
Abstract
The purpose was to evaluate the value of radiology to distinguish between symptomatic and asymptomatic flexible flatfeet in young male adults. Among young male army recruits, 56 feet of 28 recruits were diagnosed as otherwise normal, flexible flatfoot with invisible longitudinal arch on stance and either symptomatic or asymptomatic unilaterally or bilaterally. The talus-first metatarsal and calcaneal pitch angles were measured on weight-bearing lateral radiographs, and the results were evaluated statistically. The talus-first metatarsal angle showed statistical significance in both non-parametric and logistic regression tests, but the calcaneal pitch angle showed statistical significance only in non-parametric test between symptomatic and asymptomatic flatfoot groups. Although the single gender and number of samples limit the applicability of our study, these results caused us to make an interpretation that increased talus-first metatarsal angle might be an important risk factor of being symptomatic in otherwise normal flexible flatfoot.
Résumé
Le but de cette étude est d’évaluer la valeur de la radio dans les pieds plats d’adultes jeunes qu’il soit symptomatique ou asymptomatique.Matériel et méthode : parmi des sujets recrutés dans l’armée, 56 pieds sur 28 recrues ont été considérés comme plats avec ou sans symptômes, qu’ils soient uni ou bilatéraux. L’angle astragale premier métatarse et le calcanéum a été mesuré en charge sur des radiographies de profil.Résultats : cet angle a une valeur significative seulement dans le test non paramétrique entre le groupe des pieds plats symptomatiques et des pieds plats asymptomatiques.Conclusion : ces résultats nous permettent de penser que l’aggravation de cet angle est un important facteur de risques d’évolution symptomatique chez les sujets avec pieds plats normaux, asymptomatiques.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
There are no distinct clinical or radiographic criteria to distinguish symptomatic and asymptomatic flexible flatfoot [7, 9, 10]. As a clinical definition that best describes the flattening, low or absent arch of the foot creates the clinical picture [2, 3, 6, 8, 9]. However, not every flatfoot that is clinically apparent causes symptoms or restrictions in adults in their usual lifestyle [1, 4]. As well as the clinical picture itself, the radiographic assessment of the flatfoot does not always correlate with the symptoms if any are present, and, although there are several radiographic measurements to assess flatfoot, not all demonstrate significant differences between normal and flat arches [6, 8, 10].
This study was based on the study of Younger et al. [10] who reported four measurements showing statistically significant difference between normal controls and symptomatic flatfeet on radiographic assessment. These angles were talo-first metatarsal (TFM) angle, calcaneal pitch (CP) angle, and medial cuneiform-fifth metatarsal height on the lateral and talar head uncoverage distance on the anteroposterior weight-bearing foot radiographs. We aimed to check the utility of the first two measurements (TFM and CP angles on the lateral weight-bearing foot radiographs), to ascertain whether they can be used to distinguish between symptomatic and asymptomatic idiopatic flatfoot.
Materials and methods
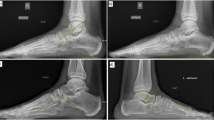
Among the army recruits who were evaluated for flatfoot on the physical examination basis, 9 were diagnosed as having asymptomatic bilateral flatfeet, 13 as symptomatic unilaterally although they had bilateral flatfeet, and 22 as symptomatic bilaterally. Flexible flatfoot on a clinical basis was diagnosed as the recruits’ feet were examined in a weight-bearing and non-weight bearing position to evaluate the medial longitudinal arch, forefoot abduction and heel valgus. The ones with obscured medial longitudinal arch, forefoot abduction and heel valgus in the weight-bearing position were diagnosed as having flatfeet and further evaluated as they stood on tiptoes. The reconstitution of the arch and heel supination on tiptoes were required to make the diagnosis of flexible flatfoot. Among these, those with obscured but still visible arch on weight bearing, lack of hindfoot supination, Achilles tendon contracture, callostasis or other skin problems of the foot (evaluated by the fourth author from the dermatology department), previous foot surgery and neurological or congenital foot disease were evaluated. Since some of the above-mentioned conditions might point out an underlying pathological condition and might cause symptoms not solely related to the flatfoot, the recruits with such findings were excluded from the study group. All the others were assessed with weight-bearing lateral and anteroposterior foot radiographs. Those with arthritic changes and/or accessory navicular were also excluded. As the final study group, 24 feet were grouped as asymptomatic idiopatic flatfoot and 32 were symptomatic idiopatic flatfoot. The total number of both groups members was 28, and all were male with a mean age of 21.67 (range, 19 to 30). The major complaints in the symptomatic group were medial arch pain, foot-ankle and/or calf pain during strenuous activities such as running, long distance walking and military exercises. Physical examination revealed point tenderness on the plantar arch in the symptomatic feet. In both groups lateral weight-bearing foot views were assessed to measure the TFM and CP angles (Fig. 1) to compare both groups statistically.

Schematic illustration of TFM (talo-first metatarsal) and CP (calcaneal pitch) angles on weight-bearing lateral foot radiograph
For statistical evaluation, chi-square test was used to compare the groups, and the power was determined with G-power program. The non-parametric statistical test Mann-Whitney U-test was used to compare the results with respect to TFM and CP angles between the symptomatic and asymptomatic flatfeet. Logistic regression analysis was used to determine the risk factors and the extent these angles influence the probability of symptomatology. Statistical significance was determined as p < 0.05 with a 95% confidence interval.
Results
With the numbers available, statistical evaluation of the results was as follows (Table 1). Of the 56 flatfeet, 32 (57%) were symptomatic and 24 (43%) were asymptomatic; the difference between the groups was not statistically significant (p = 0.28) with chi-square test. When we used G-power program, the power was set at 0.82.
The average values of TFM angles for the 32 symptomatic and 24 asymptomatic flatfeet were 13.00 ± 2.89 (range, 9 to 20) and 8.04 ± 2.56 (range, 3 to 14), respectively. According to the non-parametric evaluation, with the results available the difference between the two groups is statistically significant (p < 0.001). Based on the logistic regression, TFM angle is an important risk factor statistically (p = 0.001), and its change toward the upper degrees increases the risk of being symptomatic 2.41 times (Fig. 2).

Logistic regression for TFM angle showing the increased chance of being symptomatic as the angle increases
The average values of CP angles for the 32 symptomatic and 24 asymptomatic flatfeet were 10.84 ± 2.49 (range, 6 to 15) and 12.45 ± 3.71 (range, 4 to 20), respectively. According to the non-parametric evaluation, the difference between the two groups is statistically significant (p = 0.041). Based on the logistic regression, CP angle is not an important risk factor statistically (p = 0.06), and its change toward the lower degrees increases the risk of being symptomatic only 0.83 times.
Discussion
Radiographic evaluation has long been studied to classify and define the flatfoot and its related clinical features [2, 9, 10]. The correlation between the symptoms and radiographic parameters has not been shown with certainty [7, 10]. However, several studies have claimed that some radiographic parameters have important differences between flatfoot and normal foot [3, 7, 10]. Among these TFM angle, CP angle and medial cuneiform-fifth metatarsal height on weight-bearing lateral radiograph, as well as talar head uncoverage on weight-bearing anteroposterior radiograph have been shown to be the most useful [3, 6, 7, 9, 10].
Adults with flexible flatfoot may demonstrate unilateral as well as more common bilateral symptoms [8]. As defined in the study of Younger et al. [10], symptomatic flatfoot has statistical significance according to the above-mentioned radiographic parameters when compared to a normal foot. In this study, increased TFM angle on standing lateral radiograph was found the most discriminating measurement. It was also mentioned in the study that the purpose was not to identify the radiographic differences between symptomatic and asymptomatic flatfoot in adults. We used this study as the basis for our study where TFM and CP angles on the standing lateral radiographs, the most commonly used ones in our clinical practice, were evaluated between the symptomatic and asymptomatic otherwise normal flexible flat feet. In addition, these young male adults had no visible medial longitudinal arch in stance.
On lateral radiographs of the foot, TFM angle is a determinant of talar inclination and increases in flatfoot as the talar inclination and hindfoot pronation increase; and CP angle shows hindfoot alignment and decreases in flatfoot [7, 8].
In our study with the numbers available, the TFM angle showed statistical significance in both non-parametric and logistic regression tests, but the CP angle showed statistical significance only in the non-parametric test between symptomatic and asymptomatic flatfoot groups. With greater emphasis on the TFM angle, the TFM angle greater than 13.00 ± 2.89 degrees and CP angle less than 10.84 ± 2.49 degrees increased the chance for being clinically symptomatic in flexible otherwise normal flatfoot. Although the single gender and number of samples limit the applicability of our study, these results caused us to make an interpretation that the TFM angle and, to a lesser degree, the CP angle might be used in the evaluation of symptomatic flatfoot. To extrapolate, this data may produce a baseline for the orthotic management of flexible flatfoot [10] as well as for treatment outcomes with either orthotics or surgical interventions.
References
Abdel-Fattah MM, Hassanin MM, Felembane FA, Nassaane MT (2006) Flat foot among Saudi Arabian army recruits: prevalence and risk factors. East Mediterr Health J 12:211–217
Buerk AA, Albert MC (2001) Advances in pediatric foot and ankle treatment. Curr Opin Orthop 12:437–442
Chen CH, Huang MH, Chen TW, Weng MC, Lee CL, Wang GJ (2006) The correlation between selected measurements from footprint and radiograph of flatfoot. Arch Phys Med Rehabil 87:235–240
Esterman A, Pilotto L (2005) Foot shape and its effect on functioning in Royal Australian Air Force recruits. Part 1: Prospective cohort study. Mil Med 170:623–628
Esterman A, Pilotto L (2005) Foot shape and its effect on functioning in Royal Australian Air Force recruits. Part 2: Pilot, randomized, controlled trial of orthotics in recruits with flat feet. Mil Med 170:629–633
Herring JA (2002) Flexible flatfoot (Pes planovalgus). In: Herring JA (ed) Tachdjian’s Pediatric Orthopaedics. WB Saunders, Philadelphia, pp 908–921
Kanatli U, Yetkin H, Cila E (2001) Footprint and radiographic analysis of the feet. J Pediatr Orthop 21:225–228
Lee MS, Vanore JV, Thomas JL, Catanzariti AR, Kogler G, Kravitz SR, Miller SJ, Gassen SC (2005) Diagnosis and treatment of adult flatfoot. J Foot Ankle Surg 44:78–113
Lin CJ, Lai KA, Kuan TS, Chou YL (2001) Correlating factors and clinical significance of flexible flatfoot in preschool children. J Pediatr Orthop 21:378–382
Younger AS, Sawatzky B, Dryden P (2005) Radiographic assessment of adult flatfoot. Foot Ankle Int 26:820–825
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pehlivan, O., Cilli, F., Mahirogullari, M. et al. Radiographic correlation of symptomatic and asymptomatic flexible flatfoot in young male adults. International Orthopaedics (SICOT) 33, 447–450 (2009). https://doi.org/10.1007/s00264-007-0508-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-007-0508-5