
Abstract
The in vitro study of calcium oxalate (CaOx) stone formation is usually based on crystallisation models but it is recognised that both healthy individuals and stone formers have crystalluria. We have established a robust in vitro stone growth model based on the principle of mixed suspension, mixed product removal system (MSMPR). Utilising this technique we studied the influence of CaOx crystallisation kinetics and the variation of calcium and oxalate concentrations on CaOx stone growth in vitro. Six stones received standard concentration of Ca (6 mM) and Ox (1.2 mM) in the medium while another six received variable concentrations of both Ca and Ox at various intervals. Stone mass was plotted against the experiment duration (typically 5–7 weeks). The stone growth was dependent on sufficient input calcium and oxalate concentrations and once triggered, stone growth could not be maintained at reduced calcium and oxalate inputs. The stone growth rate was positively correlated to the number of crystals in suspension around the stone and to the crystal nucleation rate and negatively correlated to the crystal growth rates. This leads to the conclusion that aggregation of crystals from the surrounding suspension was the dominant mechanism for stone enlargement.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Current understanding of renal stone formation is mainly based on the study of crystallisation in simple salt solutions, urine-like media or urine itself. While crystals are the building blocks for stones, the pathophysiological process of microscopic crystals transforming into macroscopic stones remain unclear; nor is it inevitable, as it is well recognised that crystalluria occurs commonly in healthy subjects [1]. The “stone farm”, an in vitro stone growth model that was developed in our laboratory operates on the principle of equilibrium supersaturation which is dynamically similar to the kidney [2–4]. This allows us to study the relation between the solution composition, the crystal suspension and stone enlargement.
At first sight, it might seem self evident that higher input supersaturation, through increased calcium and/or oxalate concentrations being fed into the system, should lead to increased stone growth. The opposite, however, might occur if the increased supersaturation causes an increase in nucleation of new crystals, which in turn would result in the solution supersaturation being lowered and the potential for crystal growth at the stone surface diminishing. If this mechanism were to operate, then stone enlargement might proceed efficiently at relatively low input calcium and oxalate concentrations and this might explain the in vivo “triggering” experiments of Vermeulen [5], where a high initial dose of stone salts allowed embryonic stones to form and these continued to grow in a low stone salt environment. An aim of the studies reported here is to try to replicate this behaviour in an in vitro system. Another objective is to obtain quantitative data pertaining to another conundrum about stone growth: does it occur primarily through crystal growth at the surface or through aggregation of suspended crystals?
Materials and methods
The study was conducted with the in vitro stone farm method described by Chow et al. [3, 4]. This is based on MSMPR continuous crystallisation. By allowing continuous flow through the crystallisation chamber, this system is able to establish an equilibrium supersaturation, which is dynamically similar to the renal system [6]. The stone farm consists of six pairs of individually jacketed crystallisation chambers containing a fragment of core material suspended in each chamber. The pairs of chambers were set up in parallel, the first of each pair received two feed solutions at a total flow rate of 1 L/day. The output of the first chambers was used as the feed for the second. Six pair of chambers received control artificial urine (AU) as feed solutions while the remaining six received modified AU in terms of the calcium and oxalate concentrations.
Flow rates were checked daily by the change of weight of the feed solutions over time. The solutions within each chamber were continuously stirred and the temperature controlled at 37°C. The volume of solution of each chamber was set at 20 ml. Every 24 h the stones were removed and the system cleaned with 0.1 M HCL. Stones were weighed about every 48 h, and ion-selective electrodes measured the pH and ionized calcium of each individual chamber regularly. The stones were grown for periods of between 5 and 7 weeks.
Artificial urine
Artificial urine used was prepared according to the standard values used by Chow et al. [3]. The AU in one feed solution contained calcium while the other oxalate. Feed solution I was made up of 12 mM CaCl2, 6 mM MgCl2 and 4 mM K3citrate. Feed solution II contained 300 mM NaCl, 151 mM KCl, 40.4 mM (NH4)2SO4, 10.2 mM Na2HPO4, 38.8 mM NaH2PO4 and 2.4 mM Na2Ox. Each feed solution was fed in at the same flow rate (0.35 ml/min), giving a mixture with a pH of 6.0. A number of procedures were adopted to try to prevent any microbial contamination [3] and no evidence of any such contamination (e.g. deviation of pH from about 6.0) was observed.
Stone core
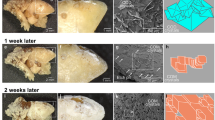
Previously we have used residual CaOx stone fragments as the stone nidus for the study of CaOx stone growth in vitro [2–4] but this has some shortcomings. The amount of residual fragments that is suitable for stone farm experiments is limited and this poses the difficulty of standardising all fragments used in the experiments. Ideally we would use fragments with the same mass, surface area, and composition but this is difficult to achieve with natural stone material. Marble chips (calcium carbonate) were used for the experiments performed in this study. They address most of the disadvantages faced by CaOx stone fragments. Their usage allows not only the proper standardisation of fragments but also the source they are derived from. The initial deposition upon the marble chips appears as readily as with natural stone fragments and, as might be expected, once this first layer has been completed the subsequent product is indistinguishable from material grown around natural stones. In particular, the growth rates with marble chips are comparable to those obtained with natural fragment but the inter- and intra-experimental variation of controls stones is much improved [7].
Protocols
In each experiment, a total of 12 stones were grown in the stone farm. Six stones acted as controls receiving 6 mM calcium (Ca) and 1.2 mM oxalate (Ox) in the standard media while the remaining stones received different concentrations of either one or both calcium and oxalate at various intervals. Stone growth was measured by periodic weighing and growth rates calculated assuming a surface area-dependent model [2, 7]. Towards the end of each daily growth period the equilibrium crystal size distribution was measured twice in the surrounding suspension of each stone using a Coulter counter (Coulter Multisizer II, Beckmann). The crystal nucleation and growth rates were calculated from the crystal size distribution, using the principles of MSMPR [8].
Results
Pulses of high and low calcium and oxalate concentrations
This experiment was intended to determine whether stone growth, once initiated, could be maintained by a lower dose of calcium and oxalate, in a manner comparable to in vivo experiments by Vermeulen [5]. With 50% of the standard calcium and oxalate concentration, growth was minimal. Increasing both calcium and oxalate to the standard condition caused the stones to grow appreciably. Returning the calcium and oxalate in the input media to 50% reduced growth back to a minimal rate (Fig. 1; Table 1). Because the growth rates in Table 1 are calculated with only 4–6 data points they do not have a very high degree of confidence. The lower panel of Fig. 1 shows that, although the rate estimates for the individual segment vary, when the growth is very slow they cannot really be distinguished.

Stone growth (mean ± s.e., n = 6) in AU with Ca and Ox at standard concentrations (6 and 1.2 mM respectively, solid circles) or reduced by half (open circles). Upper panel: the upper series A of five curves are relate to the same six stones while the lower series B of two curves correspond to the other six stones grown at the same time. Lower panel: an enlargement of the first section of series B. The heavy solid and dashed lines are the best fit curves to the four time sections shown in Table 1. The lighter solid line is the best fit curve to all the data shown
Variable calcium concentration
Rapid stone growth was obtained in the presence of 5 mM or more while 3 and 4 mM of Ca produced only minimal stone growth (Fig. 2).

Changes in mean stone mass (±s.e., n = 6) at variable calcium concentrations. The input oxalate concentration was 1.2 mM throughout. The lines through the data are fitted to the surface area-dependent model, used to estimate the growth rate, k (103 × mg/h3/2)
The relationship between suspension crystallisation kinetics and stone growth
Through 26 experimental growth periods, the stone growth rate was correlated to the crystal nucleation rate and the number of crystals in suspension around the stone. There was an inverse relationship between stone growth rate and crystal growth rate. Similarly, the nucleation rate was correlated to the particle density and inversely related to the crystal growth rate (Table 2). Multiple linear regressions showed that only the nucleation rate was an independent and significant predictor of stone growth.
Discussion
Vermeulen [5], summarising a series of in vivo experiments with different animals and stone forming protocols, concluded that a brief but high level of supersaturation was sufficient for a stone embryo to form while further stone growth could be sustained at a lower level of supersaturation. Similar results for in vivo production of nephrocalcinosis have also been recently published [9]. Figure 1 shows an attempt to replicate these findings in vitro. We used 6 mM Ca and 1.2 mM Ox as the “trigger” dose since these concentrations are known to promote stone growth in previous experiments [2, 3] while the “maintenance” dose was 50% of the concentrations of the “trigger” dose. An initial period of maintenance dose, with negligible stone growth, was followed by a period of triggering dose for half the stones. This resulted in the consistent growth that we regularly find under these conditions [7]. Reverting back to the maintenance dose caused the growth rate to fall back to the same level as the control stones that had not received a triggering dose. This pattern was repeatable and we found no evidence to suggest that the growth in the maintenance dose could be enhanced by a period of triggered growth. Vermeulen [5] used a maintenance dose, which was 25% of the triggering dose, so although the concentrations in the vitro and in vivo models are not directly comparable, it is likely that had the same effect been achievable in our system then our maintenance dose would have been sufficient to demonstrate this. The disparity in outcomes might be associated with the absence of biological factors in our model. Future work involving the inclusion of whole urine or UMM might help to clarify this issue.
Irrespective of the rate of stone growth, or whether it is in an initial or maturing phase, there are two fundamentally different mechanisms of enlargement possible. A stone could enlarge either by aggregation of crystals from the suspension or by direct precipitation onto the stone surface (onto secondary nuclei or mature crystals), or both [10]. These possible routes were investigated by examination of the relationship between stone growth and the quantitative analysis of crystal sizes and numbers surrounding the growing stone. In our earlier MSMPR studies [8] we demonstrated that there were systematic changes in the crystal size suspension in correspondence to changes in the input concentrations of the AU. Thus, by varying the calcium and oxalate concentrations we have been able to produce different suspension conditions and different rates of stone growth. An example of the latter is shown in Fig. 2, where the stone growth rate is demonstrated to increase with increasing calcium concentrations. From these and other experiments we found a significant correlation between stone growth rate and crystal nucleation rate which in turn is positively correlated to the crystal density and negatively related to the crystal growth rate.
If the direct precipitation mechanism is the more important process then stone enlargement would be expected to be greatest when the solution supersaturation is high in order to support new crystal growth on the stone surface. On the other hand, if the aggregation mechanism is more important then stone enlargement would be expected to be greatest when the particle numbers in suspension are high, because this would increase the likelihood of collisions between the stone and the surrounding crystals. Figure 3 illustrates these two scenarios and highlights our results, which are consistent with the aggregation model as the dominant mechanism of stone growth in the stone farm.

Illustration of two scenarios of crystal size distribution (suspended crystals) and the expected outcome of stone enlargement based primarily on aggregation (A) or crystal growth (CG). The correlations we observed (Table 2) are consistent with the aggregation mechanism
Calcium oxalate renal stones are complex structures. Different types can be recognised and within individual stones there is much internal heterogeneity. The crystals may be individually coated in matrix or groups of crystals may be located within matrix bound regions. Adjacent crystals may be randomly orientated, or ordered in sheet or stack like structures [11–14]. Individual crystals are typically in the “micro” rather than “nano” size range, although they may be built up of smaller crystallites [15, 16] perhaps by a process corresponding to mesoscopic transformation [17]. Although stones are undoubtedly polycrystalline aggregates it does not necessarily follow that each crystal aggregated into the bulk of the stone mass in its mature “micro” form. (This would probably involve a small degree of local recrystallisation in order to form a consolidated structure [18, 19]). Alternatives would be for “nano” nuclei (from a primary or secondary nucleation event) to become associated with the stone and there to enlarge by classical crystal growth (ion attachment and unit cell replication) or for multiple nuclei to assembly as a mesocrystal [17]. When discussing stone architecture, others have interpreted the structural information in terms of “micro” crystals aggregating to the surface [12] or to local solution chemistry and precipitation [14, 20] or both [21]. The significance of the distinction perhaps lies in understanding the role of intratubular crystals. If, as is widely believed to be possible [22, 23], crystals form in the collecting ducts and pass freely beyond the ducts of Bellini, can they then contribute to stone development? Our results appear to give quantitative evidence that this is possible and, as this happened in AU, the presence of matrix macromolecules is not a prerequisite for the process. Of course, in vitro evidence that crystal aggregation can occur at the macro-scale of real stones is not proof that it takes place in vivo, but it does suggest that crystalluria itself will directly enhance the process of new stone formation or re-growth of residual fragments.
References
Kavanagh JP (2001) A critical appraisal of the hypothesis that urine is a saturated equilibrium with respect to stone-forming calcium salts. BJU Int 87:589–598
Ananth K, Kavanagh JP, Walton RC, Rao PN (2002) Enlargement of calcium oxalate stones to clinically significant size in an in-vitro stone generator. BJU Int 90:939–944
Chow K, Dixon J, Gilpin S, Kavanagh JP, Rao PN (2004) A stone farm: development of a method for simultaneous production of multiple calcium oxalate stones in vitro. Urol Res 32:55–60
Chow K, Dixon J, Gilpin S, Kavanagh JP, Rao PN (2004) Citrate inhibits growth of residual fragments in an in vitro model of calcium oxalate renal stones. Kidney Int 65:1724–1730
Vermeulen CW (1972) Calculogenesis and stone triggering. National Academy of Sciences, Washington
Finlayson B (1972) The concept of a continuous crystalliser. Its theory and application to in vivo and in vitro urinary tract models. Invest Urol 9:258–263
Kavanagh JP, Rao PN (2007) Lessons from a stone farm. AIP Conf Proc 900:159–169
Kavanagh JP, Jones L, Rao PN (1999) Calcium oxalate crystallization kinetics at different concentrations of human and artificial urine, with a constant calcium to oxalate ratio. Urol Res 27:231–237
Marengo S, Zhang A (2007) It pays to read the old dead guy’s papers:triggering doses of oxalate and calcium oxalte nephrocalcinosis. AIP Conf Proc 900:398–401
Kavanagh JP (1999) Enlargement of a lower pole calcium oxalate stone: A theoretical examination of the role of crystal nucleation, growth, and aggregation. J Endourol 13:605–610
Grases F, Costa-Bauza A, Garcia-Ferragut L (1998) Biopathological crystallization: a general view about the mechanisms of renal stone formation. Adv Colloid Interface Sci 74:169–194
Khan SR, Hackett RL (1993) Role of organic matrix in urinary stone formation—an ultrastructural-study of crystal matrix interface of calcium-oxalate monohydrate stones. J Urol 150:239–245
Daudon M, Bader CA, Jungers P (1993) Urinary calculi—review of classification methods and correlations with etiology. Scanning Microsc 7:1081–1106
Millan A (1997) Crystal morphology and texture in calcium oxalate monohydrate renal calculi. J Mater Sci Mater Med 8:247–250
Webber D, Chauvet MC, Ryall RL (2005) Proteolysis and partial dissolution of calcium oxalate: a comparative, morphological study of urinary crystals from black and white subjects. Urol Res 33:273–284
Fleming DE, Van Riessen A, Chauvet MC, Grover PK, Hunter B, Van Bronswijk W, Ryall RL (2003) Intracrystalline proteins and urolithiasis: a synchrotron X-ray diffraction study of calcium oxalate monohydrate. J Bone Miner Res 18:1282–1291
Niederberger M, Colfen H (2006) Oriented attachment and mesocrystals: Non-classical crystallization mechanisms based on nanoparticle assembly. Phy Chem Chem Phy 8:3271–3287
Hounslow MJ, Mumtaz HS, Collier AP, Barrick JP, Bramley AS (2001) A micro-mechanical model for the rate of aggregation during precipitation from solution. Chem Eng Sci 56:2543–2552
David R, Espitalier F, Cameirao A, Rouleau L (2001) Developments in the understanding and modeling of the agglomeration of suspended crystals in crystallization from solution. KONA 21:40–53
Sokol E, Nigmatulina E, Maksimova N, Chiglintsev A (2005) CaC2O4.H2O spherulites in human kidney stones: morphology, chemical composition, and growth regime. Eur J Mineral 17:285–295
Grases F, Costa-Bauza A, Ramis M, Montesinos V, Conte A (2002) Simple classification of renal calculi closely related to their micromorphology and etiology. Clin Chim Acta 322:29–36
Finlayson B, Reid F (1978) Expectation of free and fixed particles in urinary stone disease. Invest Urol 15:442–448
Kok DJ, Khan SR (1994) Calcium-oxalate nephrolithiasis, a free or fixed particle disease. Kidney Int 46:847–854
Acknowledgments
These studies were funded by Kidney Research UK and The Oxalosis and Hyperoxaluria Foundation. We also thank S. Gilpin and J. Dixon for their technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Saw, N.K., Rao, P.N. & Kavanagh, J.P. A nidus, crystalluria and aggregation: key ingredients for stone enlargement. Urol Res 36, 11–15 (2008). https://doi.org/10.1007/s00240-007-0121-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-007-0121-5