
Abstract
Background
Rotational acetabular osteotomy (RAO) is one of the surgical treatments for acetabular dysplasia, and satisfactory results have been reported. We evaluated the postoperative changes of articular cartilage and whether the pre-operative condition of the articular cartilage influences the clinical results using T2 mapping MRI.
Methods
We reviewed 31 hips with early stage osteoarthritis in 31 patients (mean age, 39.6 years), including three men and 28 women who underwent RAO for hip dysplasia. Clinical evaluations including Japanese Orthopedic Association (JOA) score and Japanese Orthopedic Association Hip Disease Evaluation Questionnaire (JHEQ), and radiographical evaluations on X-ray were performed. Longitudinal qualitative assessment of articular cartilage was also performed using 3.0-T MRI with T2 mapping technique preoperatively, 6 months, and at 1 and 2 years postoperatively.
Results
There was no case with progression of osteoarthritis. The mean JOA score improved from 70.1 to 93.4 points, the mean postoperative JHEQ score was 68.8 points, and radiographical data also improved postoperatively. We found that the T2 values of the cartilage at both femoral head and acetabulum increased at 6 months on coronal and sagittal views. However, they significantly decreased 1 and 2 years postoperatively. The T2 values of the center to anterolateral region of acetabulum negatively correlated with postoperative JHEQ score, particularly in pain score.
Conclusions
This study suggests that biomechanical and anatomical changes could apparently cause decreased T2 values 1–2 years postoperatively compared with those preoperatively. Furthermore, preoperative T2 values of the acetabulum can be prognostic factors for the clinical results of RAO.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Developmental dysplasia of the hip (DDH) is a major cause of hip osteoarthritis (OA) [1]. Abnormal morphology results in a smaller area of acetabular coverage. Decreased contact area increases the mechanical stress, resulting in cartilage damage [2]. Rotational acetabular osteotomy (RAO), developed by Tagawa and Ninomiya [3], is one of the surgical treatments for symptomatic DDH. This procedure reorients the acetabulum to reduce superolateral acetabular inclination, transferring the joint center medially. This improves femoral head coverage, and normalizes the loading of the acetabular rim [3]. RAO has been reported to have satisfactory intermediate and long-term results in relieving hip pain [4, 5]. However, there have been no reports about qualitative evaluations of pre- and post-operative cartilage condition, and detailing how the preoperative condition of articular cartilage affects clinical results of RAO.
Several magnetic resonance imaging (MRI) techniques such as T2 mapping, T1ρ, and delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) can detect the qualitative changes of articular cartilage, and may therefore serve as biomarkers to define the natural history of cartilage repair [6,7,8]. MRI T2 mapping is a technique sensitive to early biochemical changes in articular cartilage, including water content and collagen fiber orientation due to the interaction between water molecules and between water and surrounding macromolecules [9, 10]. It has become commercially available on clinical scanners and is becoming a standard technique in clinical research primarily evaluating articular cartilage. Previous studies in vitro and in vivo have shown that cartilage T2 values are significantly elevated in subjects with OA, and that it correlates with the severity of OA [11,12,13,14]. Several reports support the use of cartilage T2 as an early marker of cartilage degeneration, demonstrating responsiveness to cartilage change over time [13,14,15]. Thus, the integration of T2 mapping may be useful to gain further knowledge on the treatment of osteotomy, such as RAO. The purpose of our study was to evaluate the longitudinal T2 measurements of cartilage after RAO and how the preoperative condition of the articular cartilage influences the postoperative results by using T2 mapping MRI.
Materials and methods
Ethics approval was granted by the Institutional Review Board, and informed consent was obtained from all individual participants included in the study.
Study population
From December 2011 to March 2013, RAO was performed for DDH in 31 patients (31 hips), including three men and 28 women without femoral osteotomy. The patients have activity-related hip pain and radiographical evidence of acetabular dysplasia [4, 5]. The mean age at surgery was 39.6 years (range, 22–51 years old), and the stage of OA was early stage OA (according to the criteria of the Japanese Orthopedic Association, JOA) in all patients (Table 1). All patients had supine AP view of the pelvis and false-profile radiographs of the affected joint obtained preoperatively. Clinical evaluations, including JOA score (pain 40, ROM 20, walk 20, activities of daily living 20, wherein 0 and 100 points indicate the worst and best, respectively) and the Japanese Orthopedic Association Hip Disease Evaluation Questionnaire (JHEQ) score (0 and 84 points indicate the worst and best, respectively; pain, 0–28 points; movement, 0–28 points; mental, 0–28 points) were evaluated preoperatively and 2 years postoperatively [16]. Radiographical evaluations, including lateral center-edge angle, acetabular roof angle, and minimal joint space width on X-ray were also performed preoperatively and 2 years postoperatively [17, 18]. Longitudinal qualitative assessment of the articular cartilage was performed using T2 mapping MRI.
Surgical procedure
RAO was performed based on the technique of Ninomiya and Tagawa, apart from fixation of the rotated acetabulum with two PLLA screws (Super-FIXSORB; Depuy, Warsaw, IN, USA) instead of Kirschner wires [3]. No postoperative cast was used, and partial weight bearing on two crutches was allowed in the third postoperative week, and full weight bearing was allowed approximately 5 months postoperatively, when the Trendelenburg sign had disappeared.
MRI protocol
To evaluate the longitudinal outcome, MRI was performed preoperatively, at 6 months, and 1 and 2 years postoperatively using a 3.0-T GE Excite Sigma MR Scanner (General Electric, Milwaukee, WI, USA) and phased array coil (USA Instruments, Cleveland, OH, USA). During MRI, the lower extremities were fixed in position (hip extension, neutral rotation). We created an oblique coronal and sagittal plane, which was parallel to the femoral neck, passing through the center of the femoral head, perpendicular to the articular cartilage of the femoral head. This allowed us to obtain an anatomically similar imaging plane each time and to use a relatively small field of view (FOV) (180 × 180 mm) without the need to create of phase wrap artifacts. A frequency-selective fat-suppression technique was used to minimize the chemical shift artifact at the cartilage–bone interface. T2 mappings were obtained from two-dimensional multiple spin-echo images with the following scanning parameters using eight echoes (TR: 1500 ms, TE: 8.4/16.9/25.3/33.8/42.2/50.6/59.1/67.5 ms, FOV: 180 × 180 mm, scan time: 8.03 min). Single-slice acquisition was used for T2 measurement to exclude undesirable factors, such as magnetization transfer [19] and cross-talk [20].
Region of interest setting and T2 measurement
The assessment of articular cartilage was performed using a coronal and sagittal T2-weighted FSE fat-saturated image. All MR images were transferred to a workstation, and T2 maps were reconstructed by fitting the T2 images pixel by pixel using custom-developed software (Baum2D, version 1.17; Osaka University, Osaka, Japan). For T2 measurement, the first echo was excluded to minimize T2 inaccuracy due to stimulated echoes. In the color scale, blue and red represented areas of short and long T2 values, respectively.
The acetabular and femoral cartilages were manually defined on the image corresponding to the second echo, and attention was paid not to include joint fluid with high signal intensity at the surface of the acetabular and femoral cartilages and subchondral plate with low signal intensity on the image with the second or later echo time.
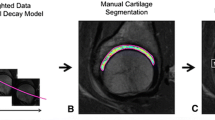
To evaluate the femoral head on coronal and sagittal view, the center of the femoral head was found using a concentric circle, and a vertical line going through the center of the head was drawn. On coronal view, the region of interest (ROI) was defined in the weight-bearing portion from the lateral edge of the fovea to the lateral side of the femoral head, with a 40° angle from the center line (Fig. 1a). On sagittal view, the ROI was defined at the weight-bearing portion of the femoral head within an angle of − 40° to 40° from the center line to minimize the effect of the magic angle (MAE) (Fig. 1e).

ROI setting and T2 measurement section for the description of the division of femoral and acetabular cartilage. a ROI setting of the femoral head on coronal view. b ROI setting of the acetabulum on coronal view. c Femoral head on coronal view. d Acetabulum on coronal view. e ROI setting of the femoral head on sagittal view. f ROI setting of the acetabulum on sagittal view. g Femoral head on sagittal view. h Acetabulum on sagittal view. Lower table shows the mean T2 value in the acetabulum on coronal view. SD standard deviation, ms mm second
To evaluate the acetabulum on coronal and sagittal views, the ROI was defined at the weight-bearing portion from the lateral edge of the acetabular fossa to the edge of the bony acetabulum (Fig. 1b–f). To evaluate the variation of the individual parts of the T2 value in hip cartilage following RAO, each acetabular and femoral cartilage was automatically divided into three radial sections with equal widths:
-
On coronal view
-
Femoral head (lateral part; Fl, center part; Fc, medial part; Fm) (Fig. 1c)
-
Acetabulum (lateral part; Al, center part; Ac, medial part; Am) (Fig. 1d)
-
On sagittal view
-
Femoral head (anterior part; Fa, center part; Fcs, posterior part; Fp) (Fig. 1g)
-
Acetabulum (anterior part; Aa, center part; Acs, posterior part; Ap) (Fig. 1h)
Subsequently, the mean T2 value within each section was calculated.
Evaluation design
Twelve normal volunteers, including five men and seven women (mean age, 30.6 years [range, 24–39 years]) without history of hip pain and hip disease were firstly evaluated with the same protocol. To evaluate the longitudinal qualitative assessment of articular cartilage following RAO, the mean T2 value of the individual part in each acetabular and femoral cartilage was evaluated preoperatively, at 6 months, and 1 and 2 years postoperatively on coronal and sagittal views, respectively. Furthermore, the interactions between the preoperative T2 values of each acetabulum and femoral head and clinical results of RAO at 2 years postoperatively were evaluated.
Statistical analysis
All data were expressed as mean ± standard deviation, and statistical significance was determined by repeated one-way analysis of variance. Correlations were evaluated using Pearson Chi-square test. A p value of < 0.05 was considered statistically significant.
Results
Based on the MR images of normal volunteers, the mean T2 values were 36.3 ± 4.9 and 36.5 ± 6.1 in the femoral head and acetabulum, respectively.
There was no case with OA progression in this study. The mean JOA score improved from 70.1 to 93.4 points, and radiographical data also improved 2 years postoperatively (Tables 1 and 2).
For the T2 values of the femoral head, the T2 value was the highest 6 months postoperatively, and significant differences were found between the T2 values preoperatively and those 2 years postoperatively, and between the T2 values of 6 months and those of 2 years post-operatively in all three regions on coronal view (Fig. 2). Similarly, on the sagittal view, the mean T2 value was the highest at 6 months postoperatively, and significant differences were found between the T2 values preoperatively and those 2 years postoperatively, and between the T2 values of 6 months and those of 2 years postoperatively in all three regions (Fig. 2). With regard to the acetabulum, the T2 values of the cartilage also increased 6 months postoperatively compared with those preoperatively, and decreased 2 years postoperatively on the coronal and sagittal views (Fig. 3). Significant differences between the T2 values preoperatively and those 2 years postoperatively, and between T2 values at 6 months and those 2 years postoperatively in all three regions on coronal and sagittal view. Especially in the center and medial region on coronal view, and center and posterior regions on sagittal view, the T2 values immediately decreased even at 1 year postoperatively compared with those preoperatively with statistical differences. With regard to the interaction between preoperative T2 values and JHEQ score at 2 years postoperatively, preoperative T2 values in Al were negatively correlated with postoperative JHEQ total and pain score, and the T2 values in Ac was negatively correlated with pain score in JHEQ with significance (Table 2). The T2 values in Aa were negatively correlated with all parameters in JHEQ. However, with regard to the T2 values in the femoral head, only the T2 values in Fcs was negatively correlated with JHEQ.

The upper figures show the mean T2 value of the cartilage in the femoral head on coronal view. Fl: The mean T2 value: pre; 40.2 ± 5.1, 6 m; 44.2 ± 7.5, 1 y; 40.5 ± 5.0, 2 y; 38.2 ± 1.9 (ms). FC: pre; 41.4 ± 7.9, 6 m; 42.5 ± 8.6, 1 y; 39.0 ± 4.5, 2 y; 36.6 ± 3.8 (ms). FM: pre; 43.0 ± 5.7, 6 m; 44.2 ± 7.8, 1 y; 41.5 ± 7.0, 2 y; 38.4 ± 5.3 (ms). The lower figures show the mean T2 value of the cartilage in the femoral head on sagittal view. Fa: The mean T2 value: pre; 45.5 ± 6.6, 6 m; 48.1 ± 7.9, 1 y; 42.1 ± 5.1, 2 y; 40.9 ± 6.0 (ms). Fcs: pre; 43.2 ± 7.7, 6 m; 50.0 ± 9.5, 1 y; 42.5 ± 5.5, 2 y; 41.3 ± 7.1 (ms). Fp: pre; 47.0 ± 6.0, 6 m; 51.0 ± 9.9, 1 y; 44.0 ± 5.5, 2 y; 43.2 ± 6.0 (ms)

The upper figures show the mean T2 value of the cartilage in the acetabulum on coronal view. Al: The mean T2 value: pre; 41.9 ± 8.2, 6 m; 44.3 ± 12.9, 1 y; 38.8 ± 9.5, 2 y; 34.4 ± 5.3 (ms). Ac: pre; 43.1 ± 5.0, 6 m; 44.2 ± 6.2, 1 y; 35.3 ± 7.9, 2 y; 36.4 ± 5.9 (ms). Am: pre; 47.8 ± 8.8, 6 m; 51.3 ± 11.9, 1 y; 41.7 ± 10.6, 2 y; 40.4 ± 14.6 (ms). The lower figures show the mean T2 value of the cartilage in the acetabulum on sagittal view. Aa: The mean T2 value: pre; 41.2 ± 9.3, 6 m; 44.2 ± 6.7, 1 y; 38.0 ± 5.8, 2 y; 35.1 ± 4.8 (ms). Acs: pre; 40.5 ± 7.2, 6 m; 44.2 ± 6.4, 1 y; 36.5 ± 5.8, 2 y; 36.6 ± 5.2 (ms). Ap: pre; 45.6 ± 5.8, 6 m; 46.2 ± 5.1, 1 y; 41.2 ± 6.1, 2 y; 39.5 ± 5.2 (ms)
Discussion
This is the first report to evaluate the articular cartilage with MRI T2 mapping following RAO and the interaction between the preoperative T2 values of the hip joint and clinical results of RAO. The present study suggests that cartilage degeneration occurs even in patients with DDH with early stage OA, and biomechanical and anatomical changes apparently cause decreased T2 values from 1 to 2 years postoperatively compared with those preoperatively. Furthermore, the preoperative T2 values of the acetabulum can be prognostic factors for the clinical results of RAO.
T2 mapping MRI has been reported to be a useful predictor of cartilage degeneration in the hip joint [21]. White et al. performed a direct comparison of histology and polarized light microscopy with T2 mapping after arthroscopic cartilage repair and demonstrated that this technique is sensitive and specific for the assessment of fibrous repair tissue [22]. Several knee studies have reported that T2 values of the repair site initially increased 3–13 months after autologous chondrocyte implantation, and it subsequently decreased over time [23]. Furthermore, Domayer et al. reported that the T2 values of the repair tissue are significantly lower than those of the native cartilage in the knee after microfracture; thus, lower T2 values may be an indicator for fibrous repair tissue composition and lower water content [24]. Goodwin et al. demonstrated that the local collagen fibril architecture in the cartilage modifies the anisotropic characteristics of the T2 relaxation [25]. The relative difference in T2 values between the native cartilage and the repair tissue may be explained by progressive loss of elasticity and increased stiffness.
The RAO procedure has been reported to be effective for mild-to-severe hip dysplasia in improving joint biomechanics and causing joint modeling [4, 5]. Joint modeling is a biological reaction caused by the change of mechanical balance in response to intra-articular load stress. RAO contributes to the change of distribution of load stress on the acetabulum but also to the medialization of the femoral head [26]. These biomechanical and anatomical changes could cause a decrease of stress in both the acetabulum and femoral head. Shimogaki et al. reported that RAO caused considerable changes in joint morphology and histological changes in the articular cartilage, particularly in the medial part of the acetabulum [27]. The experimental studies of RAO in a rabbit model indicated that chondrocytes/osteocytes were activated in the early postoperative stage in response to load stress [28, 29].
In this study, the T2 values of the cartilage in the femoral head and acetabulum are higher than those of healthy and asymptomatic adults that were previously reported [21]. The T2 values of the cartilage in the femoral head and acetabulum temporarily increased at 6 months postoperatively compared with those preoperatively; however, they gradually decreased at 1 and 2 years postoperatively compared with those preoperatively with statistical differences in all regions on coronal and sagittal planes. Several reports mentioned that cartilage degeneration occurs even in early stage OA from arthroscopic findings [29]. Hingsammer et al. reported that preoperative dGEMRIC index decreased after 1 and 2 years after periacetabular osteotomy (PAO) in the dGEMRIC study, and they concluded that PAO for developmental dysplasia of the hip alters the mechanical loading of articular cartilage in the hip, which in turn alters the cartilage matrix composition [30]. Our results showing several patients with preoperative high T2 values may suggest that there could be a variety of cartilage degeneration even in patients with DDH with early stage OA, and the extent of cartilage degeneration may affect the long-term radiographical and clinical results of RAO. Our results also suggested that biomechanical and anatomical changes could cause increased T2 values of the cartilage in an early stage postoperatively. However, they could apparently cause decreased T2 values 1–2 years postoperatively compared with those preoperatively, suggesting decreased mobility of the water molecules within the milieu of randomly oriented fibrous tissue. This may reflect an increase in the stiffness of the repair tissue over time, leading to cartilage modeling and maturation of repair tissue.
In addition, several reports mentioned that protected weight-bearing can affect the biosynthetic activity of the chondrocytes and proteoglycan content of the articular cartilage [31, 32]. Our results may suggest that excessive earlier weight loading of the operated hip might not have beneficial effects on the joint and cartilage modeling.
With the preoperative factors affecting the clinical results of RAO, our results indicated that the T2 values in the center to anterolateral region of the acetabulum affects the clinical results of RAO. Several reports suggested that the mechanical overload in dysplastic hips is more localized to the superior and superoanterior regions [30], and these areas, particularly in the acetabulum could be prognostic factors for clinical results of RAO, which cannot be evaluated by radiograph.
Our study has several limitations. First, movement of the acetabulum is not considered. Theoretically, the fragment moves anterolaterally in RAO; hence, there is a possibility that we did not evaluate the same portion of the acetabular cartilage, although we speculate that the postoperative comparison result is reliable even in the evaluation of the acetabulum. Second, single-slice acquisition was used for T2 mapping; for clinical studies, two-dimensional multi-slice acquisition has been shown to be available for T2 mapping of the cartilage [20]. Compared with single-slice acquisition, multi-slice acquisition has the advantage of enabling inspection of the whole cartilage area at one time. However, undesirable factors, such as magnetization transfer and cross talk, can cause inaccuracy in T2 measurement when multi-slice acquisition is used for cartilage imaging. Furthermore, the use of multi-slice acquisition with relatively high slice thickness can be a cause of larger volume averaging, particularly at the edge of the femoral head and acetabulum. To avoid these undesirable factors, single-slice acquisition with an imaging section that passes through the center of the femoral head and crosses the cartilage at a right angle was used in this study. Third, we did not consider the MAE because the reference ROIs were selected in weight-bearing areas at an orientation approximately perpendicular to the magnetic field. Nevertheless, MAE accounting for regional differences is unlikely [33, 34].
Despite several limitations, including the fact that further investigation with a larger number of patients is needed, our results indicated that cartilage degeneration could occur even in patients with DDH with early stage OA, and biomechanical and anatomical changes could apparently cause decreased T2 values from 1 to 2 years postoperatively compared with those preoperatively, suggesting cartilage modeling and maturation of repair tissue. Furthermore, the preoperative T2 values of the center to the anterolateral region of acetabulum can be prognostic factors for the clinical results of RAO.
References
Harris WH. Etiology of osteoarthritis of the hip. Clin Orthop Relat Res. 1986;213:20–33.
Hipp JA, Sugano N, Millis MB, Murphy SB. Planning acetabular redirection osteotomies based on joint contact pressures. Clin Orthop Relat Res. 1999;364:134–43.
Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am. 1984;66:430–6.
Yasunaga Y, Ochi M, Yamasaki T, Shoji T, Izumi S. Rotational acetabular osteotomy for pre- and early osteoarthritis secondary to dysplasia provides durable results at 20 years. Clin Orthop Relat Res. 2016;474(10):2145–53.
Yasunaga Y, Yamasaki T, Ochi M. Patient selection criteria for periacetabular osteotomy or rotational acetabular osteotomy. Clin Orthop Relat Res. 2012;470(12):3342–54.
Nieminen MT, Rieppo J, Töyräs J, Hakumäki JM, Silvennoinen J, Hyttinen MM, et al. T2 relaxation reveals spatial collagen architecture in articular cartilage: a comparative quantitative MRI and polarized light microscopic study. Magn Reson Med. 2001;46(3):487–93.
Regatte RR, Akella SV, Borthakur A, Kneeland JB, Reddy R. Proteoglycan depletion-induced changes in transverse relaxation maps of cartilage: comparison of T2 and T1rho. Acad Radiol. 2002;9(12):1388–94.
Burstein D, Velyvis J, Scott KT, Stock KW, Kim YJ, Jaramillo D, et al. Protocol issues for delayed Gd(DTPA)(2-)-enhanced MRI (dGEMRIC) for clinical evaluation of articular cartilage. Magn Reson Med. 2001;45(1):36–41.
Liess C, Lusse S, Karger N, Heller M, Gluer CC. Detection of changes in cartilage water content using MRI T2-mapping in vivo. Osteoarthr Cartil. 2002;10:90–13.
Bittersohl B, Kircher J, Miese FR, Dekkers C, Habermeyer P, Fröbel J, et al. T2* mapping and delayed gadolinium-enhanced magnetic resonance imaging in cartilage (dGEMRIC) of humeral articular cartilage—a histologically controlled study. J Shoulder Elb Surg. 2015;24(10):1644–52.
Dunn TC, Lu Y, Jin H, Ries M, Majumdar S. T2 relaxation time of cartilage at MR imaging: comparison with severity of knee osteoarthritis. Radiology. 2004;232:592–8.
Blumenkrantz G, Lindsey CT, Dunn TC, Jin H, Ries MD, Link TM, et al. A pilot, two-year longitudinal study of the interrelationship between trabecular bone and articular cartilage in the osteoarthritic knee. Osteoarthr Cartil. 2004;12:997–1005.
Regatte RR, Akella S, Lonner JH, Kneeland JB, Reddy R. T1r relaxation mapping in humanosteoarthritis (OA) cartilage: comparison of T1r with T2. J Magn Reson Imaging. 2006;23:547–53.
Li X, Ma B, Link TM, Castillo DD, Blumenkrantz G, Lozano J, Carballido-Gamio J, Ries M, Majumdar S. In vivo T1r and T2 mapping of articular cartilage in osteoarthritis of the knee using 3-T MRI. Osteoarthr Cartil 2007;789–97.
Baum T, Joseph GB, Nardo L, Virayavanich W, Arulanandan A, Alizai H, et al. Correlation of magnetic resonance imaging-based knee cartilage T2 measurements and focal knee lesions with body mass index: thirty-six-month follow-up data from a longitudinal, observational multicenter study. Arthritis Care Res (Hoboken). 2013;65(1):23–33.
Matsumoto T, Kaneuji A, Hiejima Y, Sugiyama H, Akiyama H, et al. Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ): a patient-based evaluation tool for hip-joint disease. The subcommittee on hip disease evaluation of the clinical outcome committee of the Japanese Orthopaedic Association. J Orthop Sci. 2012;17:25–38.
Croft P, Cooper C, Wickham C, Coggon D. Defining osteoarthritis of the hip for epidemiologic studies. Am J Epidemiol. 1990;132:514–22.
Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint: with special reference to the complication of osteo-arthritis. Acta Chir Scand. 1939;83(suppl 58):5–135.
Maier CF, Tan SG, Hariharan H, Potter HG. T2 quantitation of articular cartilage at 1.5 T. J Magn Reson Imaging. 2003;17:358–64.
Kneeland JB, Shimakawa A, Wehrli FW. Effect of intersection spacing on MR image contrast and study time. Radiology. 1986;158:819–22.
Watanabe A, Boesch C, Siebenrock K, Obata T, Anderson SE. T2 mapping of hip articular cartilage in healthy volunteers at 3T: a study of topographic variation. J Magn Reson Imaging. 2007;26:165–71.
White LM, Sussman MS, Hurtig M, Probyn L, Tomlinson G, Kandel R. Cartilage T2 assessment: differentiation of normal hyaline cartilage and reparative tissue after arthroscopic cartilage repair in equine subjects. Radiology. 2006;241(2):407–14.
Potter HG, Chong LR, Sneag DB. Magnetic resonance imaging of cartilage repair. Sports Med Arthrosc Rev. 2008;16:236–45.
Domayer SE, Kutscha-Lissberg F, Welsch G, Dorotka R, Nehrer S, Gabler C, et al. T2 mapping in the knee after microfracture at 3.0 T: correlation of global T2 values and clinical outcome e preliminary results. Osteoarthr Cartil. 2008;16:903–8.
Goodwin DW, Zhu H, Dunn JF. In vitro MR imaging of hyaline cartilage: correlation with scanning electron microscopy. Am J Roentgenol. 2000;174:405–9.
Ike H, Inaba Y, Kobayashi N, Yukizawa Y, Hirata Y, Tomioka M, et al. Effects of rotational acetabular osteotomy on the mechanical stress within the hip joint in patients with developmental dysplasia of the hip: a subject-specific finite element analysis. Bone Joint J. 2015;97-B(4):492–7.
Shimogaki K, Yasunaga Y, Ochi M. A histological study of articular cartilage after rotational acetabular osteotomy for hip dysplasia. J Bone Joint Surg Br. 2005;87:1019–23.
Yasunaga Y, Ochi M, Ikuta Y, Shimogaki K, Dohi D. Rotational acetabular osteotomies: a rabbit model. Arch Orthop Trauma Surg. 1997;116:74–6.
Yasunaga Y, Ikuta Y, Kanazawa T, Takahashi K, Hisatome T. The state of the articular cartilage at the time of surgery as an indication rotational acetabular osteotomy. J Bone Joint Surg Br. 2001;83-B:1001–4.
Hingsammer AM, Kalish LA, Stelzeneder D, Bixby S, Mamisch TC, Connell P, et al. Does periacetabular osteotomy for hip dysplasia modulate cartilage biochemistry? J Bone Joint Surg Am. 2015;97(7):544–50.
Tiderius CJ, Svensson J, Leander P, Ola T, Dahlberg L. dGEMRIC (delayed gadolinium-enhanced MRI of cartilage) indicates adaptive capacity of human knee cartilage. Magn Reson Med. 2004;51(2):286–90.
Rogers BA, Murphy CL, Cannon SR, Briggs TW. Topographical variation in glycosaminoglycan content in human articular cartilage. J Bone Joint Surg Br. 2006;88:1670–4.
Welsch GH, Mamisch TC, Domayer SE, Dorotka R, Kutscha-Lissberg F, Marlovits S, et al. Cartilage T2 assessment at 3-T MR imaging: in vivo differentiation of normal hyaline cartilage from reparative tissue after two cartilage repair procedures—initial experience. Radiology. 2008;247:154–61.
Mosher TJ, Smith H, Dardzinski BJ, Schmithorst VJ, Smith MB. MR imaging and T2 mapping of femoral cartilage: in vivo determination of the magic angle effect. Am J Roentgenol. 2001;177(3):665–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Shoji, T., Yamasaki, T., Izumi, S. et al. Evaluation of articular cartilage following rotational acetabular osteotomy for hip dysplasia using T2 mapping MRI. Skeletal Radiol 47, 1467–1474 (2018). https://doi.org/10.1007/s00256-018-2943-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-018-2943-3