Norris B (2012) Biomechanical analysis of a novel femoral neck locking plate for treatment of vertical shear Pauwel’s type C femoral neck fractures. Injury 43:802–806
Rupprecht M, Grossterlinden L, Ruecker AH, de Oliveira AN, Sellenschloh K, Nuchtern J, Puschel K, Morlock M, Rueger JM, Lehmann W (2011) A comparative biomechanical analysis of fixation devices for unstable femoral neck fractures: the Intertan versus cannulated screws or a dynamic hip screw. J Trauma 71:625–634
Huang TW, Hsu WH, Peng KT, Lee CY (2011) Effect of integrity of the posterior cortex in displaced femoral neck fractures on outcome after surgical fixation in young adults. Injury 42:217–222
Zlowodzki M, Brink O, Switzer J, Wingerter S, Woodall J Jr, Petrisor BA, Kregor PJ, Bruinsma DR, Bhandari M (2008) The effect of shortening and varus collapse of the femoral neck on function after fixation of intracapsular fracture of the hip: a multi-centre cohort study. J Bone Joint Surg Br 90:1487–1494
Ficat RP (1985) Idiopathic bone necrosis of the femoral head. Early diagnosis and treatment. J Bone Joint Surg Br 67:3–9
Collinge CA, Mir H, Reddix R (2014) Fracture morphology of high shear angle “vertical” femoral neck fractures in young adult patients. J Orthop Trauma 28:270–275
Enocson A, Lapidus LJ (2012) The vertical hip fracture—a treatment challenge. A cohort study with an up to 9-year follow-up of 137 consecutive hips treated with sliding hip screw and antirotation screw. BMC Musculoskelet Disord 13:171
Freitas A, Maciel RA, Lima Rde A, Souto DR, Ferrer Mde A (2014) Mechanical analysis of femoral neck fracture fixation with dynamic condylar screw in synthetic bone. Acta Ortop Bras 22:264–268
Selvan VT, Oakley MJ, Rangan A, Al-Lami MK (2004) Optimum configuration of cannulated hip screws for the fixation of intracapsular hip fractures: a biomechanical study. Injury 35:136–141
Warschawski Y, Sharfman ZT, Berger O, Steinberg EL, Amar E, Snir N (2016) Dynamic locking plate vs. simple cannulated screws for nondisplaced intracapsular hip fracture: a comparative study. Injury 47:424–427
Aminian A, Gao F, Fedoriw WW, Zhang LQ, Kalainov DM, Merk BR (2007) Vertically oriented femoral neck fractures: mechanical analysis of four fixation techniques. J Orthop Trauma 21:544–548
Fowler JR, Ilyas AM (2010) Headless compression screw fixation of scaphoid fractures. Hand Clin 26(3):351–361
Capelle JH, Couch CG, Wells KM, Morris RP, Buford WL Jr, Merriman DJ, Panchbhavi VK (2013) Fixation strength of anteriorly inserted headless screws for talar neck fractures. Foot Ankle Int 34(7):1012–1016
Acknowledgments
We thank the staff of Sports Biomechanics Laboratory in Shanghai Jiao Tong University Affiliated Sixth People’s Hospital and colleagues who provided us a lot of useful inspiration.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article and no conflict outside the current study.
Rights and permissions
About this article

Cite this article
Zhang, B., Liu, J., Zhu, Y. et al. A new configuration of cannulated screw fixation in the treatment of vertical femoral neck fractures. International Orthopaedics (SICOT) 42, 1949–1955 (2018). https://doi.org/10.1007/s00264-018-3798-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-3798-x