
Abstract
Kawasaki disease (KD) is a self-limiting systemic vasculitis of unknown etiology. KD is often complicated by coronary artery aneurysms (CAAs), which develop in about 20–25% of untreated children and 3–5% of children treated with intravenous immunoglobulin therapy. To identify the risk loci for CAA susceptibility in patients with KD, we performed a genome-wide association study (GWAS) using our previous Illumina HumanOmni1-Quad BeadChip data (296 KD patients) and a new replication study in an independent sample set (713 KD patients) by grouping KD patients without CAA (control) versus KD patients with extremely large aneurysms (diameter ≥ 5 mm) (case). Among 44 candidate single -nucleotide polymorphisms (SNPs) selected from the initial GWAS data (33 cases vs. 215 controls), a SNP (rs899162) located 7 kb upstream of the TIFAB gene on chromosome five was replicated in an independent sample (12 cases vs. 532 controls). In the combined analysis (45 cases vs. 747 controls), the SNP (rs899162) showed a highly significant association with CAA formation (diameter ≥ 5 mm) in patients with KD (odds ratio = 3.20, 95% confidence interval = 2.02–5.05, Pcombined = 1.95 × 10−7). These results indicate that the TIFAB gene may act as a CAA susceptibility locus in patients with KD.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Kawasaki disease (KD) is the leading cause of acquired heart disease in children in developed countries due to self-limiting systemic vasculitis [1]. KD is often complicated by coronary artery aneurysms (CAAs), which occur in 20–25% of untreated children and 3–5% of children treated with intravenous immunoglobulin (IVIG) [2, 3]. Aneurysms can be classified as small (< 5 mm internal diameter), medium (5–8 mm internal diameter), or giant (> 8 mm internal diameter) [4]. Approximately 20% of patients with a CAA may also subsequently require invasive cardiac treatment [5]. Coronary arteritis in patients with KD is known to lead to CAA with destruction of the vascular media and infiltration of inflammatory cells, including neutrophils, macrophages, dendritic cells, IgA plasma cells, and T cells [6,7,8,9]. These studies suggest that excessive inflammatory cell infiltration is important in the pathogenesis of CAAs in patients with KD.
Although the etiology of CAA in patients with KD remains unknown, efforts have been directed to reduce the development of CAAs. Clinical risk factors for CAA include long fever duration, IVIG resistance, male gender, and incomplete KD [10,11,12,13,14,15,16,17]. Despite the clinical importance of CAA in patients with KD, very limited numbers of genome-wide association studies (GWAS) using a small number of samples were performed to search genetic susceptibility loci for CAA formation in these patients [18, 19]. However, all of the suggested genetic loci for CAA formation have not been replicated by either the original study group or other independent investigators. We also previously performed a GWAS analysis using Affymetrix SNP chip data from KD cases only by grouping 49 patients with KD and a large aneurysm (diameter ≥ 5 mm) versus 314 patients with KD without CAA and identified one CAA-associated locus, the rs17136627 SNP in the potassium intermediate/small conductance calcium-activated channel, subfamily N, member 2 (KCNN2) gene [20]. In this study, we performed a GWAS analysis using Illumina BeadChip data with a large number of case and control samples to identify additional CAA susceptibility genes in patients with KD.
Methods
Study Subjects and Genotype Data
All 1009 of our patients with KD were diagnosed by pediatricians according to the diagnostic criteria of the American Heart Association [1]. Information detailing the samples has been described in our previous studies [21, 22]. For genetic study, whole blood samples (approximately 5 ml) were collected from each patient at either acute, subacute, convalescent, or normal stage. Genomic DNA was extracted from whole blood samples using the PUREGENE DNA purification kit (Gentra Systems, Minneapolis, MN) according to the manufacturer’s instructions. Patients with KD were classified as having CAAs if the largest lumen diameter of the coronary artery was ≥ 3 mm. A total of 296 patients with KD were genotyped for the GWAS on the Illumina HumanOmni1-Quad BeadChip, following the manufacturer’s instructions (Illumina, San Francisco, CA, USA). All samples had a genotyping call rate of > 98%. To filter the SNP markers, we excluded SNPs with a call rate ≤ 95% in samples, minor allele frequency ≤ 0.01, and deviation from Hardy–Weinberg equilibrium (P ≤ 0.0001). Genotyping for the replication study in the additional 713 patients with KD was performed on the high-throughput Fluidigm SNPtype system (Fluidigm Corp., San Francisco, CA, USA) using the Fluidigm SNPType™ assay platform. This study was approved by our institutional review board (IRB) at Asan Medical Center (IRB No. 2014-0823) and informed consent was obtained from the parents of the patients with KD.
Statistical Analysis
The genetic associations among single-nucleotide polymorphisms (SNPs) were analyzed using PLINK (ver. 1.07) [23]. A Chi-square test was performed to compare allelic frequencies between the cases and the controls. Genetic associations were estimated using odds ratios (ORs) with 95% confidence intervals (CIs). From the initial GWAS analysis, 44 candidate SNPs for a replication study were chosen by selecting loci that were involved with cardiac functions or immune responses and that had significant P-values (P < 0.001). Regional association plots and local linkage disequilibrium (LD) values were generated from the GWAS results using LocusZoom software [24].
Results
A SNP (rs899162) Located 7 kb Upstream of the TIFAB Gene is Associated with CAA in Patients with KD
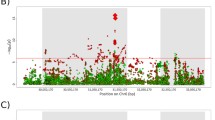
To identify the genetic variants associated with CAA formation in patients with KD, we initially carried out a GWAS using the Illumina Omni1-Quad BeadChip data from 248 patients with KD, including 215 KD patients without CAAs (control) and 33 patients with CAAs (diameter ≥ 5 mm) (case). We selected 44 candidate SNPs showing significant associations with CAA formation in the patients with KD for the replication study (P < 0.001) from functionally immune- or cardiovascular-related genes and examined them in an independent sample set consisting of 544 patients with KD (532 patients without CAA and 12 patients with CAA, diameter ≥ 5 mm) (Supplementary Table 1). Among 44 candidate SNPs, a SNP (rs899162) located 7 kb upstream of the TIFAB gene for CAA formation (diameter ≥ 5 mm) was replicated with significance in patients with KD (OR 3.20, 95% CI 2.02–5.05, Pcombined = 1.95 × 10−7) (Table 1). This locus contained the TIFAB and DCANP1 genes (Fig. 1), indicating that either the TIFAB and/or the DCANP1 gene is a CAA susceptibility gene. Interestingly, the risk genotype (AA or AG) of the significantly associated SNP rs899162 in the TIFAB-DCANP1 locus was enriched in KD patients with large aneurysms (diameter ≥ 5 mm) (Fig. 2).

Regional association plot of the novel TIFAB-DCANP1 (rs899162) locus for CAA susceptibility from the results of our initial genome-wide association study data analysis using 33 patients with CAAs (diameter ≥ 5 mm) versus 215 patients without a CAA. The vertical axis shows the negative logarithm of the association P-values, and the horizontal axis shows the position in mega bases. The estimated recombination rates (right y-axis) were established based on 1000 Genomes Project Asian data (November 2014). The color of each SNP is based on the linkage disequilibrium (r2) with the lead SNP rs899162 for the TIFAB-DCANP1 locus (shown in purple). CAA coronary artery aneurysm, SNP single-nucleotide polymorphism

Distribution of the risk genotype frequency of rs899162 (risk allele: A) in the TIFAB-DCANP1 locus according to the size of the CAA. The rs899162 genotypes are shown on the top of the figure by CAA size: normal, non-CAA; small, < 5 mm internal diameter; medium, 5–8 mm internal diameter; giant, > 8 mm internal diameter. CAA coronary artery aneurysm
Discussion
KD is the leading cause of heart disease in children due to acute febrile and systemic vasculitis of unknown origin. Here, we performed a GWAS and a replication study in an independent sample set to identify genetic loci for CAA susceptibility. We found that a SNP (rs899162) located 7 kb upstream of the TIFAB gene was significantly associated with the extreme phenotype of CAA formation (≥ 5 mm diameter) in KD patients with a large effect size (OR 3.20, 95% CI 2.02–5.05, P = 1.95 × 10−7). This locus contained the TIFAB and DCANP1 genes, suggesting that either the TIFAB or DCANP1 gene may play a role as a CAA susceptibility gene.
The TIFAB gene was identified by a homology search of the human and mouse genomic databases for TIFA with the FHA domain [25]. TIFAB is mainly expressed in B cells, dendritic cells, and macrophages [26]. In addition, TIFAB is associated with TIFA and inhibits TIFA-mediated activation of nuclear factor-kappa-B [27]. TIFAB is also known to be a negative regulator of TRAF6-induced cell proliferation and maturation in hematopoiesis [26]. TIFAB is also a haploinsufficient gene in del (5q) myelodysplastic syndrome that shows skewed proportions of hematopoietic stem/progenitor cells and altered myeloid differentiation, resulting in blood cytopenia, myeloid dysplasia, and a predisposition to acute myeloid leukemia or bone marrow failure [27]. In contrast, DCANP1, which is mainly localized in the perinucleus, is highly expressed in mature dendritic cells, whereas it is poorly expressed in immature dendritic cells and not expressed in monocytes or B cells [28]. Interestingly, unlike other febrile diseases, the number of circulating myeloid dendritic cells decreases during the acute phase of KD [29] and arterial mature myeloid dendritic cells accumulate in the coronary arterial wall with CD3+ T cells [8]. These data suggest that the dysregulation of TIFAB- or the DCANP1-mediated inflammatory response plays a role in the development of CAA formation in patients with KD.
As the TIFAB and DCANP1 genes are in same LD block of SNP rs899162, it is unknown which gene is the CAA susceptibility gene. However, the most significant CAA-associated SNP (rs899162) was located closer to TIFAB (7 kb upstream of the TIFAB gene) rather than the DCANP1 gene (11.9 kb upstream of the DCANP1 gene). In addition, a tightly linked SNP (rs1031844) of the eQTL SNP in the DCANP1 gene (rs13154143, located 456 bp upstream of the DCANP1 gene) (P = 1.22 × 10−13) was not associated (P = 0.063) with CAA formation in patients with KD (Supplementary Table 2). These data strongly suggest that TIFAB is more likely the causative susceptibility gene for CAA formation in patients with KD. However, we cannot exclude DCANP1 as a potential candidate gene for CAA formation. Although the tightly linked SNPs of the eQTL SNP in the DCANP1 gene were not associated with CAA formation, a CAA-associated SNP (rs899162) located 7 kb upstream of the TIFAB gene has been reported to be associated with expression of the DCANP1 gene in whole blood in a previous eQTL study (P = 3.52 × 10−7) [30] (Supplementary Table 2). This result may support the possibility of differential expression of DCANP1 by the CAA-associated SNP rs899162 genotype, subsequently playing a role as a susceptibility gene for CAA formation. Furthermore, to identify any potential functional coding variants in the TIFAB and DCANP1 genes associated with CAA formation in patients with KD, we also examined our whole exome sequencing data, containing 22 KD patients with CAAs (diameter ≥ 5 mm) and 126 KD patients without CAAs. However, we could not find any coding variants in the TIFAB and DCANP1 genes associated with CAA formation in the patients with KD (data not shown). This result suggests that allelic gene expression in TIFAB-DCANP1 locus plays an important role in CAA formation in patients with KD.
A limited number of GWAS was performed to identify genetic markers for coronary artery aneurysm in Kawasaki disease [18,19,20]. However, all these previous GWAS used small sample size (less than 100 cases with CAA). The strengths of our study were that we used a genome-wide SNP array chip comprising approximately 1,000,000 SNPs and relatively large sample size (a total of 216 cases with CAA) to identify a new locus that has not been previously reported. However, the P-value of rs899162 in TIFAB locus did not reach genome-wide significance, and it was not validated in other ethnic population yet.
In conclusion, we identified a SNP (rs899162) located 7 kb upstream of the TIFAB gene, which is significantly associated with CAA formation in patients with KD. This result suggests that TIFAB plays an important role in the pathogenesis of CAA in these patients. Further larger studies are required to validate whether this candidate locus plays a role as a CAA susceptibility gene. It is also necessary to validate a functional role for TIFAB and DCANP1 as well as the CAA-associated SNP (rs899162) in CAA susceptibility.
References
McCrindle BW, Rowley AH, Newburger JW et al (2017) Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation 135:e927–e999
Burns JC, Glodé MP (2004) Kawasaki syndrome. Lancet 364:533–544
Burns JC (2007) The riddle of Kawasaki disease. N Engl J Med 356:659–661
Newburger JW, Takahashi M, Gerber MA et al (2004) Diagnosis, treatment, and long-term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young. Am Heart Assoc Circ 110(17):2747–2771
Kato H, Sugimura T, Akagi T et al (1996) Long-term consequences of Kawasaki disease. A 10- to 21-year follow-up study of 594 patients. Circulation 94:1379–1385
Takahashi K, Oharaseki T, Naoe S et al (2005) Neutrophilic involvement in the damage to coronary arteries in acute stage of Kawasaki disease. Pediatr Int 47:305–310
Brown TJ, Crawford SE, Cornwall ML et al (2001) CD8 T lymphocytes and macrophages infiltrate coronary artery aneurysms in acute Kawasaki disease. J Infect Dis 184:940–943
Yilmaz A, Rowley A, Schulte DJ et al (2007) Activated myeloid dendritic cells accumulate and co-localize with CD3+ T cells in coronary artery lesions in patients with Kawasaki disease. Exp Mol Pathol 83:93–103
Rowley AH, Shulman ST, Mask CA et al (2000) IgA plasma cell infiltration of proximal respiratory tract, pancreas, kidney, and coronary artery in acute Kawasaki disease. J Infect Dis 182:1183–1191
Liang CD, Kuo HC, Yang KD et al (2009) Coronary artery fistula associated with Kawasaki disease. Am Heart J 157:584–588
Ruan Y, Ye B, Zhao X (2013) Clinical characteristics of Kawasaki syndrome and the risk factors for coronary artery lesions in China. Pediatr Infect Dis J 32:e397–e402
Friedman KG, Gauvreau K, Hamaoka Okamoto A et al (2016) Coronary artery aneurysms in Kawasaki disease: risk factors for progressive disease and adverse cardiac events in the US population. J Am Heart Assoc 5:e003289–e003219
Ha KS, Jang G, Lee J et al (2013) Incomplete clinical manifestation as a risk factor for coronary artery abnormalities in Kawasaki disease: a meta-analysis. Eur J Pediatr 172:343–349
Maric LS, Knezovic I, Papic N et al (2015) Risk factors for coronary artery abnormalities in children with Kawasaki disease: a 10-year experience. Rheumatol Int 35:1053–1058
Song D, Yeo Y, Ha K et al (2009) Risk factors for Kawasaki disease-associated coronary abnormalities differ depending on age. Eur J Pediatr 168:1315–1321
Burns JC, Capparelli EV, Brown JA et al (1998) Intravenous gamma-globulin treatment and retreatment in Kawasaki disease. US/Canadian Kawasaki Syndrome Study Group. Pediatr Infect Dis J 17:1144–1148
Callinan LS, Tabnak F, Holman RC et al (2012) Kawasaki syndrome and factors associated with coronary artery abnormalities in California. Pediatr Infect Dis J 31:894–898
Lin YJ, Chang JS, Liu X et al (2015) Genetic variants in PLCB4/PLCB1 as susceptibility loci for coronary artery aneurysm formation in Kawasaki disease in Han Chinese in Taiwan. Sci Rep 5:14762
Kuo HC, Li SC, Guo MMH et al (2016) Genome-wide association study identifies novel susceptibility genes associated with coronary artery aneurysm formation in Kawasaki disease. PLoS ONE 11:e0154943–e0154916
Kim JJ, Park YM, Yoon D et al (2013) Identification of KCNN2 as a susceptibility locus for coronary artery aneurysms in Kawasaki disease using genome-wide association analysis. J Hum Genet 58:521–525
Kim JJ, Yun SW, Yu JJ et al (2017) A genome-wide association analysis identifies NMNAT2 and HCP5 as susceptibility loci for Kawasaki disease. J Hum Genet 62:1023–1029
Lee JK, Hong YM, Jang GY et al (2015) Consortium-based genetic studies of Kawasaki disease in Korea: Korean Kawasaki Disease Genetics Consortium. Korean Circ J 45:443–448
Purcell S, Neale B, Todd-Brown K et al (2007) PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet 81:559–575
R Core Team (2016) R: a language and environment for statistical computing. R Foundation for Statistical Computing, Vienna
Matsumura T, Semba K, Azuma S et al (2004) TIFAB inhibits TIFA, TRAF-interacting protein with a forkhead-associated domain. Biochem Biophys Res Commun 317(1):230–234
Matsumura T, Kawamura-Tsuzuku J, Yamamoto T et al (2009) TRAF-interacting protein with a forkhead-associated domain B (TIFAB) is a negative regulator of the TRAF6-induced cellular functions. J Biochem 146:375–381
Varney ME, Niederkorn M, Konno H et al (2015) Loss of Tifab, a del(5q) MDS gene, alters hematopoiesis through derepression of Toll-like receptor-TRAF6 signaling. J Exp Med 212:1967–1985
Masuda M, Senju S, Fujii SI et al (2002) Identification and immunocytochemical analysis of DCNP1, a dendritic cell-associated nuclear protein. Biochem Biophys Res Commun 290:1022–1029
Suda K, Kishimoto S, Takahashi T et al (2013) Circulating myeloid dendritic cells is decreased in the acute phase of Kawasaki disease. J Clin Exp Cardiol 4:272
Westra HJ, Peters MJ, Esko T et al (2013) Systematic identification of trans eQTLs as putative drivers of known disease associations. Nat Genet 45:1238–1243
Acknowledgements
We thank all of our patients and their families for participating in this study. The following authors also participated in this study as members of the Korean Kawasaki Disease Genetics Consortium: In-Sook Park, Soo-Jong Hong, and Kwi-Joo Kim (Department of Pediatrics, Asan Medical Center, Seoul, Korea); Hyo-Kyoung Nam and Jung-Hye Byeon (Department of Pediatrics, Korea University Hospital, Seoul, Korea); Jung-Woo Rhim (Department of Pediatrics, The Catholic University of Korea, St. Mary’s Hospital, Daejeon, Korea); Dong Soo Kim (Department of Pediatrics, Yonsei University College of Medicine, Severance Children’s Hospital, Seoul, Korea); and Jae-Moo Lee and Jong-Duk Kim (Seoul Clinical Laboratories, Seoul, Korea). This study was supported by a Grant from the Ministry of Health and Welfare of the Republic of Korea (HI15C1575).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflict of interest to declare.
Additional information
Collaborators of the Korean Kawasaki Disease Genetics Consortium are listed in “Acknowledgements” section.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Kwon, YC., Kim, JJ., Yu, J.J. et al. Identification of the TIFAB Gene as a Susceptibility Locus for Coronary Artery Aneurysm in Patients with Kawasaki Disease. Pediatr Cardiol 40, 483–488 (2019). https://doi.org/10.1007/s00246-018-1992-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-018-1992-7