
Abstract
Atrioventricular nodal reentrant tachycardia (AVNRT), a common tachycardia in children, is routinely treated by catheter ablation using radiofrequency or cryothermal energy. Acute success rates of 95–97 % are reported for cryoablation, similar to those achieved with radiofrequency ablation (RFA). However, early studies reported higher recurrence rates after cryoablation for treatment of AVNRT than those reported for RFA. This study evaluated the success and recurrence rates for cryoablation in a current cohort of pediatric patients across several institutions. Patients 21 years old or younger with AVNRT who underwent cryoablation at five participating centers between 2004 and 2009 were retrospectively reviewed. Patient demographics and procedural data were extracted from patient records and analyzed. A total of 434 patients with AVNRT who underwent cryoablation were identified. Cryoablation was used as the exclusive ablation method for 379 patients. For 97 % (368/379) of these patients, cryoablation was acutely successful. A higher acute success rate was found with the 6-mm-tip catheter (99 %) than with the 4-mm-tip catheter (91 %) (p < 0.01). Recurrence was experienced by 7.3 % of the patients. Recurrence was more likely for those treated with the 4-mm-tip catheter (6/42, 14 %) than for those who had the larger catheters (12/204, 6 %) No patient experienced permanent heart block. Success and recurrence rates for this cohort of patients were similar to those reported for RFA used to treat AVNRT in pediatric patients. The findings show a higher success rate and a lower recurrence rate after cryoablation with a 6-mm-tip catheter than after use of the 4-mm-tip catheter, with an associated excellent safety profile.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Atrioventricular nodal reentrant tachycardia (AVNRT) is a common tachycardia in children [21]. The acute success rate for the treatment of AVNRT is 95–97 % when cryoablation is used [5, 6, 9, 10, 12, 23]. This rate is comparable with that reported for radiofrequency ablation (RFA) [6, 24].
In contrast to RFA, the catheter tip adheres to the myocardium during cryoablation, preventing migration of the catheter tip and possible damage to surrounding tissue (most importantly the atrioventricular node). Cryoablation is not associated with junctional ectopy, which allows monitoring of fast-pathway conduction [29]. It has a low propensity for thrombus formation [15] and is painless [4, 9].
Probably the most important advantage of cryoablation over RFA for the pediatric population is a decreased incidence of inadvertent permanent atrioventricular (AV) block during slow-pathway ablation [15, 19, 29]. To date, no case of permanent AV block complicating cryoablation in the treatment of AVNRT has been reported. Heart block continues to be reported for 1–3 % of the patients treated with RFA [13, 31]. Although rare, heart block has significant implications in an otherwise healthy child undergoing ablation of AVNRT, a non-life threatening arrhythmia, because it necessitates a lifetime of ventricular pacing.
It is suggested that the added safety associated with cryoablation comes at the cost of lower acute success rates and higher arrhythmia recurrence rates. The reported recurrence rates after cryoablation range from 5 to 14 % in various studies investigating children [5, 6, 12, 24] and adults [3, 9, 28]. This is higher than the 4–5 % rate reported for RFA in adult trials [9, 28]. With increased collective experience, a more common use of larger-tip cryoablation catheters, and more aggressive lesion applications, we hypothesized that the recurrence rates for AVNRT after cryoablation in children may approach those of patients treated with RFA. This decrease in the frequency of tachycardia recurrence after cryoablation has been demonstrated in adult patients with AVNRT [26, 28]. We therefore reviewed all cases of AVNRT in children treated with cryoablation at five pediatric cardiac centers in the United States over a recent 5-year period to determine acute success and recurrence rates and to evaluate predictors of recurrence.
Methods
We reviewed data from all patients with AVNRT 21 years old or younger at the time of cryoablation who presented for catheter ablation at five participating centers between 1 January 2004 and 31 December 2008. The study was approved by the institutional review boards of each institution. The participating centers were Children’s Healthcare of Atlanta, Emory University, Atlanta, Georgia; C.S. Mott Children’s Hospital, University of Michigan, Ann Arbor; Children’s Hospital, University of Iowa, Iowa City; Primary Children’s Medical Center, University of Utah, Salt Lake City; Children’s Heart Center, Las Vegas, Nevada.
Electrophysiology study records were reviewed to determine success or failure of the procedure, procedural complications, catheter size, and number of total lesions applied. All lesions treated 240 s or longer were designated as full lesions, whereas those terminated within the first minute were regarded as “freeze mapping” lesions. The first successful lesion, determined by the operator, was defined as a full lesion that terminated the AVNRT, eliminated inducibility of the AVNRT, or eliminated slow-pathway conduction.
Acute success was defined as either elimination of inducible tachycardia or slow-pathway conduction before the patient left the electrophysiology laboratory. A recurrence of AVNRT was defined by any of the following: suggestive clinical history; narrow complex tachycardia documented on electrocardiogram, Holter monitoring, event recorder, or repeat electrophysiology study.
Statistical analysis was performed using Stata 11.0 software. Descriptive data are presented as means ± standard deviations and percentages. Comparisons between groups (4- vs. 6- vs. 8-mm-tip and recurrence vs. no recurrence) were completed using Student’s t test or analysis of variance (ANOVA) for continuous variables and Fisher’s exact test for categorical variables. After univariate analysis, multivariable analysis was performed using a logistic regression model with selected variables. A p value less than 0.05 was considered statistically significant.
Results
The study population consisted of 434 children with AVNRT. The outcomes of the ablation procedures are summarized in Fig. 1. For 55 patients, both cryoablation and RFA were used. For 33 of these 55 patients, cryoablation was successful after RFA failure, or the operator switched to cryoablation due to a perceived increased risk with the use of RFA. All 55 cases were excluded from analysis of success or recurrence rates.

Study population profile. CA cryoablation, RFA radiofrequency ablation
During the follow up period, 246 of the 368 patients who underwent successful cryoablation had adequate follow-up assessment and were included in the analysis for arrhythmia recurrence. To be included, the patients needed to have documentation of a return visit to one of the clinics belonging to the included study centers. Because the five centers are referral centers for a large geographic area, many of the patients had clinical follow-up assessment at outlying sites and therefore were not included in the follow-up data set. Of the 246 individuals with available follow-up data after an initially successful cryoablation procedure, 18 had a recurrence of arrhythmia, giving a recurrence rate of 7.3 % over an average follow-up period of 24 months (Table 1). None of the patients in the study population experienced permanent first-, second-, or third-degree AV block.
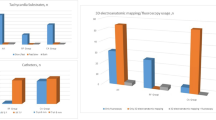
The ablation procedure characteristics of the study group are illustrated in Table 2. Cryoablation used as the exclusive ablation method was acutely successful for 97 % (368/379) of the patients. The 4-mm-tip catheter was used for only 18 % (70/379) of the study population and rarely during the latter part of the study because all the participating centers had changed from primarily using a 4-mm-tip catheter to using the 6-mm-tip catheter, and occasionally the 8-mm-tip catheter. The 8-mm-tip catheter also was used sparingly during the study period, although a bit more frequently toward the latter portion of the study. Nonetheless, when the patients treated with cryoablation alone were segregated into three groups based on catheter tip size (4, 6, or 8 mm), a significantly higher acute success rate was found with the 6-mm catheter tip (99 %) and 8-mm-tip (97 %) than with the 4-mm-tip (91 %) (Table 3) (p < 0.01).
The demographic and cryoablation features of the patients with and without AVNRT recurrence (18 recurrence cases; 228 no recurrence cases) who underwent cryoablation only are displayed in Table 4. The overall recurrence rate was 7.3 %. Recurrences were less frequent after ablation with a larger-tip catheter (12/204, 6 %) than after ablation with the 4-mm-tip catheter (6/42, 14 %; p = 0.017). Of the 12 recurrences after cryoablation with a larger-tip catheter, a 6-mm-tip was used in eight cases (8/178, 4.5 %), whereas an 8-mm-tip was used in four cases (4/26, 15 %). For four patients, a combination of 6- and 8-mm-tip catheters was used, and one of these patients had a recurrence.
To determine predictors for AVNRT recurrence, we performed logistic regression analysis using multiple variables. The results are summarized in Table 5. Using a catheter tip of 6 mm for cryoablation reduced the risk of recurrence by nearly 60 % (odds ratio 0.41; p = 0.002). Similarly, only a larger catheter tip was significantly predictive of acute success after cryoablation (odds ratio 3.0; p = 0.007).
Discussion
The largest study comparing the outcomes between RFA and cryoablation in adults with AVNRT has been published recently [9]. To date, our study is the largest report of cryoablation used to treat AVNRT in the pediatric population. The authors of the adult study [9] report that the acute success rates with both methods are similar. Similarly, we found that cryoablation is highly effective for the treatment of AVNRT in children, with an acute success rate equivalent to that reported for RFA in the current era (97 % in our study). Although we did not analyze our data on a year-to-year basis, our study period involved a time span with a trend toward the use of 6- or 8-mm-tip catheters [5, 16, 25, 26], application of “bonus” lesions [11], a freeze-thaw-freeze technique, and evaluation of sustained slow-pathway conduction suppression [8, 26] as the end point denoting better efficacy.
This study adds to the growing experience with the safety of cryoablation used for children. There were no cases of permanent AV block or any other serious complications such as cardiac perforation after cryoablation in the study population despite the smaller size of the children, the use of larger-tip catheters, and the application of several “insurance lesions” in most cases.
A novel finding of this study was the distinct advantage offered by a larger-tip catheter (6 mm) compared with the 4-mm-tip catheter in pediatric patients, with better success and lower recurrence rates. This observation has been made in the adult population [3, 7, 25], but pediatric experience has been limited to date [5].
Deisenhofer et al. [9] reported comparable acute success rates between cryoablation and RFA in their prospective trial using only the 6-mm-tip catheter and a bonus freeze at the successful site. An interesting observation in their study was the high number of device functionality failures in the cryoablation group (n = 18) compared with the RFA group (n = 2). Whether this had any impact on the success and procedure duration was not explained.
Our arrhythmia recurrence rate of 7.3 % after cryoablation over an average follow-up period of 2 years is lower than that reported in previous smaller studies and only marginally higher that those reported for RFA in adults [5, 6, 9, 11, 20, 23, 24]. Deisenhofer et al. [9] prospectively showed a lower recurrence rate with the 6-mm-tip cryoablation catheter than in their pilot study [32] a few years ago using the 4-mm-tip. Speculations as to the mechanisms for higher recurrence rates after cryoablation include a comparatively smaller lesion and absence of a large colliquation necrosis [30]. Our lower recurrence rate of 7.3 % compared with the 9.4 % observed in the landmark trial group of Deisenhofer et al. [9] may be partly related to a more aggressive approach among the investigators, which included the application of more lesions. In particular, the centers included in this study all delivered several “bonus” lesions surrounding the successful ablation site rather than a single “bonus” lesion. In fact, four of the five participating centers routinely used the EnSite NavX system (Endocardial Solutions, St. Jude Medical, Inc., St. Paul, MN, USA) for all cases and delivered one to five extra lesions guided by the successful mapped location.
In our study, the results with the 8-mm-tip catheter were worse than those achieved with the 6-mm-tip catheter in terms of arrhythmia recurrence. The reason for this difference is unclear. Use of the 8-mm-tip catheter may involve a learning curve. Because of the larger catheter size, operators may have limited the energy delivered (number of lesions) to the region of the slow-pathway and may have avoided a more anterior catheter position, thereby limiting efficacy and possibly increasing instances of recurrences. The selection of patients for use of the 8-mm-tip catheter also may have influenced the recurrence rate by limiting its use for more difficult cases. However, the number of patients analyzed who underwent ablation with the 8-mm-tip was too small for any significant conclusions to be drawn.
The risk of AV block, concerns for proarryhythmia, the possibility of lesion enlargement [18, 27], and thromboembolic events with RFA [1, 2, 15] make cryoablation a potentially safer option for treating AVNRT in children. These concerns are particularly important with the pediatric population because AVNRT is a condition that is relatively benign, whereas the consequences of inadvertent heart block at a young age are life changing.
Although transient adverse effects on AV conduction may be observed, we had no patients noted to have any permanent first-, second-, or third-degree heart blocks as a complication of the procedure. Such transient blocks have been reported, and we certainly observed that impingement on the conduction system was possible during cryoablation despite no evidence of such an effect during cryomapping. This may be explained by a larger cooling zone created during cryoablation relative to cryomapping which may impinge on the electrophysiological properties of adjacent structures [14]. Recently, cryothermal lesion expansion in immature infant swine myocardium has been demonstrated [17]. This serves as a cautionary note and calls for careful follow-up assessment, at least in the intermediate term, to ensure that no problems with AV conduction evolve.
Due to the retrospective nature of our study, which included five American pediatric centers, a uniform methodology was not available to enable analysis of its impact on success or recurrence rates. Also, different modes of mapping are used at these centers.
The choice between RFA and cryoablation was determined by the operator based on many factors including experience and equipment availability. In most of the centers included in this report, cryoablation is the default choice for catheter ablation of pediatric patients with AVNRT. These biases could not be excluded from our retrospective study.
This study also was limited by restricted data set variables available for analysis. Anecdotally, we noted a larger number of lesions during certain difficult cases that had recurrence. Enhanced safety with cryoablation may have influenced persisting endeavors from the operator in such cases. Full follow-up data were available for only 246 of 368 patients, which may have introduced bias into the results. It is likely, however, that those patients who had an arrhythmic recurrence would have been more likely to return for medical attention than those without recurrences. Therefore, the recurrence rate may be even lower than described in this report.
A further possible limitation of this retrospective study was that the 4-mm-tip catheter was used more frequently in the early portion of the study period. The possibility exists that the additional operator experience later in the study contributed to improved outcomes. A similar trend of improvement in efficiency with RFA was noted early after its introduction [22]. Our study results suggest that with more procedural experience, the efficacy and recurrence rates for cryoablation may mirror those of RFA.
Conclusion
In this largest review of cryoablation use with pediatric patients to treat AVNRT to date, the success and recurrence rates are similar to those for RFA use. A lower recurrence rate for AVNRT after cryoablation using a 6-mm-tip catheter was demonstrated as well as an associated excellent safety profile. This experience suggests that the 6-mm-tip catheter can be used safely and effectively in children.
References
Anfinsen OG, Gjesdal K, Brosstad F et al (1999) The activation of platelet function, coagulation, and fibrinolysis during radiofrequency catheter ablation in heparinized patients. J Cardiovasc Electrophysiol 10:503–512
Brueckmann M, Wolpert C, Bertsch T et al (2004) Markers of myocardial damage, tissue healing, and inflammation after radiofrequency catheter ablation of atrial tachyarrhythmias. J Cardiovasc Electrophysiol 15:686–691
Chan NY, Mok NS, Lau CL et al (2009) Treatment of atrioventricular nodal reentrant tachycardia by cryoablation with a 6-mm-tip catheter vs. radiofrequency ablation. Europace Eur Pacing Arrhythm Cardiac Electrophysiol 11:1065–1070
Chan NY, Choy CC, Lau CL et al (2011) Cryoablation versus radiofrequency ablation for atrioventricular nodal reentrant tachycardia: patient pain perception and operator stress. Pacing Clin Electrophysiol 34:2–7
Chanani NK, Chiesa NA, Dubin AM, Avasarala K, Van Hare GF, Collins KK (2008) Cryoablation for atrioventricular nodal reentrant tachycardia in young patients: predictors of recurrence. Pacing Clin Electrophysiol 31:1152–1159
Collins KK, Dubin AM, Chiesa NA, Avasarala K, Van Hare GF (2006) Cryoablation versus radiofrequency ablation for treatment of pediatric atrioventricular nodal reentrant tachycardia: initial experience with 4-mm cryocatheter. Heart Rhythm 3:564–570
De Sisti A, Tonet J, Barakett N, Lacotte J, Leclercq JF, Frank R (2007) Transvenous cryoablation of the slow pathway for the treatment of atrioventricular nodal reentrant tachycardia: a single-centre initial experience study. Europace Eur Pacing Arrhythm Cardiac Electrophysiol 9:401–406
De Sisti AD, Tonet J, Amara W et al (2011) Correlations between long-term results after cryoablation for atrioventricular nodal reentry tachycardia and a residual jump associated or not with a single echo. Europace Eur Pacing Arrhythm Cardiac Electrophysiol 14:261–266
Deisenhofer I, Zrenner B, Yin YH et al (2010) Cryoablation versus radiofrequency energy for the ablation of atrioventricular nodal reentrant tachycardia (the CYRANO study): results from a large multicenter prospective randomized trial. Circulation 122:2239–2245
Drago F, De Santis A, Grutter G, Silvetti MS (2005) Transvenous cryothermal catheter ablation of reentry circuit located near the atrioventricular junction in pediatric patients: efficacy, safety, and midterm follow-up. J Am Coll Cardiol 45:1096–1103
Drago F, Silvetti MS, De Santis A, Grutter G, Andrew P (2006) Lengthier cryoablation and a bonus cryoapplication is associated with improved efficacy for cryothermal catheter ablation of supraventricular tachycardias in children. J Interv Cardiac Electrophysiol 16:191–198
Drago F, Russo MS, Silvetti MS, DE Santis A, Iodice F, Naso Onofrio MT (2009) Cryoablation of typical atrioventricular nodal reentrant tachycardia in children: six years’ experience and follow-up in a single center. Pacing Clin Electrophysiol 33:475–481
Estner HL, Ndrepepa G, Dong J et al (2005) Acute and long-term results of slow-pathway ablation in patients with atrioventricular nodal reentrant tachycardia: an analysis of the predictive factors for arrhythmia recurrence. Pacing Clin Electrophysiol 28:102–110
Fischbach PS, Saarel EV, Dick M II (2004) Transient atrioventricular conduction block with cryoablation following normal cryomapping. Heart Rhythm 1:554–557
Khairy P, Chauvet P, Lehmann J et al (2003) Lower incidence of thrombus formation with cryoenergy versus radiofrequency catheter ablation. Circulation 107:2045–2050
Khairy P, Novak PG, Guerra PG et al (2007) Cryothermal slow pathway modification for atrioventricular nodal reentrant tachycardia. Europace Eur Pacing Arrhythm Cardiac Electrophysiol 9:909–914
Khairy P, Guerra PG, Rivard L et al (2011) Enlargement of catheter ablation lesions in infant hearts with cryothermal versus radiofrequency energy: an animal study. Circ Arrhythm Electrophysiol 4:211–217
Kimman GP, van Hemel NM, Jessurun ER et al (1999) Comparison of late results of surgical or radiofrequency catheter modification of the atrioventricular node for atrioventricular nodal reentrant tachycardia. Eur Heart J 20:527–534
Kimman GP, Theuns DA, Szili-Torok T, Scholten MF, Res JC, Jordaens LJ (2004) CRAVT: a prospective, randomized study comparing transvenous cryothermal and radiofrequency ablation in atrioventricular nodal reentrant tachycardia. Eur Heart J 25:2232–2237
Kirsh JA, Gross GJ, O’Connor S, Hamilton RM (2005) Transcatheter cryoablation of tachyarrhythmias in children: initial experience from an international registry. J Am Coll Cardiol 45:133–136
Ko JK, Deal BJ, Strasburger JF, Benson DW Jr (1992) Supraventricular tachycardia mechanisms and their age distribution in pediatric patients. Am J Cardiol 69:1028–1032
Kugler JD, Danford DA, Houston KA, Felix G (2002) Pediatric radiofrequency catheter ablation registry success, fluoroscopy time, and complication rate for supraventricular tachycardia: comparison of early and recent eras. J Cardiovasc Electrophysiol 13:336–341
Miyazaki A, Blaufox AD, Fairbrother DL, Saul JP (2005) Prolongation of the fast-pathway effective refractory period during cryoablation in children: a marker of slow-pathway modification. Heart Rhythm 2:1179–1185
Papez AL, Al-Ahdab M, Dick M II, Fischbach PS (2006) Transcatheter cryotherapy for the treatment of supraventricular tachyarrhythmias in children: a single-center experience. J Interv Cardiac Electrophysiol 15:191–196
Rivard L, Dubuc M, Guerra PG et al (2008) Cryoablation outcomes for AV nodal reentrant tachycardia comparing 4-mm versus 6-mm electrode-tip catheters. Heart Rhythm 5:230–234
Sandilands A, Boreham P, Pitts-Crick J, Cripps T (2008) Impact of cryoablation catheter size on success rates in the treatment of atrioventricular nodal reentry tachycardia in 160 patients with long-term follow-up. Europace Eur Pacing Arrhythm Cardiac Electrophysiol 10:683–686
Saul JP, Hulse JE, Papagiannis J, Van Praagh R, Walsh EP (1994) Late enlargement of radiofrequency lesions in infant lambs: implications for ablation procedures in small children. Circulation 90:492–499
Schwagten B, Knops P, Janse P et al (2011) Long-term follow-up after catheter ablation for atrioventricular nodal reentrant tachycardia: a comparison of cryothermal and radiofrequency energy in a large series of patients. J Interv Cardiac Electrophysiol 30:55–61
Skanes AC, Dubuc M, Klein GJ et al (2000) Cryothermal ablation of the slow pathway for the elimination of atrioventricular nodal reentrant tachycardia. Circulation 102:2856–2860
Skanes AC, Klein G, Krahn A, Yee R (2004) Cryoablation: potentials and pitfalls. J Cardiovasc Electrophysiol 15(10 Suppl):S28–S34
Van Hare GF, Javitz H, Carmelli D et al (2004) Prospective assessment after pediatric cardiac ablation: demographics, medical profiles, and initial outcomes. J Cardiovasc Electrophysiol 15:759–770
Zrenner B, Dong J, Schreieck J et al (2004) Transvenous cryoablation versus radiofrequency ablation of the slow pathway for the treatment of atrioventricular nodal reentrant tachycardia: a prospective randomized pilot study. Eur Heart J 25:2226–2231
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Das, S., Law, I.H., Von Bergen, N.H. et al. Cryoablation Therapy for Atrioventricular Nodal Reentrant Tachycardia in Children: A Multicenter Experience of Efficacy. Pediatr Cardiol 33, 1147–1153 (2012). https://doi.org/10.1007/s00246-012-0273-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-012-0273-0