
Abstract
Purpose
The washout rate (WR) has been used in 123I-metaiodobenzylguanidine (MIBG) imaging to evaluate cardiac sympathetic innervation. However, WR varies depending on the time between the early and late MIBG scans. Late scans are performed at either 3 or 4 hours after injection of MIBG. The aim of this study was to directly compare the WR at 3 hours (WR3h) with the WR at 4 hours (WR4h).
Methods
We hypothesized that the cardiac count would reduce linearly between the 3-hour and 4-hour scans. A linear regression model for cardiac counts at two time-points was generated. We enrolled a total of 96 patients who underwent planar 123I-MIBG scintigraphy early (15 min) and during the late phase at both 3 and 4 hours. Patients were randomly divided into two groups: a model-creation group (group 1) and a clinical validation group (group 2). Cardiac counts at 15 minutes (countearly), 3 hours (count3h) and 4 hours (count4h) were measured. Cardiac count4h was mathematically estimated using the linear regression model from countearly and count3h.
Results
In group 1, the actual cardiac count4h/countearly was highly significantly correlated with count3h/countearly (r = 0.979). In group 2, the average estimated count4h was 92.8 ± 31.9, and there was no significant difference between this value and the actual count4h (91.9 ± 31.9). Bland-Altman analysis revealed a small bias of −0.9 with 95 % limits of agreement of −6.2 and +4.3. WR4h calculated using the estimated cardiac count4h was comparable to the actual WR4h (24.3 ± 9.6 % vs. 25.1 ± 9.7 %, p = ns). Bland-Altman analysis and the intraclass correlation coefficient showed that there was excellent agreement between the estimated and actual WR4h.
Conclusion
The linear regression model that we used accurately estimated cardiac count4h using countearly and count3h. Moreover, WR4h that was mathematically calculated using the estimated count4h was comparable to the actual WR4h.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
123I-Labelled meta-iodobenzylguanidine (MIBG) cardiac scintigraphy has played an important role in the evaluation of heart failure and neurodegenerative disease [1–5]. The heart-to-mediastinum ratio (HMR) and washout rate (WR) have been used in MIBG imaging to evaluate cardiac sympathetic innervation. The HMR and WR are known to have good reproducibility in planar MIBG imaging [6]. Although quantitative measurement of cardiac MIBG uptake can be performed using HMR and WR, these indices are considerably influenced by collimator performance, processing of the region of interest (ROI) and acquisition conditions [7–10]. In particular, the WR varies depending on the time from the early to the late MIBG scan. Late scanning is alternatively performed at 3 or 4 h after injection of MIBG [11]. Consequently, the WR derived from different acquisition times cannot easily be compared. Therefore determination of the difference between two values is needed to obtain a standardized WR.
We propose a method for estimating cardiac WR at 4 h (WR4h) using early (15 min) and late (3 h) planar images. This method should be useful for the direct comparison of WR at 3 h (WR3h) and WR4h. The aim of this study was to evaluate the efficacy of the method to compare the actual WR4h with an estimated WR4h in a group of consecutive patients who underwent cardiac 123I-MIBG imaging at 15 min, 3 h and 4 h.
Material and methods
Consecutive patients
Consecutive patients (n = 98) who underwent early and late MIBG scans were included in this study. All patients underwent planar imaging at 15 min, 3 h and 4 h after the injection of MIBG. Of the 98 patients, 2 were excluded because of inappropriate time intervals from the 3-h scan to the 4-h scan (27 and 37 min). Since all the patients were retrospectively enrolled, we randomly divided the remaining 96 patients into two study groups: group 1 for creation of a regression model (24 men and 24 women), and group 2 for clinical validation (22 men and 26 women). This study was performed from May 2010 to April 2011 in Okayama Kyokuto Hospital, Okayama, Japan. Informed consent was obtained from all patients before enrolment (in the hospital). The ethics committee approved this study.
Image acquisition
The anterior MIBG planar image was acquired with a dual-head gamma camera (Millennium VG; GE Healthcare Japan, Tokyo, Japan) equipped with an extended low-energy general-purpose collimator. MIBG at a dose of 111 MBq was injected intravenously. An early planar image and two late planar images were acquired at 15 min, 3 h and 4 h after injection. The acquisition time was approximately 3 min in both the early and late scans. Planar imaging was performed with a 256 × 256 matrix. A photopeak window of 123I was centred at 159 keV with a 20 % energy window.
Image analysis
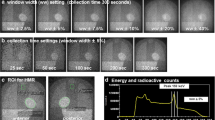
Cardiac count, mediastinal count, HMR and WR were calculated using dedicated software (smartMIBG; FUJIFILM RI Pharma, Tokyo, Japan) [8, 10]. The cardiac count was calculated with a circular ROI set manually at the centre of the heart. Using the size and position of the cardiac ROI, a rectangular mediastinal ROI was automatically determined in the upper mediastinum. Cardiac and mediastinal counts were provided as the mean count per pixel. HMR was expressed as the cardiac count divided by the mediastinal count. WR was expressed as the decrease in cardiac count between the early and late images divided by the cardiac count in the early image, and expressed as a percentage. The cardiac and mediastinal counts in the late image were mathematically corrected for decay using the time between the early and late scans. Using the mediastinal count as the background, WR with background correction was calculated by subtracting the background from the cardiac count, as proposed by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology [12].
Estimation of WR4h
The WR4h was estimated using cardiac and mediastinal counts in the early and 3-h images as follows:
-
1)
In group 1, cardiac and mediastinal counts/pixel were measured. Counts at 3 h (count3h) and 4 h (count4h) were divided by the early counts (countearly). Time-decay correction was used for the compensation of radioactive decay.
-
2)
A linear regression line for the relationship between cardiac count3h and count4h was generated using the following equation:
$$ \begin{array}{l}\frac{coun{t}_{4h}}{coun{t}_{early}}=a\times \frac{coun{t}_{3h}}{coun{t}_{early}}+b\hfill \\ {}\therefore coun{t}_{4h}=a\times coun{t}_{3h}+b\times coun{t}_{early}\hfill \end{array} $$where the variables a and b denote the slope and the y-intercept, respectively. A linear regression line for the mediastinal count was also generated.
-
3)
WR4h was calculated using the following equation:
$$ \begin{array}{l}{\mathrm{WR}}_{4h}=\frac{H_{early}-{H}_{4h}}{H_{early}}\\ {}\kern1.68em =-\left(a\times \frac{H_{3h}}{H_{early}}+b-1\right)\end{array} $$where the variables H early, H 3h and H 4h denote the cardiac countearly, count3h and count4h, respectively. WR4h with background correction was also calculated using the following equation:
$$ \begin{array}{l}{\mathrm{WR}}_{4h}\left( with\; background\; correction\right)=\frac{\left({H}_{early}-{M}_{early}\right)-\left({H}_{4h}-{M}_{4h}\right)}{\left({H}_{early}-{M}_{early}\right)}\\ {}\kern9.12em =-\left(a\times \frac{H_{3h}-{M}_{3h}}{H_{early}-{M}_{early}}+b-1\right)\end{array} $$where the variables M early, M 3h and M 4h denote the mediastinal countearly, count3h and count4h, respectively.
Statistical analysis
All continuous values are expressed as means ± standard deviation. Student’s t test was used to analyse the differences among continuous variables. To analyse the differences between count3h and count4h, a paired t test was used. Linear regression analysis was used to define the relationship between two continuous variables. The chi-squared test was used to compare the differences in categorical variables between groups. A one-way repeated measures analysis of variance was used to compare WRs among no correction, time-decay correction, and time-decay and background corrections. If the overall ANOVA was significant, then pair-wise comparisons were performed using the Bonferroni factor to correct the p values. Intraclass correlation coefficient (ICC) and Bland Altman analysis were used for the assessment of agreement. All statistical tests were two-tailed, and p values <0.05 were considered significant. These analyses were performed using MedCalc version 14.12.0 (MedCalc Software bvba, Ostend, Belgium) and JMP version 11.2.1 (SAS Institute Inc., Cary, NC).
Results
HMR and WR
The time intervals between scans, HMR and WR are shown in Table 1. The mean time interval between the 3-h and 4-h scans was 62 ± 6 min in group 1 and 61 ± 7 min in group 2 (p = ns). Both WR and HMR did not differ between the two groups (p = ns). When the time-decay correction and background correction were used for calculating WR, WR4h was significantly greater than WR3h (p < 0.0001; Fig. 1a). HMR was significantly decreased in accordance with the time after the injection of MIBG (p < 0.01; Fig. 1b).

Late 3-h (black bars) and 4-h WRs (white bars), and HMRs in the early and late scans in the 96 patients. Time-decay correction and time-decay and background corrections were used for calculating WR. The start time of the early and late scans influenced WR and HMR values
Relationship between count3h and count4h
The relationship between count3h and count4h is shown in Fig. 2. Cardiac count4h divided by countearly was positively correlated with cardiac count3h divided by countearly (count4h/countearly = 1.039 × count3h/countearly − 0.067, r = 0.979, p < 0.0001; Fig. 2a). Mediastinal count4h divided by countearly was also positively correlated with mediastinal count3h divided by countearly (count4h/countearly = 0.967 × count3h/countearly − 0.003, r = 0.892, p < 0.0001; Fig. 2b). Bland-Altman analysis revealed that the mean of the difference between count4h/countearly and count3h/countearly was −0.04 for the cardiac region and −0.03 for the mediastinal region (Fig. 2c, d).

Linear regression analysis of the relationship between count3h and count4h, and the agreement between count3h and count4h by Bland-Altman analysis. The Bland-Altman analysis shows no correlation between the mean and difference in the heart region (r = 0.281, p = ns) or the mediastinal region (r = 0.178, p = ns)
Estimated count and actual count
The mean of the actual count4h and estimated count4h was 91.9 ± 31.9 and 92.8 ± 31.9 in the cardiac region, respectively (p = ns), and 47.6 ± 8.4 and 47.4 ± 8.3 in the mediastinal region, respectively (p = ns). In the linear regression there was a positive association between the actual and estimated counts in both the cardiac region (Fig. 3a) and the mediastinal region (Fig. 3b). In the Bland-Altman analysis there was a bias of −0.9 with 95 % limits of agreement of −6.2 to +4.3 in the cardiac region (Fig. 3c), and a bias of 0.1 with 95 % limits of agreement of −2.7 to +3.0 in the mediastinal region (Fig. 3d). The ICC showed excellent agreement between the actual and estimated counts in the cardiac region (ICC(2,1) = 0.996) and in the mediastinal region (ICC(2,1) = 0.985).

Regression and agreement analysis of the relationship between the actual and estimated counts at 4 h in the heart and mediastinal regions. The Bland-Altman analysis shows no correlation between the mean and difference in the heart region (r = 0.000, p = ns) or the mediastinal region (r = 0.062, p = ns)
Estimated WR and actual WR
The average estimated WR4h with time-decay correction was not different from the actual WR4h (24.3 ± 9.6 % vs. 25.1 ± 9.7 %, p = ns). Similarly, the average estimated WR4h with time-decay and background corrections was also not different from the actual WR4h (32.9 ± 22.9 % vs. 34.8 ± 23.0 %, p = ns). The correlation coefficients of the linear regression lines ranged from 0.970 to 0.978 (Fig. 4a, b). The ICC showed excellent agreement between the actual and estimated WRs with time-decay correction (ICC(2,1) = 0.972), and with time-decay and background corrections (ICC(2,1) = 0.967). In the Bland-Altman analysis there was good agreement between the estimated WR4h and the actual WR4h with time-decay correction (bias 0.8, 95 % limits of agreement −3.2 to +4.7), and with both time-decay and background corrections (bias 1.8, 95 % limits of agreement −9.2 to +12.9; Fig. 4c, d).

Regression and agreement analysis of the relationship between the actual WR4h and estimated WR4h. Time-decay correction and both time-decay and background corrections were used in calculating WR. The Bland-Altman analysis shows no correlation between the means and differences in the actual WR4h and estimated WR4hwith time-decay correction (r = 0.074, p = ns) or with time-decay and background corrections (r = 0.030, p = ns)
Discussion
We designed this clinical MIBG study to develop a method for estimating WR4h using early and 3-h planar images. Our results showed that the estimated WR4h was equivalent to the actual WR4h. This approach has the potential to allow direct comparison of WR3h and WR4h, and to standardize quantification of the WR in cardiac MIBG imaging.
Cardiac kinetics of MIBG
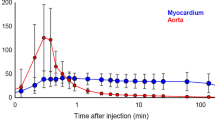
The cardiac kinetics of MIBG after clearance of the initial nonneuronal uptake can be characterized by the equation: A(t) = A 0e−0.693t/T, where A 0 is the cardiac uptake of MIBG in the initial phase, and T is the half-time of the washout [13]. We calculated the cardiac count4h/count3h (count4/3) using this equation as follows: count4/3(T) = A(4)/A(3) = e0.693T. Glowniak et al. found an average T value of 19.0 ± 11.8 in six cardiomyopathy patients and 7.98 ± 4.2 in eight normal controls [14]. The count4/3 for cardiomyopathy patients (T=19.0) and normal controls (T=7.98) were calculated as 0.982 and 0.958, respectively. We suspect that the changes in cardiac kinetics of MIBG at the two late time-points would be limited, even in cardiomyopathy patients and normal controls. Moreover, the slope of the linear regression line between cardiac count3h and count4h was 0.971 in our consecutive 96 patients, showing a similar tendency to the count4/3 values (0.982 and 0.958).
WR with and without time-decay correction and background correction
Regarding the WR calculation using early and late images, we employed time-decay correction and background correction based on the proposed standardization of MIBG for cardiac sympathetic imaging [12]. We sought to determine experimentally the effect of these corrections in our preliminary study (Fig. 5). Decreasing kurtosis associated with background correction was observed in both WR3h and WR4h. Concerning the choice of the corrections for the image analysis, we suggest that time-decay correction would be useful based on histogram distribution.

WR3h (a) and WR4h (b) values with and without time-decay correction and background correction. Histograms were generated from the 96 consecutive patients (group 1 + group 2). WR decreased with time-decay correction, but increased with background correction compared with WR with no correction (p < 0.001). The histogram for WR with time-decay correction shows a narrower distribution (less kurtosis) than the histogram with background correction. The coefficient of variation of WR with time-decay correction was less than that with background correction and that with time-decay and background corrections (WR3h 42 %, 48 % and 73 %, respectively; WR4h 37 %, 40 % and 65 %, respectively)
WR3h and WR4h
WR4h was significantly higher than WR3h in our consecutive patients. Regarding normal WR values with time-decay correction in previous studies, Yoshita et al. found a WR3h of 15.1 ± 7.4 % in 10 normal volunteers [15], Lorberboym et al. found a WR4h of 21 ± 8 % in 7 normal volunteers [16], and Somsen et al. found a WR4h of 23 ± 6.4 % in 25 normal volunteers [17]. The normal WR4h in these studies was also higher than WR3h. Standardization of the time between early and late scans is necessary to compare normal WRs derived under different acquisition conditions. Furthermore, since we hypothesize that WR linearly increases between 3 h and 4 h, WR at any arbitrary time between 3 h and 4 h can be calculated by linear interpolation.
Study limitations
Although both WR3h and WR4h can reasonably be used to evaluate cardiac sympathetic nerve activity, we used only WR4h as a standard index of cardiac WR in this study. Since our method can also be used to estimate WR3h from countearly and count4h, WR3h can also be estimated. The regression line for the estimation of WR4h was determined from the count statistics within the cardiac and mediastinal ROIs. Therefore, patients with severe myocardial sympathetic nerve dysfunction, such as those with dementia with Lewy bodies and severe heart failure, frequently show cardiac MIBG uptake so low that our method may not provide a reliable estimate of WR4h. However, inaccuracy in the determination of WR in patients with very low cardiac uptake is inherent in the calculation of WR, and high WR is usually calculated by the subtraction of background. Since our results are based on a single-centre study, further clinical validation of our method is needed in a multicentre study.
Conclusion
Using the linear regression model for the relationship between count3h and count4h, WR4h estimated from countearly and count3h accurately corresponded with actual WR4h in consecutive patients. This methodology would make it possible to directly evaluate WR3h and WR4h, and to provide WR of intermediate timing between 3 and 4 h. With further clinical validation, the estimation method could be applied to determine a standardized WR value in multicentre studies using 123I-MIBG scintigraphy.
References
Jacobson AF, Senior R, Cerqueira MD, Wong ND, Thomas GS, Lopez VA, et al. Myocardial iodine-123 meta-iodobenzylguanidine imaging and cardiac events in heart failure. Results of the prospective ADMIRE-HF (AdreView Myocardial Imaging for Risk Evaluation in Heart Failure) study. J Am Coll Cardiol. 2010;55:2212–21.
Nakata T, Nakajima K, Yamashina S, Yamada T, Momose M, Kasama S, et al. A pooled analysis of multicenter cohort studies of (123)I-mIBG imaging of sympathetic innervation for assessment of long-term prognosis in heart failure. JACC Cardiovasc Imaging. 2013;6:772–84.
Kashihara K, Ohno M, Kawada S, Okumura Y. Reduced cardiac uptake and enhanced washout of 123I-MIBG in pure autonomic failure occurs conjointly with Parkinson’s disease and dementia with Lewy bodies. J Nucl Med. 2006;47:1099–101.
Yoshita M, Arai H, Arai H, Arai T, Asada T, Fujishiro H, et al. Diagnostic accuracy of 123I-meta-iodobenzylguanidine myocardial scintigraphy in dementia with Lewy bodies: a multicenter study. PLoS ONE. 2015;10:e0120540.
Nakajima K, Okuda K, Matsuo S, Yoshita M, Taki J, Yamada M, et al. Standardization of metaiodobenzylguanidine heart to mediastinum ratio using a calibration phantom: effects of correction on normal databases and a multicentre study. Eur J Nucl Med Mol Imaging. 2012;39:113–9.
Veltman CE, Boogers MJ, Meinardi JE, Al Younis I, Dibbets-Schneider P, Van der Wall EE, et al. Reproducibility of planar (123)I-meta-iodobenzylguanidine (MIBG) myocardial scintigraphy in patients with heart failure. Eur J Nucl Med Mol Imaging. 2012;39:1599–608.
Nakajima K, Okuda K, Yoshimura M, Matsuo S, Wakabayashi H, Imanishi Y, et al. Multicenter cross-calibration of I-123 metaiodobenzylguanidine heart-to-mediastinum ratios to overcome camera-collimator variations. J Nucl Cardiol. 2014;21:970–8.
Hasegawa D, Onishi H, Matsutomo N, Kangai Y. Validation of an optimal analysis method and reproducibility to calculate the heart-to-mediastinum ratio and washout rate in the iodine-123-labeled metaiodobenzylguanidine myocardial scintigraphy. Nihon Hoshasen Gijutsu Gakkai Zasshi. 2014;70:1420–8.
Verschure DO, de Wit TC, Bongers V, Hagen PJ, Sonneck-Koenne C, D’Aron J, et al. (123)I-MIBG heart-to-mediastinum ratio is influenced by high-energy photon penetration of collimator septa from liver and lung activity. Nucl Med Commun. 2015;36:279–85.
Okuda K, Nakajima K, Hosoya T, Ishikawa T, Konishi T, Matsubara K, et al. Semi-automated algorithm for calculating heart-to-mediastinum ratio in cardiac iodine-123 MIBG imaging. J Nucl Cardiol. 2011;18:82–9.
van der Veen L, Scholte A, Stokkel M. Mathematical methods to determine quantitative parameters of myocardial 123I-MIBG studies: a review of the literature. Nucl Med Commun. 2010;31:617–28.
Flotats A, Carrio I, Agostini D, Le Guludec D, Marcassa C, Schafers M, et al. Proposal for standardization of 123I-metaiodobenzylguanidine (MIBG) cardiac sympathetic imaging by the EANM Cardiovascular Committee and the European Council of Nuclear Cardiology. Eur J Nucl Med Mol Imaging. 2010;37:1802–12.
Glowniak JV. Cardiac studies with metaiodobenzylguanidine: a critique of methods and interpretation of results. J Nucl Med. 1995;36:2133–7.
Glowniak JV, Turner FE, Gray LL, Palac RT, Lagunas-Solar MC, Woodward WR. Iodine-123 metaiodobenzylguanidine imaging of the heart in idiopathic congestive cardiomyopathy and cardiac transplants. J Nucl Med. 1989;30:1182–91.
Yoshita M, Taki J, Yokoyama K, Noguchi-Shinohara M, Matsumoto Y, Nakajima K, et al. Value of 123I-MIBG radioactivity in the differential diagnosis of DLB from AD. Neurology. 2006;66:1850–4.
Lorberboym M, Lampl Y, Nikolov G, Sadeh M, Gilad R. I-123 MIBG cardiac scintigraphy and autonomic test evaluation in multiple sclerosis patients. J Neurol. 2008;255:211–6.
Somsen GA, Verberne HJ, Fleury E, Righetti A. Normal values and within-subject variability of cardiac I-123 MIBG scintigraphy in healthy individuals: implications for clinical studies. J Nucl Cardiol. 2004;11:126–33.
Acknowledgments
We thank all patients who participated in the study for their contribution. We also thank the physicians and technologists who participated in this study.
Compliance with ethical standards
ᅟ
Funding
This study was funded by JSPS KAKENHI (26861022) and Grants for Promoted Research from Kanazawa Medical University (S2013-16, S2014-13).
Conflicts of interest
K.N. does collaborative research work for the development of the software with FUJIFIL RI Pharma, Co. Ltd, Japan. Y.K. is employed by FUJIFIL RI Pharma, Co. Ltd, Japan, supplier of 123I-MIBG in Japan.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(GIF 103 kb)
Rights and permissions
About this article

Cite this article
Okuda, K., Nakajima, K., Sugino, S. et al. Development and validation of a direct-comparison method for cardiac 123I-metaiodobenzylguanidine washout rates derived from late 3-hour and 4-hour imaging. Eur J Nucl Med Mol Imaging 43, 319–325 (2016). https://doi.org/10.1007/s00259-015-3173-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-015-3173-8