
Abstract
This study was performed to determine the safety and efficacy of intravenous contrast echocardiography in children attending a tertiary cardiac center. This was a prospective study to evaluate the use of Optison contrast agent in children with severely limited transthoracic echocardiographic windows. Twenty children (median age, 15 years; range, 9–18) underwent fundamental imaging (FI), harmonic imaging (HI), and HI with intravenous contrast (Optison FS-069). Endocardial border delineation was determined based on a visual qualitative scoring system (0, none: 4, excellent). Endocardial border definition was significantly improved in all patients using contrast echocardiography (FI vs Optison, p < 0.001 for each). Improved border definition was most dramatic in the apical and left ventricular (LV) free wall regions. Left ventricular ejection fraction (LVEF) was measurable in 20 patients (100%) using contrast compared to 11 (55%) with FI or HI (p < 0.05). The echocardiographic diagnosis was correctly delineated in 1 patient with a severely dyskinetic LV segment only with use of intravenous contrast and HI. No patients suffered adverse hemodynamic effects, changes in taste, or flushing episodes. Three patients experienced transient headaches. Intravenous contrast echocardiography offers an additional tool in evaluating children with very poor transthoracic echocardiographic windows. Such a strategy increases diagnostic accuracy and allows accurate LVEF determination. Adverse hemodynamic effects related to intravenous contrast are exceedingly rare.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Intravenous contrast echocardiography has been demonstrated to be a useful tool in optimizing endocardial border delineation in the adult population [1, 2, 3, 8]. However, there is limited experience with contrast agents in children [9]. Although limited echocardiographic windows are a common challenge in adults, there is a similar subset of children who also have very poor echocardiographic windows secondary to obesity, chest wall deformities, or prior surgical intervention [6]. Although the potential benefits from a visualization standpoint are unequivocal using intravenous contrast, concerns regarding possible side effects related to the intravenous contrast agents and whether use of such agents improves cardiac function evaluation in children remain to be addressed.
This study sought to (1) determine the side effect profile of FS-069 Optison (Mallinckrodt, St Louis, MO, USA) in the pediatric population and (2) assess whether the combined use of intravenous contrast agents and harmonic imaging (HI) could improve the evaluation of cardiac function over fundamental imaging (FI) or HI alone.
Materials and Methods
Between January 2000 and July 2002, pediatric patients with limited transthoracic echocardiographic windows with suboptimal endocardial definition were recruited to participate in the study. Informed consent was obtained from the child's parent or guardian prior to the study. Patients with intracardiac shunts were excluded from the study following recommendations of the Food and Drug Administration (provided on the product label). The study was approved by the institutional review board of Baylor College of Medicine.
Echocardiographic Analysis
Equipment settings were standardized as follows: (1) low mechanical index (MI), (2) transmit focus at the level of the mitral valve, and (3) time gain control and overall gain were decreased. Imaging of the parasternal short- and long-axis, apical four-chamber, and subcostal views was performed initially with FI and then with HI. The left ventricle (LV) was divided into three sections (from basal to mid to apical regions) for specific evaluation of endocardial border definition (Fig. 1). A qualitative score was given to each ventricular segment. Scores were graded as 0 where there was no visualization of the LV endocardial border, 1 where poor, 2 where fair, 3 where good, and 4 where there was excellent visualization. Intra- and interobserver variability was determined for each of the views.

Apical four-chamber view comparing (A) functional imaging, (B) harmonic imaging (HI), and (c) HI with contrast echocardiography in a patient with a dyskinetic left ventricular segment.
Optison Administration
We administered two doses of Optison during the study protocol. In children weighing less than 20 kg, 0.3 cc of contrast was administered with each dose, and in children greater than 20 kg, 0.5 cc of contrast was administered with each dose. A bolus of contrast, at a steady rate of approximately 1 cc per second, was injected through a peripheral intravenous line in the hand or antecubital vein and immediately flushed with isotonic saline. The MI was lowered to 0.2–0.3 at the time of Optison administration to avoid contrast fragmentation. During administration and the following 30 minutes after administration of the contrast agent, vital signs including blood pressure, heart rate, and oxygen saturation were closely monitored. Patients were assessed and questioned as to the presence of symptoms including a sensation of flushing, metallic taste, skin rashes, or nausea.
Data Analysis
Differences in scoring between imaging modalities for each of the LV wall segments was compared using analysis of variance. Data are expressed as mean and range. A p value <0.05 was taken as statistically significant.
Results
Twenty patients (8 female) with a median age of 15 years (range, 9–18) were included in the study. Diagnoses are listed in Table 1. No cases of intracardiac shunting were documented with contrast administration. No changes in heart rate, blood pressure, or pulse oximetry occurred during or after administration of contrast. Additionally, no arrhythmias were noted during the study protocol. There were no reports of subjective flushing or nausea. Three patients developed transient headaches, each lasting less than 15 minutes, all of which occurred within 30 minutes of contrast administration. One patient reported a transient change in taste sensation for a brief period of time.
Image Improvement
There was a dramatic improvement in endocardial border definition in all myocardial wall segments with the concomitant use of intravenous contrast and HI (Table 2). The improvement in border delineation was further augmented by a second administration of intravenous contrast for each segment. The most dramatic improvements were in the apical segments and LV free wall in 18 of the 20 patients (90%). Left ventricular ejection fraction (LVEF) could not be calculated from the standard transthoracic echocardiograms in 9 patients (45%). In the 11 patients in whom LVEF was measurable, interobserver variability was high (16%), with a median LVEF of 38%. Calculation of LVEF was possible in all patients when HI was combined with contrast echocardiography. More importantly, LVEF was erroneously undermeasured with FI alone compared to use of HI and contrast together (38 vs 57% for FI and HI with Optison contrast, respectively). There was a significant reduction in interobserver variability (4%) using HI with contrast echocardiography versus FI or HI alone (10%, p < 0.05). Of note, 1 patient was diagnosed with a markedly dyskinetic LV segment by contrast echocardiography not apparent by FI or HI alone (Fig. 2). Using the aforementioned dose of contrast agent, the median LV opacification time was 1 minute 54 seconds, allowing multiple serial LVEF measurements.

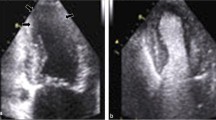
Comparison of HI and HI with Optison in a patient with dyskinetic apial LV segment.
Discussion
This study demonstrates the safety of using contrast echocardiography in children with limited transthoracic echocardiographic windows. Equally important, it demonstrates the improved delineation and diagnostic accuracy of LVEF measurements using intravenous contrast echocardiography with HI versus FI or HI alone. This study also corroborates data from several adult studies and one pediatric study indicating that Optison contrast significantly improves LV cavity and endocardial border visualization [5, 6, 9]. Similar to previously reported series, endocardial border definition was most significantly improved in the apical and LV free walls [7, 9].
Multiple contrast agents have been studied, including agitated saline, albunex (Mallinckrdot, St. Louis, MO, USA), and Optison. Optison, a second-generation agent produced by sonification of albumin with octofluoropropane, is advantageous compared to the other available products due to its prolonged duration of action allowing repeated evaluation of ventricular function as well as more definitive anatomical assessment [2]. Although there were initial concerns regarding the safety of intravenous contrast agents, several studies, including one pediatric study, reported a low incidence of adverse hemodynamic or systemic complications [1, 2, 3, 8, 9]. However, one animal study did demonstrate altered myocardial permeability, premature ventricular contractions, and petechial hemorrhages within the myocardium of rats, particularly with increasing Optison dosage in the range 25–500 μl/kg [4].
In our experience, apical views are preferable for the detailed evaluation of different left ventricular segments because parasternal views may be significantly affected by attenuation artifacts generated by the presence of contrast in the right ventricle. Attenuation artifacts were present in many of our patients during contrast evaluation including the apical views but dissipated within a few cardiac cycles.
Complications
The only significant complication in our study cohort was transient headaches, temporarily related to contrast administration. A previous pediatric study reported similar findings with no significant adverse hemodynamic consequences to intravenous contrast administration [1]. Minor side effects in our study included a single patient with altered taste sensation for a short period of time. Side effects in adult studies are significantly more prevalent, most likely secondary to higher infused volumes of contrast agent. One study of 279 adult patients using doses as high as 44 cc reported side effects in 16.8% of patients, including headache (5.4%), nausea/vomiting (4.3%), flushing (3.6%), and dizziness (2.5%) [2]. Use of low doses in the pediatric population has been proven in this study to be safe and to allow excellent anatomic and functional assessment.
Conclusions
This study provides further evidence that the use of intravenous contrast agents is safe, improves accuracy of evaluation of cardiac function, and helps to better delineate the endocardial borders of specific segments in children. Given the ever-increasing demand for acquisition of high-quality echocardiographic data in cardiac units, Optison contrast echocardiography represents a useful noninvasive diagnostic tool in obtaining an accurate evaluation in terms of anatomic and functional assessment. Adverse hemodynamic disturbances following contrast administration are exceedingly rare.
References
A Candido J Coucelo J Galvao et al. (2003) ArticleTitleContrast echocardiography in segmental analysis and intraventricular gradient quantification in hypertrophic cardiomyopathy Rev Port Cardiol 22 789–798 Occurrence Handle14526696
UN Clark HC Dittrich (2000) ArticleTitleCardiac imaging using Optison Am J Cardiol 86 14G–18G Occurrence Handle10997346 Occurrence Handle10.1016/S0002-9149(00)00984-X Occurrence Handle1:CAS:528:DC%2BD3cXlvV2kurc%3D
M Kornblith DH Liang P Brown et al. (2000) ArticleTitleContrast echocardiography is superior to tissue harmonics for assessment of left ventricular function in mechanically ventilated patients Am Heart J 140 291–296
P Li L Cao CY Dou et al. (2003) ArticleTitleImpact of myocardial contrast echocardiography on vascular permeability: an in vivo dose response study of delivery mode, pressure amplitude and contrast dose Ultrasound Med 29 1341–1349
V Malhotra J Nwogu MD Bondmass et al. (2000) ArticleTitleIs the technically limited echocardiographic study an endangered species: endocardial border definition with native tissue harmonic imaging and Optison contrast; a review of 200 cases J Am Soc Echocardiogr 13 771–773 Occurrence Handle10936821 Occurrence Handle1:STN:280:DC%2BD3cvotVeltA%3D%3D
CJ McMahon K Fraley JP Kovalchin (2001) ArticleTitleUse of tissue harmonic imaging in pediatric echocardiography Cardiol Young 11 562–564 Occurrence Handle11727915 Occurrence Handle1:STN:280:DC%2BD3MnotFCgtw%3D%3D
TR Porter F Xie A Kricsfeld et al. (1994) ArticleTitleImproved endocardial border resolution during dobutamine stress echocardiography with intravenous sonificated dextrose albumin J Am Coll Cardiol 10 45–51
JW Verjans N Narula A Loyd et al. (2003) ArticleTitleMyocardial contrast echocardiography in acute myocardial infarction Curr Opin Cardiol 18 346–350 Occurrence Handle12960465
MV Zilberman SA Witt TR Kimball (2003) ArticleTitleIs there a role for intravenous transpulmonary contrast imaging in pediatric stress echocardiography? J Am Soc Echocardiogr 16 9–14 Occurrence Handle12514629
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
McMahon, C., Ayres, N., Bezold, L. et al. Safety and Efficacy of Intravenous Contrast Imaging in Pediatric Echocardiography. Pediatr Cardiol 26, 413–417 (2005). https://doi.org/10.1007/s00246-004-0795-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00246-004-0795-1