
Abstract
Background
Our goal was to obtain nasal bone and nasal pyramid morphometric measurements in Caucasian skulls and analyze variation in different age groups and gender.
Methods
Ninety caucasian skulls were grouped according to three age groups: group I (20–40), II (41–64), and III (>65). The basion (B)-nasion (N), B-anterior nasal spine (ANS), B-supradentale (SD), N-ANS, ANS-SD, and length and width of each nasal bone, height, width, and angle of the pyriform aperture were measured. Comparisons were done between age groups, males and females, between left/right sides.
Results
The distance between B-N, B-ANS, and B-SD was greater when group I was compared with group II and III in both genders with the exception that the B-N distance in male population was slightly (0.2 mm) longer in group I. There was a statistically significant directly proportional relationship between B-N and B-ANS (p < 0.001, rho 0.54), B-N and B-SD (p = 0.001, rho 0.34), and B-ANS and B-SD (p < 0.001, rho 0.90) distances in all skulls independent of age and gender. The mean nasal bone lengths were; nasal bone length at midline (F: 20.07/19.67/21.20 mm, M:23.07/22.33/23.13 mm in groups I/II/III, respectively), at lateral suture lines (F:23.9/24.93/24.33 mm, M: 27.03/26.95/27.93 mm in groups I/II/III, respectively).
Conclusion
This study not only supports the existing literature that the midface and the nasal skeleton show variation with age and gender but also adds valuable information about the nasal bone and related parameters. Nasal and midfacial surgeries should be done with particular attention to different morphology in different age and gender groups in order to provide the patient with an improved physiologic and normal result.
Level of Evidence: not ratable.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Aesthetic and functional nasal surgeries, together with nasal reconstructive procedures are widely performed plastic surgery procedures worldwide. A solid knowledge of pertinent anatomy is vital to successfully restore or modify nasal and midface features. Age-related changes of the nasal skeleton and nasal pyramid structures and their impact on facial appearance have been analyzed in few studies [1, 2]. Also, cadaver studies and measurements on three-dimensional computerized tomography (3D-CT) were done by a group of researchers that analyzed dimensions of nasal bone and nasal pyramid structures in different races [3–7]. However, the literature is devoid of detailed studies about morphology of the nasal bones and the midface in equally distributed age and gender groups.
Understanding the variation of nasal skeletal characteristics in different age and gender groups can potentially improve outcomes of nasal surgeries and midface rejuvenation procedures [8]. The goal of this study was to obtain nasal bone and midface measurements in different age groups, divided by gender, and to analyze the relation of these parameters in respect to each other.
Materials and methods
Ninety caucasian skull specimens were acquired from Cleveland Natural History Museum, Cleveland, Ohio, USA, and were used for morphometric analysis. The skulls were taken from the unclaimed dead of Cleveland, OH, and Cuyahoga County, OH, USA, between 1912 and 1938. They were macerated using live steam and boiling water. Once the maceration process was complete, the skulls were cleaned with brushes to remove the remnants of the soft tissue and dried. The skulls were then labeled and stored based on age, gender, and race. The specimens were randomly chosen according to three age groups: group I–young age (20–40 years old), group II–middle age (41–64 years old) and group III—old age (>65 years old). Each group consisted of 15 male and 15 female skulls. Skull specimens that were edentulous and lacked dental support were excluded from analysis as well as those with obvious fractures and other anomalies. The skulls with sagittal or coronal cuts for internal inspection were included as long as the landmarks were intact for measurement.
The following landmarks were measured: (1) basion–nasion (B-N), (2) basion-anterior nasal spine (B-ANS), (3) basion–supradentale (B-SD), (4) nasion–anterior nasal spine (N-ANS), (5) anterior nasal spine–supradentale (ANS-SD), (6) length of nasal bones, (7) width of nasal bones, (8) height of pyriform aperture, (9) width of pyriform aperture, and (10) angle between paired nasal bones and pyriform aperture (pyriform aperture angle; PAA) (Figs. 1, 2, and 3). The width of nasal bones was measured along proximal and distal edges and the length was measured along the lateral suture lines and along the midline between the paired nasal bones. The height of the pyriform aperture was measured between the distal edge of the nasal midline and ANS while the width was measured at the widest part (Fig. 3).

The following landmarks were measured: (1) basion–nasion (B-N), (2) basion-anterior nasal spine (B-ANS), (3) basion–supradentale (B-SD)

The following landmarks were measured: (4) nasion–anterior nasal spine (N-ANS), (5) anterior nasal spine–supradentale (ANS-SD)

The height of the pyriform aperture was measured between the distal edge of the nasal midline and ANS while the width was measured at the widest part
Measurements were done utilizing a portable, high-precision measurement tool, the MicroScribe® (Revware Systems, Inc., Raleigh, NC, USA) that calculates the distance between two points in a 3D space with high accuracy of up to 0.23 mm, a ruler and a protractor for measuring angle. To minimize inter-observer and intra-observer error, the skulls were immobilized on a measuring table and all measurements were done by the same author (CO) while two other authors (CNO, SU) confirmed and entered the data on site. Additionally, the data collection was completed within a short period of time as recommended to avoid intra-observer errors.
The analysis of data was done by overall means and Bonferroni corrected pairwise comparisons for the three age groups, by gender. Additionally, correlations between the specific measurements (B-ANS vs. B-N, B-ANS vs. B-SD, B-N vs. B-SD, and apertura height vs. aperture width) and symmetry comparisons of nasal bones were done for both genders. For each of these analyses, an overall p value that is significant (p < 0.05) states that there is a relationship between three age groups and the skull measurement. For pairwise differences in three group comparisons, significance was p < 0.0167 based on Bonferroni correction for three possible pairs. Finally, the symmetry comparisons of left and right nasal bones, and relationship between specific measurements that is not related with age and gender, were done using correlation analyses that range from −1 to +1 with 0 being no relationship, and +1 being the strongest relationship. A positive correlation means that there is a direct relationship (as one parameter increases the other one increases as well). A negative correlation means these two parameters are inversely related.
Results
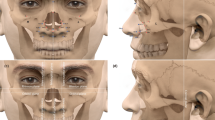
The mean age of female (F) specimens was 33.13, 49.07, and 72.27 and male (M) specimens were 30.87, 53.73, 69.2 in groups I, II, and III, respectively. The mean number of maxillary teeth was 10.80/6.87/2.8 in females, and 13.27/11.60/6.40 in males groups I, II, and III, respectively. Sample skull specimens are demonstrated in Fig. 4.

Human skull specimens. a Anterior and b lateral view of the male skull specimen aged 35. c Anterior and d lateral view of the female skull specimen aged 34
Craniometric analysis of midface parameters
The mean distances were as follows: B-N (F:76.09/80.78/79.37 mm, M: 81.73/82.33/81.53 mm in groups I/II/III, respectively), B-ANS (F: 86.16/87.45/89.81 mm, M:77.46/83.96/83.25 mm in groups I/II/III, respectively), and B-SD (F:76.06/83.37/81 mm, M:83.67/86.41/87.39 mm in groups I/II/III, respectively). The distance between B-N, B-ANS, and B-SD was greater when group I (young age) was compared with group II (middle age) and III (older age) in both genders with the exception that the B-N distance in male population was slightly (0.2 mm) longer in group I when compared with group III (Tables 1 and 2). However, these results were not statistically significant (p > 0.05). In the female subgroup, B-ANS (p = 0.031) and B-SD (p = 0.043) distances were statistically significant between the groups I and II (Table 1).
There was a statistically significant directly proportional relationship with positive correlation coefficient between B-N and B-ANS distances (p < 0.001, rho 0.54), B-N and B-SD distances (p = 0.001, rho 0.34), and B-ANS and B-SD distances (p < 0.001, rho 0.90) in all skulls independent of age and gender (Table 3).
Craniometric analysis of nasal bones and pyriform aperture
The mean nasal bone lengths were; nasal bone length at midline (F: 20.07/19.67/21.20 mm, M:23.07/22.33/23.13 mm in groups I/II/III, respectively), nasal bone length at lateral suture lines (F:23.9/24.93/24.33 mm, M: 27.03/26.95/27.93 mm in groups I/II/III, respectively), nasal bone width at proximal edges (F: 7.1/7.5/7.1 mm, M: 8/7.8/8.2 mm in groups I/II/III, respectively), and nasal bone width at distal edges (F: 12.46/12.87/12.4 mm, M:13.97/14.8/14.74 mm in groups I/II/III, respectively) (Tables 1 and 2). Analysis of width of proximal and distal edges, length along the midline and lateral suture lines did not show any significant difference between the age groups and genders (Tables 1 and 2). When symmetry was analyzed, the left nasal bone distal width was found to be significantly longer than on the right side in the overall analysis (female and male groups combined, p = 0.044) (Table 4).
The pyriform aperture angle was larger in groups II and III versus groups I in both genders, and also with significantly (p = 0.032) larger in group II versus group I in male gender (p = 0.032) (Tables 1 and 2). The width of the pyriform aperture was significantly larger (p = 0.024) in group III versus group I in males. There were no other statistically significant differences in rest of the parameters (Tables 1 and 2).
There was a positive correlation between aperture width and aperture height but this did not reach statistical significance (p = 0.2, rho 0.14) (Table 3).
Discussion
Characteristics of midface structures and nasal skeleton show variation in different gender and age groups. A clear understanding of the morphology is important for surgeons performing nasal bone and midface surgeries. There are several published reports about direct measurement of nasal bone and nasal pyramid structures [3–7]. Lee et al. reported in their 3D CT study that average Korean nasal bone midline length was (n = 58):22.00 mm (±5.59 mm) in males, and (n = 17): 17.30 mm (±6.00 mm) in females [3]. Moon et al. had similar results in their 3D-CT analysis with a mean nasal bone midline length of 21.28 mm in male group (n = 50) and 18.02 mm in female group (n = 50) [7]. Another Korean study, Hwang et al. found nasal bone length was M: 25.9 mm (±3.8 mm) and F: 24.5 mm (±3.7 mm) [4]. Recently, Lazovic et al. performed cadaver dissections on 22 female Caucasian males and 22 Caucasian females, age 18 to 55 years old, and reported their average nasal bone midline length as 24.77 mm, lateral length of nasal bones as 24.87 mm (right) and 24.77 mm (left), proximal width of nasal bones as 7.12 mm (right) and 6.75 mm (left), and distal width of nasal bones as 11.30 mm (right) and 11.44 mm (left) [5]. Another cadaver study done at Hungary, Palhazi et al. found the average nasal bone midline length as 24.7 mm (range 22–27 mm) in 15 cadavers [6]. In our study, the mean nasal bone lengths of Caucasian skulls at midline were 20.07/19.67/21.20 mm (females), 23.07/22.33/23.13 mm (males) in groups I/II/III, respectively. These and the rest of the nasal bone measurements, as reported in our results, are similar with the existing literature. Our study is one of the largest and most detailed cadaver studies in terms of sample number and analyses in equally distributed age and gender groups.
According to our study, all measured midface and nasal parameters appear to be greater in males, with exception of B-ANS. This might be clinically reflected as a more defined midface in females. Although not based on an objective measurement, the nasal bones of males were observed to be thicker and more durable when compared to females, as expected. Again based on observation, the lower half of the nasal bones were thinner and more brittle in the older age groups. Thus, nasal bone procedures such as nasal bone reductions and osteotomies should be performed meticulously in older age groups to avoid unfavorable and communicated fractures.
When symmetry of left and right nasal bones was analyzed, there was a statistically significant difference between left and right nasal bone distal width measurements in the overall analysis with the left side being larger. The significant difference observed might be due to increased sample size or sampling bias, without a clinical significance. The rest of the nasal bone parameters were measured to be symmetrical, with no statistically significant difference.
The facial skeleton is commonly believed to expand continuously throughout life and there is increase in certain anthropometric measurements with age such as the distance between N-ANS [9]. However, it is not clear whether maxillary bone resorption or nasal bone resorption is the primary cause of this increase [9–13]. Several other studies demonstrate that aging of the maxilla is primarily one of bone resorption [14–18]. A longitudinal methodology demonstrating age-related changes in the same individual is the preferred way of analyzing this change. Although not performed with this methodology, our study shows a tendency of longer N-ANS and shorter ANS-SD distance in older age groups mostly in females, and suggesting that selective bone resorption in the maxillary skeleton is the primary cause of this skeletal remodeling. Although this study focused on the anatomy of the nasal bones and midface, clinical application of our findings to midface is worth mentioning. As discussed by Mendelson and Wong, the facial skeleton, especially midface, is an important target for volume replacement procedures due to significant bone loss and shrinkage occurring in that area [19]. The correction of the facial skeletal framework is increasingly viewed as the new frontier in facial rejuvenation [19]. The greatest bone change occurs in the bones of dental origin, the maxilla and mandible. Our observations showed notable maxillary bone loss at older age groups, mostly in females. This could be due to lack of dental support contributing to bony atrophy as shown in literature [20–22]. Age- and dental-related changes at maxillary bone in older patients should be evaluated carefully before planning facial rejuvenation procedures.
In their adult growth study, Sarnas and Solow found increase in anterior cranial base length by aging indicating that these changes might be due to a combination of forward movement of nasion and posterior movement of sella [23]. In 1985, Behrents noted a similar increase in the length of sella to nasion with a consistent anterior movement of nasion [24]. In their three-dimensional stereolithographic study, Pessa et al. tested a model called Lambro’s algorithm and demonstrated that facial skeleton changes by aging [15, 16]. According to this hypothesis, the bones of facial skeleton rotate clockwise by aging, such as forehead rotates anteriorly and slightly inferiorly while the midface rotates posteriorly and superiorly. In their longitudinal cephalometric study of 39 subjects, Pecora et al. found an increase in the length of sella to nasion, midfacial length, and lower anterior facial height by aging, significantly between late adolescence and midadulthood, that provides further evidence of continuation of changes in the craniofacial complex with age [25]. Our findings of a greater distance of B-N, B-ANS, and B-SD in the older age group supports the theory of anterior displacement of the midface and posterior displacement of B-sella with age (specifically between group I and group II).
Shaw and Kahn’s study found an increase in the pyriform aperture area with age due to bone recession around the pyriform aperture [14, 26]. Our results showed that there is a positive correlation between aperture width and height, meaning when aperture width increases the height also increases. However, these findings were not statistically significant and did not include the measurement of the pyriform aperture area.
In this manuscript, our goal was to perform morphometric measurements of nasal skeleton and midface in different age groups, and observe differences by gender. We had access to mature skulls and data was compared in evenly distributed age and gender groups. We utilized a high precision tool, the MicroScribe®, for calculation of distances and three-dimensional measurements were done with accuracy. In literature, both direct measurement of the dry skulls and CT-based calculations were used in similar studies [3–7]. Although using 3D-CT is found clinically accurate in most publications, a few studies found that CT derived 3D measurements underestimated direct measurements compared to using dry skulls [27, 28]. The 3D-CT data may have potential technical problems (soft-tissue attenuation, metallic artifacts, and patient motion), landmark identification errors (software algorithm, contrast resolution of scan, the thickness and degree of calcification or cortication of bone, and the technical skill of the operator related with 3D-CT), and subsequent measurement errors [27]. Additionally, most of the patients undergoing a head CT scan have a history of cranio/maxillofacial pathology that might distort the normal anatomy of the region. One of the weaknesses of our study is lack of longitudinal methodology, which is the optimal design to evaluate age-related changes. Studying different skulls in different age groups is not the same as studying the same skull during the process of aging. Another shortcoming of our study includes the lack of measurement of skeletal thickness and the inability to calculate bone mineral density which provides important information about bone structure. Finally, this study includes only Caucasian skulls that may reduce the worldwide applicability of our findings.
In conclusion, this study not only supports the existing literature that the midface and the nasal skeleton show variation with age and gender but also adds valuable information about the nasal bone and related parameters. Longitudinal studies along with analysis of other ethnic groups will help us better assess the aging of the nasal and midface bony elements. Also, further studies are needed to understand the relationship between nasal framework and overlying soft tissue during aging. Nasal and midface surgeries should be done with particular attention to different morphology in different age and gender groups in order to provide the patient with an improved physiologic and cosmetic result.
References
Pessa JE, Desvigne LE, Zadoo VP (1999) The effect of skeletal remodeling on the nasal profile: considerations for rhinoplasty in the older patient. Aesthetic Plast Surg 23(4):239–242
Patterson CN (1980) The aging nose: characteristics and correction. Otolaryngol Clin North Am 13(2):275–288
Lee SH, Yang TY, Han GS, Kim Y et al (2008) Analysis of the nasal bone and nasal pyramid by three-dimensional computed tomography. Eur Arch Otorhinolaryngol 265(4):421–424
Hwang TS, Song J, Yoon H, Cho BP et al (2005) Morphometry of the nasal bones and piriform apertures in Koreans. Ann Anat 187(4):411–414
Lazovic GD, Daniel RK, Janosevic LB et al (2015) Rhinoplasty: the nasal bones—anatomy and analysis. Aesthet Surg J 35(3):255–263
Palhazi P, Daniel RK, Kosins AM (2015) Rhinoplasty: the osseocartilaginous vault of the nose: anatomy and surgical observations. Aesthet Surg J 35(3):242–251
Moon KM, Cho G, Sung HM et al (2013) Nasal anthropometry on facial computed tomography scans for rhinoplasty in Koreans. Arch Plast Surg 40(5):610–615
Mendelson B, Wong CH (2012) Changes in the facial skeleton with aging: implications and clinical applications in facial rejuvenation. Aesthetic Plast Surg 36(4):753–760
Bartlett SP, Grossman R, Whitaker LA (1992) Age-related changes of the craniofacial skeleton: an anthropometric and histologic analysis. Plast Reconstr Surg 90(4):592–600
Garn SM, Rohmann CG, Wagner B et al (1967) Continuing bone growth throughout life: a general phenomenon. Am J Phys Anthropol 26(3):313–317
Lasker GW (1953) The age factor in bodily measurements of adult male and female Mexicans. Hum Biol 25(1):50–63
Enlow DH (1966) A morphogenetic analysis of facial growth. Am J Orthod 52(4):283–299
Enlow DH (1979) Facial growth and development. Int J Oral Myol 5(4):7–10
Shaw RB Jr, Kahn DM (2007) Aging of the midface bony elements: a three-dimensional computed tomographic study. Plast Reconstr Surg 119(2):675–681 discussion 682-683
Pessa JE, Zadoo VP, Mutimer KL et al (1998) Relative maxillary retrusion as a natural consequence of aging: combining skeletal and soft-tissue changes into an integrated model of midfacial aging. Plast Reconstr Surg 102(1):205–212
Pessa JE (2000) An algorithm of facial aging: verification of Lambros’s theory by three-dimensional stereolithography, with reference to the pathogenesis of midfacial aging, scleral show, and the lateral suborbital trough deformity. Plast Reconstr Surg 106(2):479–488 discussion 489-490
Mendelson BC, Hartley W, Scott M et al (2007) Age-related changes of the orbit and midcheek and the implications for facial rejuvenation. Aesthetic Plast Surg 31(5):419–423
Pessa JE, Zadoo VP, Yuan C et al (1999b) Concertina effect and facial aging: nonlinear aspects of youthfulness and skeletal remodeling, and why, perhaps, infants have jowls. Plast Reconstr Surg 103(2):635–644
Wong CH, Mendelson B (2015) Newer understanding of specific anatomic targets in the aging face as applied to injectables: aging changes in the craniofacial skeleton and facial ligaments. Plast Reconstr Surg 136(5 Suppl):44S–48S
Chrcanovic BR, Abreu MH, Custodio AL (2010) Morphological variation in dentate and edentulous human mandibles. Surg Radiol Anat 33:203–213
Cawood JI, Howell RA (1988) A classification of the edentulous jaws. Int J Oral MaxillofacSurg 17:232–236
Ozturk CN, Ozturk C, Bozkurt M et al (2013) Dentition, bone loss, and the aging of the mandible. Aesthet Surg J 33(7):967–974
Sarnas KV, Solow B (1980) Early adult changes in the skeletal and soft-tissue profile. Eur J Orthod 2(1):1–12
Behrents RG (1985) An atlas of growth in the aging craniofacial skeleton. in: Craniofacial growth series. Ann Arbor, Mich. Center for Human Growth and Development, University of Michigan
Pecora NG, Baccetti T, McNamara JA Jr (2008) The aging craniofacial complex: a longitudinal cephalometric study from late adolescence to late adulthood. Am J Orthod Dentofac Orthop 134(4):496–505
Shaw RB Jr, Katzel EB, Koltz PF et al (2011) Aging of the facial skeleton: aesthetic implications and rejuvenation strategies. Plast Reconstr Surg 127(1):374–383
Periago DR, Scarfe WC, Moshiri M et al (2008) Linear accuracy and reliability of cone beam CT derived 3-dimensional images constructed using an orthodontic volumetric rendering program. Angle Orthod 78:387–395
Baumgaertel S, Palomo JM, Palomo L et al (2009) Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofac Orthop 136:19–25 discussion 25-28
Acknowledgements
We would like to thank Lyman L Jellema from Cleveland Natural History Museum for his contribution to this publication. We would also like to thank Matthew Karafa, PhD for his help in statistical analysis and Amanda Mendelsohn for her help in illustrations.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Conflict of interest
Can Ozturk, Cemile Nurdan Ozturk, Safak Uygur, Thomas Barrett Sullivan, Mehmet Bozkurt, Franziska Huettner, Risal Djohan, Francis A. Papay declare that they have no conflict of interest.
Funding
None.
Rights and permissions
About this article

Cite this article
Ozturk, C., Ozturk, C.N., Uygur, S. et al. Craniometric analysis of the nasal skeleton and midface in Caucasian population. Eur J Plast Surg 40, 499–506 (2017). https://doi.org/10.1007/s00238-017-1303-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00238-017-1303-1