
Abstract
Purpose
The imaging features of serous cystadenomas (SCAs) overlap with those of mucinous cystic neoplasms (MCNs) and branch duct intraductal papillary mucinous neoplasms (BD-IPMNs), and an accurate preoperative diagnosis is important for clinical treatment due to their different biological behaviors. The aim of this study was to provide a computed tomographic (CT) feature for the diagnosis of SCAs and estimate whether the “circumvascular sign” can contribute to the discrimination of SCAs from MCNs and BD-IPMNs.
Methods
From August 2011 through December 2019, a total of 71 patients (30 patients with 30 SCAs, 21 patients with 21 MCNs and 20 patients with 22 BP-IPMNs) were enrolled in this study. All patients underwent CT examination and were confirmed by surgical pathology. In addition to patient clinical information, CT features (e.g., location, shape) were evaluated via CT.
Results
Central scarring, central calcification and the circumvascular sign were found to be specific CT features for the diagnosis of SCAs and their differential diagnosis from MCNs and BD-IPMNs. All three CT features had high specificity, and both central scarring and central calcification had low sensitivity. When any one of these two features was combined with the circumvascular sign, the sensitivity increased to 83.3%.
Conclusion
Pancreatic cystic neoplasms that show central scarring, central calcification or the circumvascular sign on CT could be diagnosed as SCAs. When either of the first two features is combined with the circumvascular sign, the diagnostic sensitivity could be increased.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Pancreatic cystic neoplasms (PCNs) are relatively rare and tend to be found incidentally; however, given the widespread use of abdominal cross-sectional imaging techniques, PCNs are becoming diagnosed more frequently [1,2,3,4]. Although PCNs account for only 10 to 15% of pancreatic cystic lesions and 1 to 2% of pancreatic tumors, the management of PCNs depends on their biological behaviors [1, 5, 6]. The three common types of PCNs are serous cystadenomas (SCAs), mucinous cystic neoplasms (MCNs), and intraductal papillary mucinous neoplasms (IPMNs), which constitute more than 90% of PCNs [7]. SCAs account for approximately 20% of PCNs; most are asymptomatic and generally considered benign and do not require surgical resection unless the patient has clinical symptoms or the diagnosis is unclear [8]. MCNs and IPMNs have been described as “mucin-producing cysts” and have malignant potential; they should therefore be treated with surgical resection [3,4,5,6,7]. Thus, it is important to accurately diagnose SCAs from MCNs and IPMNs preoperatively to administer the correct form of treatment.
SCAs mainly occur in older women and classically appear as lobulated, multilocular well-circumscribed masses that contain central stellate scars and calcifications [4, 6,7,8]. The accuracy of preoperative diagnosis is easy when SCAs have these characteristic features. However, central scarring with or without calcifications is seen in only 30% of cases [4, 5, 9, 10]. SCAs can have an oligocystic appearance, although this represents less than 10% of cases, and thus may be mistaken for MCNs [1, 5, 9,10,11]. Meanwhile, MCNs exclusively occur in middle-aged women and usually have internal septa and a multilocular appearance [5, 6]. In addition, branch duct IPMNs (BP-IPMNs) also have a multilocular cystic appearance and can mimic SCAs [12]. Unfortunately, the accuracy of preoperative diagnosis has been reported to be relatively low, ranging from 23.3% [2] to 78% [13], because SCAs can demonstrate a wide spectrum of imaging appearances [8].
Image techniques play an important role in the detection and diagnosis of PCNs. Ultrasonography is not an ideal screening technique due to its relatively low sensitivity [7]. Endoscopic ultrasound is an invasive and operator-dependent technique, with risk of complications such as pancreatitis, and is not well accepted by some patients [12]. Although magnetic resonance imaging (MRI) can demonstrate septa with greater sensitivity than computed tomography (CT), it cannot detect tiny calcifications, and the image quality is easily affected by respiratory motion artifacts [6, 7]. CT remains the first-line imaging modality due to its more widespread availability. In our clinical practice, we found some abnormal arteries around SCAs on CT, which we called the “circumvascular sign”. The aim of this study was to estimate whether the “circumvascular sign” can contribute to the discrimination of SCAs from MCNs and BP-IPMNs.
Materials and methods
Patients
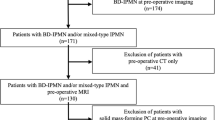
This retrospective study was approved by the Ethics Administration Office of our hospital, and informed patient consent was not required. From August 2011 through December 2019 at our hospital, the terms “serous cystadenomas of pancreas”, “mucinous cystadenomas of pancreas”, “mucinous cystic carcinoma of pancreas”, and “intraductal papillary mucinous neoplasms/tumor of pancreas” were searched from electronic pathology records. Ninety-eight patients were identified within the pathology records. However, 12 patients were excluded because their CT data could not be found on or was incomplete in the picture archiving and communication system (PACS). Fifteen additional patients were excluded because of diagnosis of main duct or combined-type IPMN. Finally, 71 patients (30 SCAs, 21 MCNs and 20 BP-IPMNs) were included. The clinical data for these patients were extracted from the electronic medical records, including age, gender, symptoms and relevant laboratory examination results (e.g., CA199, CEA). The maximal serum reference values for the normal ranges for CA199 and CEA were < 37 U/mL and < 10 ng/mL, respectively.
CT acquisition
Before the operation, all patients received contrast-enhanced abdominal multiple CT examinations using a 16-slice or 64-slice LightSpeed VCT machine (GE Healthcare, Milwaukee, WI, USA) or a dual-source scanner (Flash, Siemens Medical Solutions, Erlangen, Germany). All CT scans were performed using the following parameters: 120 kVp, 200–280 mA s, matrix 512 × 512, pitch 0.8–1.0, section thickness and section distance 5 mm. A total of 80–100 mL of non-ionic contrast medium (Visipaque 320; GE Healthcare) was injected into the antecubital vein at a rate of 3 to 3.5 mL/s. The arterial phase, portal venous phase and delayed phase were obtained 25-30 s, 50-60 s and 120 s, respectively, after contrast medium injection. Subsequently, all images were thinly sliced at a thickness of 0.625 mm and transferred to commercial workstations (GE Healthcare and Siemens Medical Solutions) to generate multiplanar reformations (MPRs), curved planar reformations (CPRs), volume renderings (VRs) and maximum intensity projections (MIPs).
CT image analysis
Two observers blinded to the clinical information and pathological diagnosis analyzed the CT images independently. Dichotomous morphological variables included the location of the PCN (head and neck or body and tail), border (clear or fuzzy), shape (round or ovoid, or lobulated), capsule (thick or shin), central scarring, calcification, main pancreatic duct dilatation, solid component, and “circumvascular sign”. A capsule was considered thick if it was more than 2 mm in diameter and thin if it was 2 mm or less. The presence of calcification was divided into central or other calcification. A 2 mm or greater of the main pancreatic duct was considered dilatation. Solid component was defined as the presence of solid tissues, such as mural nodules, except in the septum and capsule. The “circumvascular sign” was defined as the presence of some abnormal arteries surrounding the lesion on arterial phase CT (Fig. 1). In addition, tumor size, tumor patterns, and degree of enhancement were also recorded. Based on the number of sacs, the tumor patterns were classified as multilocular microcystic, macrocystic (or oligocystic), or mixed [10]. The degree of enhancement was classified into none or mild, moderate, and severe based on the enhancement of the adjacent normal pancreatic parenchyma and psoas major muscle at the three enhancement phases. None or mild enhancement indicated that the enhancement level of the tumor was less than that of the psoas major muscle, moderate enhancement indicated that the enhancement level of the tumor was between that of the psoas major muscle and of the pancreatic parenchyma, and severe enhancement meant that the enhancement level of the tumor was higher than that of the pancreatic parenchyma. Continuous data were calculated as average values, while any discrepancies in categorical data were re-evaluated by a third reader for subsequent statistical analyses.

A 32-year-old female diagnosed with serous cystadenoma. Axial non-contrast-enhanced CT image (a) shows a fluid-density lobulated lesion in the tail of the pancreas, calcifications in the center and septa. Axial contrast-enhanced CT image (b) shows multiple septa dividing the lesion into multiple sacs and the density of enhanced septa between the psoas major muscle and pancreatic parenchyma. Maximum intensity projections image (c) shows some abnormal arteries surrounding the lesion on arterial phase CT
Statistical analysis
Statistical analyses were performed by using SPSS software (version 17.0; SPSS Chicago, IL, USA). Differences in the clinical and CT characteristics between SCAs and both MCNs and BP-IPMNs were compared by using the Chi squared test for categorical variables. The continuous variables were compared using paired sample t tests. The sensitivity and specificity values of the CT characteristics were calculated. A p value ≤ 0.05 was considered to be statistically significant difference.
Results
All patients underwent lesion resection and were diagnosed based on histopathologic examination. Seventy-three lesions were identified in 71 patients, with 2 patients having 2 BP-IPMNs each on both CT and the resection specimens. The clinical information of the 71 patients is listed in Table 1. As shown in Table 1, 30 patients had SCAs (7 males, 23 females), with an average age of 54.6 ± 12.67 (range, 26-75) years, 21 patients had MCNs (4 males, 17 females), with an average age of 52.5 ± 13.27 (range 25–77) years, and 20 patients had BP-IPMNs (16 males, 4 females), with an average age of 61.85 ± 10.05 (range 42–84) years. Three SCAs, 6 MCNs and 8 BP-IPMNs patients presented with abdominal pain, and no others were symptomatic. The remaining lesions were found by chance. Laboratory examination (CA199 and CEA) showed no abnormalities except in 2 patients who were diagnosed with borderline MCNs and presented with elevated CA199 levels of 46 U/mL and 78 U/mL (normal: 0–37 U/mL). However, the CA199 level was not elevated in 5 patients with mucinous cystadenocarcinomas. The statistical analysis showed that patients with MCNs were more likely to have symptoms (p = 0.035) and more males had BP-IPMNs (p < 0.001). There were no significant differences in age or laboratory examination between SCAs and either MCNs or BP-IPMNs.
A comparison of CT features between SCAs and both MCNs and BP-IPMNs is shown in Table 2. In 18 of 30 SCAs, the lesions were located within the body/tail of the pancreas, and the diameter ranged from 1.8 to 9.5 cm. Thirteen MCNs were located in the body/tail of the pancreas versus eight lesions in the pancreatic head, and diameters were ranged from 2.1 to 16.5 cm. Twenty BP-IPMNs were located in the head/neck of the pancreas versus 2 lesions in the pancreatic body, and diameters ranged from 1.7 to 7.1 cm.
All SCAs displayed a lobulated appearance, 25 lesions showed a multilocular microcystic pattern, thin capsules were found in all lesions, central scarring was shown in 11 lesions, central calcification was detected in only 7 lesions, and 3 lesions has septa calcifications. Most MCNs were rounded in shape and macrocystic, a thick capsule was found in 9 lesions, and no central scarring or central calcification was detected. All BP-IPMNs displayed a lobulated appearance, and most demonstrated a multilocular microcystic pattern, a thin capsule, and a lack of central scarring or central calcification.
Solid components were rare and found in 2 SCAs. Most SCAs showed no or mild enhancement, out of all SCAs, 23 lesions had circumvascular signs and 7 lesions were related to the main pancreatic duct dilation. Solid components were shown in 4 MCNs, and all of them were borderline MCNs and mucinous cystadenocarcinomas. Most MCNs showed moderately enhanced, none of the lesions had the circumvascular sign, and 7 lesions resulted in main pancreatic duct dilation. Solid components were found in 5 BP-IPMNs, and 1 of them was malignant. Most BP-IPMNs showed no or mild enhancement, no lesions showed the circumvascular sign, and 19 lesions were associated with main pancreatic duct dilation.
In terms of the morphological characteristics of the SCAs and MCNs, there were statistically significant differences in the shape and patterns of the tumors, central scarring, central calcification, capsule, and circumvascular sign. Regarding the CT features of the SCAs and BP-IPMNs, there were statistically significant differences in the tumor location, central scarring, central calcification, main pancreatic duct dilation and circumvascular sign. Only central scarring, central calcification and the circumvascular sign were consistently statistically significant in the differential diagnosis of SCAs from MCNs and BP-IPMNs.
Table 3 shows the sensitivity and specificity of the central scarring, central calcification and circumvascular sign. The central scarring, central calcification and circumvascular sign had high specificities, 97.7%, 100% and 100%, respectively. However, the sensitivities of central scarring and central calcification were low, 36.7% and 23.3%, respectively. Only the circumvascular sign had moderate sensitivity (76.7%). Combining the circumvascular sign with either of the other features increased the sensitivity for the diagnosis of SCAs to 83.3%.
The relationship between the circumvascular sign and the enhancement degree of the SCAs is listed in Table 4. There were no significant differences revealed by statistical analysis.
Discussion
Pseudocysts represent approximately 90% of all cystic pancreatic lesions [13]; most are related to pancreatitis or trauma and are relatively simple to diagnose. SCAs, MCNs and IPMNs are the most common types of PCNs, but they exhibit distinctly different biological behaviors. SCAs are benign, and most of them do not require surgical resection, while MCNs and BP-IPMNs are recommended for surgical resection due to their malignant potential [1,2,3,4,5,6,7,8,9,10,11,12]. In clinical practice, once a PCN is detected, an accurate and fast diagnosis is important for clinical treatment. SCAs are easily diagnose if the adenomas demonstrate typical imaging features. However, the occurrence of classic CT features is not high [8, 15]. Hence, an accurate preoperative diagnosis remains difficult [14]. In this study, we found that central scarring, central calcification and the circumvascular sign were helpful in distinguishing between the three types of PCNs.
Similar to MCNs, SCAs are diagnosed more frequently in women approximately 50 years of age and are located in the body/tail of the pancreas. The differences between the two are a lobulated appearance, a multilocular microcystic pattern, a thin capsule and central scarring with or without central calcification, which is consistent with previous reports [4, 6,7,8, 10, 14, 15]. However, for BP-IPMNs, these differential diagnostic features may not be applicable except central scarring and central calcification. Central scarring with or without calcification is thought to be a specific feature of SCAs but is only seen in approximately 30% of cases [4, 6, 8, 10]. One report showed that central scarring was seen in less than 20% of SCAs and without calcification [7]. In this study, central scarring was observed in 36.7% of SCAs and 63.6% of these SCAs with central calcification. The difference in the occurrence of central scarring with central calcification may be related to the sample selection. Although the specificity of central scarring and central calcification in the diagnosis of SCAs was high, the sensitivity was low.
The circumvascular sign, which we defined as abnormal arterial vessels surrounding the lesion, had moderate sensitivity and high specificity in the diagnosis of SCAs. We hypothesize that the formation of the circumvascular sign may be related to the blood supply to the tumor. Previous studies have reported that the solid component, central scarring and thin septations show a rich blood supply on arterial phase images [6, 10, 16]. In this study, 2 cases showed solid components, were obviously enhancement and had circumvascular signs. However, 10 lesions with mild enhancement also showed the circumvascular sign. We found that the presence of the circumvascular sign was independent of tumor enhancement degree.
Zhong et al. [5] reported that a head/neck location, lobulated shape, thin wall and septa greater than 2 were significant in diagnosing patients with SCAs. When two of these four findings were combined, the sensitivity and specificity for the diagnosis of SCAs were 80.6% and 84.2%, respectively. Sun et al. [17] indicated that a head/neck location, lobulated shape, thin wall (< 3 mm), and inner regular honeycomb pattern were specific imaging features for the diagnosis of SCAs. When any two features were combined, the sensitivity and specificity were 71.4% and 80.8%, respectively, and when any three features were combined, the specificity reached 100%. However, these studies were solely concerned with the difference between SCAs and MCNs. Features such as a head/neck location, lobulated shape and thin wall cannot be used to identify SCAs from BP-IPMNs. In this study, we found that the circumvascular sign played an important role in the diagnosis of SCAs among the three tumors (SCAs, MCNs and BP-IPMNs). Once central scarring or central calcification was combined with circumvascular sign, the diagnosis sensitivity and specificity for SCAs can be increased to 83.3% and 97.7% or 100%, respectively.
Limitations
There were several limitations of in the current study. First, this is a retrospective study with a small sample size; pseudocysts, solid pseudopapillary tumors and cystic forms of solid tumors were not included in this study. A multicenter study with a large sample size is necessary in the future. Second, all of our lesions were surgically removed and confirmed by pathology. Some cases with typical features were not treated surgically and were excluded from this study, which may have lead to selection bias. Third, many lesions were found by chance, and we did not perform a pancreatic parenchymal phase scan. This may have lead to an increased incidence of the circumvascular sign. Fourth, a disadvantage of CT is that compared with MRI, it has a lower soft tissue resolution and a potentially inferior ability to recognize internal septa, which may have led to a mistake in determining the tumor patterns. Finally, we used three different CT scanners, which may have affected our judgement, although the effect was small.
Conclusions
In conclusion, this study showed that central scarring, central calcification and the circumvascular sign were able to distinguish SCAs from MCNs and BP-IPMNs. When either central scarring or central calcification was combined with the circumvascular sign, the sensitivity for the diagnosis of SCAs increased. The circumvascular sign may be a novel diagnostic and differential diagnostic sign for SCAs.
References
Cohen-Scali F, Vilgrain V, Brancatelli G, Hammel P, Vullierme MP, Sauvanet A, et al. Discrimination of unilocular macrocystic serous cystadenoma from pancreatic pseudocyst and mucinous cystadenoma with CT: initial observations. Radiology. 2003;228(3):727-33.
Yang J, Guo X, Zhang H, Zhang W, Song J, Xu H, et al. Differential diagnosis of pancreatic serous cystadenoma and mucinous cystadenoma: utility of textural features in combination with morphological characteristics. BMC Cancer. 2019;19(1):1223.
Pozzessere C, Castaños Gutiérrez SL, Corona-Villalobos CP, Righi L, Xu C, Lennon AM, et al. Diffusion-Weighted MR imaging in distinguishing between mucin-producing and serous pancreatic cysts. J Comput Assist Tomogr. 2016; 40(4): 505-12.
Elta GH, Enestvedt BK, Sauer BG, Lennon AM. ACG Clinical Guideline: Diagnosis and Management of Pancreatic Cysts. Am J Gastroenterol. 2018;113(4): 464-79.
Zhong L, Chai N, Linghu E, Li H, Yang J, Tang P. A prospective study on endoscopic ultrasound for the differential diagnosis of serous cystic neoplasms and mucinous cystic neoplasms. BMC Gastroenterol. 2019;19(1):127.
Bollen TL, Wessels FJ. Radiological Workup of Cystic Neoplasms of the Pancreas. Visc Med. 2018;34(3):182-90.
Saleem DM, Haseeb WA, Parry AH, Irfan R, Muzaffar NM, Tariq G, et al. Preoperative contrast-enhanced computed tomographic characterisation of pancreatic cystic lesions: A prospective study. SA J Radiol. 2019; 23(1): 1727.
Chu LC, Singhi AD, Hruban RH, Fishman EK. Characterization of pancreatic serous cystadenoma on dual-phase multidetector computed tomography. J Comput Assist Tomogr. 2014;38(2):258-63.
Burk KS, Knipp D, Sahani DV. Cystic Pancreatic Tumors. Magn Reson Imaging Clin N Am. 2018;26(3):405-20.
Chu LC, Singhi AD, Haroun RR, Hruban RH, Fishman EK. The many faces of pancreatic serous cystadenoma: Radiologic and pathologic correlation. Diagn Interv Imaging. 2017;98(3):191-202.
Pravisani R, Intini SG, Girometti R, Avellini C, Leo CA, Bugiantella W, et al. Macrocystic serous cystadenoma of the pancreas: Report of 4 cases. Int J Surg. 2015;21 Suppl 1:S98-S101.
Chen F, Liang JY, Zhao QY, Wang LY, Li J, Deng Z, et al. Differentiation of branch duct intraductal papillary mucinous neoplasms from serous cystadenomas of the pancreas using contrast-enhanced sonography. J Ultrasound Med. 2014;33(3):449 -55.
Lévy P, Rebours V. Differential diagnosis of cystic pancreatic lesions including the usefulness of biomarkers. 2015;31(1):7-13.
Dewhurst CE, Mortele KJ. Cystic tumors of the pancreas: imaging and management. Radiol Clin North Am. 2012;50(3):467-86.
Sun HY, Kim SH, Kim MA, Lee JY, Han JK, Choi BI. CT imaging spectrum of pancreatic serous tumors: Based on new pathologic classification. Eur J Radiol. 2010; 75(2):e45-55.
Liu QY, Zhou J, Zeng YR, Lin XF, Min J. Giant Serous Cystadenoma of the Pancreas (≥10 cm): The Clinical Features and CT Findings. Gastroenterol Res Pract. 2016;2016:8454823.
Sun Y, Zhou F, Liu F, Hu Y, Tan S, Liang P, et al. Discrimination of serous cystadenoma from mucinous cystadenoma in the pancreas with contrast-enhanced ultrasonography: a prospective study in 61 patients. OncoTargets and therapy. 2017;10:1285-94.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have declared that no competing interests exist.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, Gx., Wang, Zp., Chen, Hl. et al. Discrimination of serous cystadenoma from mucinous cystic neoplasm and branch duct intraductal papillary mucinous neoplasm in the pancreas with CT. Abdom Radiol 45, 2772–2778 (2020). https://doi.org/10.1007/s00261-020-02664-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-020-02664-7