
Abstract
Objective
The diagnosis of ankle syndesmosis injuries is made by various imaging techniques. The present study was undertaken to examine whether the three-dimensional reconstruction of axial CT images and calculation of the volume of tibiofibular joint space enhances the sensitivity of diastases diagnoses or not.
Design
Six adult cadaveric ankle specimens were used for spiral CT-scan assessment of tibiofibular syndesmosis. After the specimens were dissected, external fixation was performed and diastases of 1, 2, and 3 mm was simulated by a precalibrated device. Helical CT scans were obtained with 1.0-mm slice thickness. The data was transferred to the computer software AcquariusNET. Then the contours of the tibiofibular syndesmosis joint space were outlined on each axial CT slice and the collection of these slices were stacked using the computer software AutoCAD 2005, according to the spatial arrangement and geometrical coordinates between each slice, to produce a three-dimensional reconstruction of the joint space. The area of each slice and the volume of the entire tibiofibular joint space were calculated. The tibiofibular joint space at the 10th-mm slice level was also measured on axial CT scan images at normal, 1, 2 and 3-mm joint space diastases.
Results
The three-dimensional volume-rendering of the tibiofibular syndesmosis joint space from the spiral CT data demonstrated the shape of the joint space and has been found to be a sensitive method for calculating joint space volume. We found that, from normal to 1 mm, a 1-mm diastasis increases approximately 43% of the joint space volume, while from 1 to 3 mm, there is about a 20% increase for each 1-mm increase.
Conclusions
Volume calculation using this method can be performed in cases of syndesmotic instability after ankle injuries and for preoperative and postoperative evaluation of the integrity of the tibiofibular syndesmosis.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The rough medial convex surface of the distal fibula and the triangular fibular notch of the lateral surface of the distal tibia constitute the tibiofibular syndesmosis which is a fibrous joint with bones united by a strong interosseous ligament. In addition, the joint is stabilized in front and behind by the anterior, posterior and transverse tibiofibular ligaments [1, 2]. The syndesmotic ligaments resist the axial, rotational, and translational forces that attempt to separate these two bones [1, 3, 4]. From a biomechanical point of view, the anterior tibiofibular ligament is best positioned to resist external rotation. However, this ligament is the most commonly ruptured ligament in ankle fractures [3, 4].
Injury to the syndesmosis leads to severe ankle instability and requires a long recovery period [5, 6]. The relationship between tibia and fibula at the level of the ankle is of primary importance for the proper functioning of the distal tibiofibular joint. In regards to treatment and prognosis, it is important to know whether the syndesmosis is disrupted in cases of ankle fractures [7]. Tibiofibular syndesmotic diastasis without associated fibular fracture is easily overlooked.
The diagnosis of ankle syndesmosis injuries is made by various imaging techniques. CT scans have proven to be more sensitive than radiography [8]. However, even with the CT scan, it is difficult to measure a 1-mm diastasis [8]. To improve the sensitivity of CT scan imaging technique, we rendered the three-dimensional CT data of joint space and calculated the volume of tibiofibular joint space. This enhanced the ability of the CT-scan data to detect even a 1-mm diastasis.
The present study was undertaken to examine whether the three-dimensional reconstruction of axial CT images and calculation of the volume of the tibiofibular joint space enhances the sensitivity of diastases diagnoses or not. This novel technique of calculating joint space volume may allow better understanding of the pathoanatomy of tibiofibular diastasis and a system for preoperative planning to optimize the results of surgery.
Material and methods
This study was approved by our institutional review board. Six adult cadaveric ankle specimens (four males and two females) were used for CT-scan assessment of the tibiofibular syndesmosis. The specimens were dissected to the bone and all soft tissues except ankle ligaments were removed. The specimens were placed supine and the splinted extremities were neutrally positioned (right angle between ankle and the foot). Helical CT scans were obtained by Toshiba Aquillon CT scanner (120 kV, 200 mA) with a 1.0-mm slice thickness from the ankle mortise to the top of the fibular notch of the tibia for each specimen. The total number of CT slices was 20 for each specimen. The CT-scan data was transferred to the computer software AcquariusNET v1.6. Then the contours of the tibiofibular syndesmosis joint space were marked on each axial CT slice and the collection of these slices were stacked using the computer software AutoCAD 2005 according to the spatial arrangement and geometrical coordinates between each slice to produce a three-dimensional reconstruction of the joint space. The area of each slice was calculated. Then, the volume of entire tibiofibular joint space was calculated by the following formula:
whereV = volume,A = area, andT = thickness of the axial CT slice (1 mm).
The external fixation was done by K-wires. The K-wires were inserted 1 cm proximal to the ankle joint line on the anterior aspect of the tibia and fibula. The anterior tibiofibular ligament was cut and diastases of 1, 2 and 3 mm were simulated in a controlled manner using a precalibrated device (Fig. 1). Then a CT scan was taken for each of the 1, 2, and 3-mm diastases (Fig. 2). Three-dimensional reconstruction of the axial images of all specimens was performed again and their volumes were calculated using Auto-CAD 2005 software (Fig. 3). All results were analyzed by two independent observers.

Simulation of the tibiofibular diastasis by external fixator (the anterior tibiofibular ligament is cut)

Axial CT scan images of normal, 1, 2, and 3-mm diastases of tibiofibular syndesmosis at 1 cm proximal to the ankle joint line. (Arrows indicate the diastases)

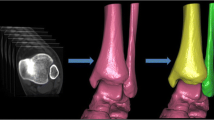
Three-dimensional volume rendered image of the tibiofibular syndesmosis joint space: a Anterior, b superior, c inferior view
The tibiofibular joint space at the 10th-mm slice level (1 cm proximal to the ankle joint line) was also measured on the axial CT scans images for all specimens at normal and 1, 2 and 3-mm joint space diastases (Fig. 2). The 1-cm proximal level from the ankle joint line is routinely used to assess tibiofibular joint diastases on radiographs and axial CT scan images [8].
The statistical analysis was done with SPSS v11.0. The mean and percentage values for area and volume calculations were calculated. The Student’st test was used to calculate thep value for the difference between the interobserver measurements and normal, 1, 2 and 3 mm diastases of the axial CT scan and volume measurements.
Results
The three-dimensional volume rendering of the tibiofibular syndesmosis from the axial CT scan data demonstrated the shape of the joint space (Fig. 3). All 1–3-mm diastases could be clearly visualized on the three-dimensional reconstructed joint-space volume model. This permitted the calculation of the volume of joint space for the respective diastases value (Tables 1, 2).
Comparison of each 1-mm slice area between normal, 1, 2, and 3 mm diastases of tibiofibular syndesmosis is shown in Fig. 4. The difference between normal mean tibiofibular joint volume and mean volume after 1 mm diastasis; between mean volume after 1 and 2-mm diastasis; and between mean volume after 2 and 3 mm-diastasis was statistically significant (p<0.05). The percentage increase in volume from normal to 1 mm was 43%. The percentage increase in the joint space volume was approximately 20% for 1–2-mm and 2–3-mm diastases (p<0.05) (Table 2).

Comparison of the each 1-mm slice area between normal, 1, 2, and 3-mm diastases of tibiofibular syndesmosis (20 slices total)
There was no statistically significant difference (p>0.05) in the measurement of the tibiofibular distance between the normal and the 1-mm axial CT-scan slices. However, a statistically significant difference (p<0.05) of measurements of the distance between the tibia and fibula was noted between the 1 and 2 mm and the 2 and 3-mm diastases slices on the axial CT image at a 1-cm proximal level to the ankle joint line (Table 3).
Discussion
A novel technique of three-dimensional volume rendering of tibiofibular joint space was assessed to diagnose syndesmotic diastasis. Several authors have compared radiographic, computed tomography, MRI and arthroscopy methods to diagnose the syndesmotic disruption [7–10].
Several radiographic measurements have been described such as tibiofibular clear space and overlap, which are used to determine ligamentous injury in ankle fractures, especially of the syndesmosis complex [11, 12]. Although several of these measurements have been shown to have good observer reliability [9], their clinical utility and predictive value have not been substantiated. Numerous investigators have questioned the utility of various radiographic measurements for predicting syndesmotic rupture [7, 10, 13–15]. Syndesmotic injury may be difficult to understand by radiographic criteria. Harper [15] and Beumer et al. [13] suggested that rotation of the ankle affects radiographic measurements and preclude reliable prediction of soft-tissue injuries. The large interobserver variability and difficulty in positioning multi-trauma patients limits the sensitivity and reliability of radiographs [16].
An intact syndesmosis is critical in maintaining normal ankle function; even just a 1-mm diastasis could cause a decrease of the tibiotalar contact area by 42%. This minor widening leads to an increase in tibiotalar contact stresses and ultimately early arthrosis of the tibiotalar joint [17]. Harper [18] found that the fibula and attached ligaments were major factors in preventing talar shift, both mediolaterally and anteriorly. The lateral supporting structures were also noted as securely stabilizing the talus against posterior subluxation in the absence of the posterior and medial malleoli [18]. Thus, it is essential to consider both ligamentous and bony structures while assessing the congruity of the tibiofibular syndesmosis. Investigators have described the importance of evaluating and ensuring stability of the ankle after fracture to optimize outcomes [12, 14]. The diastasis of the tibiofibular syndesmosis is one of the causes of functional instability that is often overlooked and may result in chronic ankle instability, pain, and arthritis.
Conventionally, the distance between tibial and fibular edges on the 10th-mm axial slice (1 cm proximal to the ankle joint line) is measured for the diagnosis of tibiofibular diastasis. Our approach was to measure the change in joint volume with diastasis because we hypothesize that a measurement at the 10th mm axial slice may not be representative of the whole joint space. A study by Ebraheim et al. [8] demonstrated that it is not possible to measure a 1-mm diastasis on the 10th mm axial slice. The minimum diastasis that they could measure was 2 mm. A 1-mm diastasis could not be detected either on the radiographs or the CT scans. However, Ebraheim et al. [19] found that tibiofibular syndesmosis assessment by CT scan is easier to perform and more reliable than radiographic diagnosis. Also, CT scan images could be used for preoperative planning and postoperative follow up [19].
Muratli et al. [7], according to their clinical study, suggested that conventional radiography and even MRI is not sufficient in assessing syndesmotic disruption, and that magnetic resonance arthrography (MRA) may make an important contribution to diagnosis in ankle fractures.
Oae et al. [20] found that MRI is quite sensitive in the diagnosis of tibiofibular syndesmosis. However, the diagnosis is based on the appearance of ligaments, which was done to diagnose the diastasis and ligament injury. However, they noted that in some cases where ligamentous anatomy is variable or where there is intra-articular bleeding, the diagnosis becomes difficult by MRI alone [20].
Brown et al. [21] assessed the ankle syndesmotic injury based on criteria that involved the appearance of ligaments on MRI, distal tibiofibular joint congruity and the height of the tibiofibular recess (from the lateral talar dome to the maximal superior extent of joint fluid between the tibia and fibula). They found that normal tibiofibular recess height is approximately 5.4 mm, which increased from 10 to 15 mm in cases of syndesmotic injury. They were not able to calculate the volume of recess fluid. Our technique utilized the three dimensional rendering technique. Using our technique, we were able to reconstruct tibiofibular syndesmotic joint space shape (from the ankle mortise to the top of the triangular shaped fibular notch of the tibia) after simulated diastases and calculate the volume of the resulting space (Fig. 3a–c). Brown et al. [21] used MRI with 4 mm slice thickness to see joint fluid in the tibiofibular recess. To reconstruct the exact structure of the joint space it is important to have at least 1-mm slice thickness so that three dimensional details are not missed. We used 1-mm-thick slices of CT scan axial images to reconstruct joint shape and calculate volume.
Takao et al. [10] in their clinical study compared the accuracy of standard anteroposterior radiography, mortise radiography and MRI with arthroscopy of the ankle for the diagnosis of a tear of the tibiofibular syndesmosis. They suggested that standard AP and mortise radiography did not always provide a correct diagnosis, and MRI was useful although there were two false-positive cases. They concluded that arthroscopy of the ankle is indispensable for the accurate diagnosis of a tear of the tibiofibular syndesmosis. However, it is not possible to measure exactly the tibiofibular diastasis.
Pelc et al. [22] found that signal intensities of MRI between bone and soft-tissue structures vary with the pulse sequence and makes processing more difficult than with CT data. Another factor that compounds the difficulty in three-dimensional rendering of MRI data is that absolute signal intensities vary across images as a result of the sensitivity profiles of the radiofrequency coil. This variation makes any “standardized” remapping of signal intensities to opacify tranformations impossible. With CT, regional variations in density may occur because of artifacts such as beam hardening, but in general, there is consistency between subjects and body regions. Thus, it is easier to reconstruct a three-dimensional model from a CT scan than from MRI [22].
Three-dimensional volume rendering of axial CT data is useful for demonstrating the relationship between ankle ligaments, tendons and the underlying osseous structures. Volume rendered imaging has become a common three-dimensional display technique [23, 24]. The rendered image data with usual methods of three-dimensional reconstruction provide almost no depth cues, but the assignment of the various tissue opacities result in the appearance of depth.
The original data of three-dimensional reconstructed images come from two-dimensional images. The larger the original data, the more detailed the three-dimensional reconstruction is. The key to collecting sufficient original data lies in section thickness and saw-path loss. If the section thickness and saw-path loss are too large, the factual information between two sections will be significantly decreased [25].
The precise location of the articular surfaces of the tibiofibular syndesmosis may be difficult to appreciate on routine axial scans. The availability of multiplanar reformatted images created from the CT data provides an additional perspective that improves depiction of the ankle joint anatomy [26].
In this study, three-dimensional anatomical data of the tibiofibular syndesmosis joint was obtained by the integrated viewing of multiple consecutive planar CT slices. Stacking of CT slices by a computer allowed recreating images of the anatomy as three-dimensional images (Fig. 3).
We found that the difference in measurement of the tibiofibular distance between the normal and 1-mm diastasis on the axial CT scan was not statistically significant and in many cases was difficult to visualize properly. However, it was possible to measure 2 and 3 mm diastases (Table 3).
Considering the limitations of axial CT-scan images such as the difficulty in measuring diastases less than 2 mm and the usage of 10th-mm axial scan (1 cm proximal to the ankle joint line) to measure diastases which may not represent the whole joint space, we found that our technique of three-dimensional volume rendering of the axial CT-scan images of the entire tibiofibular joint combined with the calculation of the joint volume is more sensitive than earlier methods. We have shown that change in total joint volume is very sensitive to even a 1-mm diastasis (Table 2).
Pretorius et al. [27] found that spiral CT with volume rendering is often able to compensate for streak artifacts, and studies are usually quite successful despite the presence of metal plates, pins, or prostheses.
The current study demonstrated that even 1 mm diastasis of the tibiofibular syndesmosis with ruptured anterior tibiofibular ligament could be recognized by calculating volume of joint space. The volume changed significantly with even 1-mm diastases. Normal joint space volume was mean 1020.31 and it increased 43% with a 1-mm increase in joint space and 20% with each 1 mm increase from 1 to 3 mm (Table 2 and Fig. 5). This finding indicates that a mere 1-mm joint space diastasis can disrupt congruity and may be the reason of chronic ankle pain and development for arthritis.

Comparison of the tibiofibular syndesmosis joint space volume between normal, 1, 2, and 3-mm diastases of tibiofibular syndesmosis
The methods of our study included the simulation of diastases from 1 to 3 mm and the calculation of the resulting change in syndesmotic joint space volume. The muscles and ligaments provide essential stabilizing function to the joints. In any case, we did not study the stabilizing function of individual ligaments and muscles. We created the de-stabilization by producing diastases and calculated the change in volume. However, in the future, the diastases could be studied with intact muscles and ligaments in order to analyze their role in tibiofibular syndesmosis joint space volume change.
There are some other limitations of our study including the possible variation in outlining the joint space on axial CT scans. However to minimize that, two independent observers made the measurements and we did not find any statistically significant difference between their measurements. Secondly, the process is time consuming and requires a longer learning curve for the operator. If computer software could be developed which outlines the area of the individual axial CT slice, makes the stack of slices of joint space, and calculates the volume of the joint space without having the need to transfer the slices to other computer software, then the assessment of tibiofibular joint space will be much easier and quicker.
We hope that our study will provide a baseline for other researchers, and that computer programmers will develop faster techniques for calculating the joint volume. The results of this study provide an understanding of volumetric changes regarding ankle diastasis.
Conclusions
The three-dimensional volume rendering of the tibiofibular syndesmosis joint space from the spiral CT data demonstrated the shape of the joint space. Three-dimensional volume rendering of the spiral CT data has been found to be a very precise method for calculating joint space volume. We found that, from normal to 1 mm, a 1-mm diastasis increases approximately 43% of the joint space volume, while from 1 to 3 mm there is about a 20% increase for each 1-mm increase.
References
Williams A, Davies MS. Ankle and Foot. In: Standring S, editor. Gray’s anatomy. London: Churchill Livingstone; 2005. p. 1525
Romanes GJ. Cunningham’s textbook of anatomy. London: Oxford University Press; 1972. p. 247–249
Gumann G. Ankle Fractures. In: Scurran BL, editor. Foot and ankle trauma. Churchill Livingstone; 1990. p. 579–625
Snedden MH, Shea JP. Diastasis with low distal fibula fractures: an anatomic rationale. Clin Orthop Relat Res 2001;382:197–205
Boytim MJ, Fischer DA, Neumann L. Syndesmotic ankle sprains. Am J Sports Med 1991;19:294–298
Pankovich AM. Fractures of the fibula at the distal tibiofibular syndesmosis. Clin Orthop Relat Res 1979;143:138–147
Muratli HH, Bicimoglu A, Celebi L, Boyacigil S, Damgaci L, Tabak AY. Magnetic resonance arthrographic evaluation of syndesmotic diastasis in ankle fractures. Arch Orthop Trauma Surg 2005;125(4):222–227
Ebraheim NA, Lu J, Yang H, Mekhail AO, Yeasting RA. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: a cadaver study. Foot Ankle 1997;18(11):693–698
Brage ME, Bennett CR, Whitehurst JB, Getty PJ, Toledano A. Observer reliability in ankle radiographic measurements. Foot Ankle Int 1997;18(6):324–329
Takao M, Ochi M, Oae K, Naito K, Uchio Y. Diagnosis of a tear of the tibiofibular syndesmosis: the role of arthroscopy of the ankle. J Bone Joint Surg Br 2003;85(3):324–329
Bozic KJ, Jaramillo D, DiCanzio J, Zurakowski D, Kasser J. Radiographic appearance of the normal distal tibiofibular syndesmosis in children. J Pediatr Orthop 1999;19(1):14–21
Harper MC, Keller TS. A radiographic evaluation of the tibiofibular syndesmosis. Foot Ankle Int 1989;10(3):156–160
Beumer A, Van Hemert WLW, Niesing R, et al. Radiologic measurement of the distal tibiofibular syndesmosis has limited use. Clin Orthop Related Res 2004;423:227–234
Ebraheim NA, Mekhail AO, Gargasz SS. Ankle fractures involving the fibula proximal to the distal tibiofibular syndesmosis. Foot Ankle Int 1997;18(8):513–521
Harper MC. An anatomic and radiographic investigation of the tibiofibular clear space. Foot Ankle 1993;14(8):455–458
Beumer AB, Swiersta A. The influence of ankle positioning on the radiography of the distal tibial tubercles. Surg Radiol Anat 2003;25:446–450
Ramsey PL, Hamilton W. Changes in tibiotalar area of contact caused by lateral talar shift. J Bone Joint Surg 1976;58A:356–357
Harper MC. Talar shift. The stabilizing role of the medial, lateral, and posterior ankle structures. Clin Orthop 1990;257:177–183
Ebraheim NA, Elgafy H, Panadilam T. Syndesmotic disruption in low fibular fractures associated with deltoid ligament injury. Clin Orthop Related Res 2003;409:260–267
Oae K, Takao M, Naito K, et al. Injury of the tibiofibular syndesmosis: value of MR imaging for diagnosis. Radiology 2003;227:155–161
Brown KW, Morrison WB, Schweitzer ME, et al. MRI findings associated with distal tibiofibular syndesmosis injury. AJR 2004;182:131–136
Pelc JS, Beaulieu CF. Volume rendering of tendon-bone relationships using unenhanced CT. AJR 2001;176:973–977
Calhoun PS, Kuszyk BS, Heath DG, Carley JC, Fishman EK. Three-dimensional volume rendering of spiral CT data: theory and method. Radiographics 1999;19:745–764
Choplin RH, Buckwalter KA, Rydberg J, Farber JM. CT with 3D rendering of the tendons of the foot and ankle: technique, normal anatomy, and disease. Radiographics 2004;24(2):343–356
Sha Y, Zhang SX, Liu ZJ, et al. Computerized 3D reconstructions of the ligaments of the lateral aspect of ankle and subtalar joints. Sur Radiol Anat 2001;23:111–114
Woolson ST, Dev P, Fellingham LL, Vassiliadis A. Three-dimensional imaging of the ankle joint from computerized tomography. Foot Ankle 1985;6(1):2–6
Pretorius ES, Fishman EK. Volume-rendered three-dimensional spiral CT: musculosceletal applications. Radiographics 1999;19:1143–1160
Acknowledgement
We are thankful to Mr. Arif B. Taser for his valuable assistance in generating the three-dimensional model using AutoCAD computer software.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was approved by the Institutional Review Board. The authors did not receive grants or outside funding in support of their research or preparation of this manuscript. They did not receive payments or other benefits or a commitment or agreement to provide such benefits from a commercial entity. No commercial entity paid or directed, or agreed to pay or direct, any benefits to any research fund, foundation, educational institution, or other charitable or nonprofit organization with which the authors are affiliated or associated.
Rights and permissions
About this article
Cite this article
Taser, F., Shafiq, Q. & Ebraheim, N.A. Three-dimensional volume rendering of tibiofibular joint space and quantitative analysis of change in volume due to tibiofibular syndesmosis diastases. Skeletal Radiol 35, 935–941 (2006). https://doi.org/10.1007/s00256-006-0101-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-006-0101-9