
Abstract
Background
Pain following mastectomy often require use of opioids, drugs associated with a significant number of side effects. This study investigated the effect of a single perioperative infusion of bupivacaine in the mastectomy cavity on the postoperative outcomes: use of opioids, pain score, and nausea.
Methods
This retrospective cohort included 244 women undergoing mastectomies at the Odense University Hospital, Denmark. Thirty-five patients received bupivacaine in the mastectomy cavity and were compared to 209 controls who had no local analgesic.
Results
A reduction in the postoperative use of 6.1 “oral morphine equivalents” (OMEQs) was observed in the infusion group in the first 24 h after mastectomy compared to a control group not receiving infusion. This corresponds to a reduction of 6.1 mg of orally administered morphine, equivalent to a 52 % reduction. This was, however, not statistically significant (p = 0.1208). No statistically significant differences between the two groups were found in visual analogue scale (VAS) scores for pain and nausea or in the use of other nonopioid analgesics.
Conclusions
A single perioperative infusion of bupivacaine may have a morphine-sparing effect in the first 24 h after mastectomy. Our results were however not statistically significant when tested on these low-pain surgical procedures. Infusion of analgesics in surgical cavities is simple, fast, and low cost. It might prevent the often seen vicious cycle of nausea and impaired coping with postsurgical pain when patients are introduced to opioids.
Level of Evidence: Level III, therapeutic study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Women undergoing breast surgery for breast cancer experience some degree of postoperative pain, often located to the chest wall, breast, and scar [1]. Pain after breast surgery is generally mild to moderate and most prominent in the acute phase [2]. There is increasing evidence suggesting that acute postoperative pain increases the risk of chronic pain. Chronic postmastectomy or postlumpectomy pain syndrome is a well-known complication with prevalence rates ranging from 20 to 68 % in people who have undergone breast surgery [1, 3–5]. Optimal postoperative care is therefore a keystone in reducing the risk of chronic pain.
The current general postop regimen, supported by a review in Acta Anaesthesiologica Scandinavica, consists of a combination of paracetamol and ibuprofen as first-line pain relief. With the presence of pain requiring more analgesia, opioids is regarded as the most effective [6]. The use of opioids is however associated with side effects: sedation, dysphoria, nausea, itching, and formications, all potentially causing a delay in recovery [7]. Use of baseline analgesics should therefore be optimized in an attempt to reduce the use of opioids.
Administration of local analgesics (LA) during surgery could be a useful addition to the current regimen of basic pain relief. It is a low-cost technique for postoperative analgesia that is safe and has few side effects [2]. Infiltration is the technique most widely used when administering LA [8, 9]. An alternative to infiltration could be simple infusion, either manually as a one-time infusion or continuous using a pump. With the advantage being that infusion is easier, no needle tissue trauma is induced and that administration is at the exact location of the surgical trauma [10]. A recent RCT by Laso et al., with a setup, similar to ours, investigated the effect of continuous infusion of local analgesic and concluded that it reduces pain and analgesic consumption with high satisfaction, but does not affect the rates of nausea and vomiting [11]. What remains to be investigated is if the same effect can be seen using a one-time infusion only.
In this retrospective cohort study, we tested the hypothesis that a single perioperative infusion of bupivacaine in the cavity after unilateral mastectomy would reduce the time spent in the recovery unit, visual analogue scale (VAS) scores for pain and nausea and the use of postoperative analgesics in the first 24 h post-op, mainly focusing on the use of morphine.
Methods
All procedures and data collection were performed in the department of plastic surgery at the Odense University Hospital (OUH), Denmark, during the period 01.01.13–30.06.14, with the statistical analysis made medio 2015.
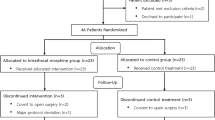
The population chosen was women undergoing unilateral mastectomy with or without removal of sentinel lymph node or radical lymph node dissection of the axillae. From the period chosen, 311 patients were identified and included in the study. Patients were excluded if any of the following criteria were met: (1) primary reconstruction was performed immediately after mastectomy, (2) records of the surgery and/or time after were missing, (3) inconsistent records, (4) males, (5) new surgery within 24 h due to complications, (6) lumpectomy was performed instead of planned mastectomy, and (7) bilateral mastectomy. Two hundred forty-five patients were eligible for inclusion in the final statistical analysis, with 35 being in the intervention group receiving infusion.
Over the last 2 years, one out of five of the breast surgeons at the department used infusion when performing mastectomies, placing 20 ml of Marcaine© (bupivacaine) 5 mg/ml injection solution into the operation cavity. All patients had drains placed in the operation cavity. Patients in the infusion group had the bupivacaine solution administered through these drains immediately after closure of the wound. The drains were then closed for 20 min, allowing for the analgesics to be absorbed, before opening and draining the cavity. The control group received no infusion. Allocation of time of surgery and surgeon was decided at the preoperation consultation where women choosing to undergo surgery were given the first available time.
After surgery, patients were transported to the recovery unit allowing full recovery from the anesthesia, before transportation to the breast ward. VAS scores for pain and nausea were recorded at the time of arrival and departure from the recovery ward. Patients were given analgesics depending on their VAS scores and the nurses’ evaluation of prospective pain. Most patients were given 1 g paracetamol perorally (PO) and 5 mg morphine PO as preventive analgesics. Though the VAS is accessed as a scale ranging 0–10, it was recorded in the patient files as a scale ranging from 0 to 3, representing the following: 0, no pain OR VAS = 0; 1, low pain OR VAS < 3; 2, moderate pain OR 3 ≤ VAS < 7; and 3, pronounced/greater pain OR VAS ≥ 7. VAS has therefore been statistically calculated from this scale.
Patients were stratified into two main groups, the infusion group receiving bupivacaine as infusion into the mastectomy cavity and the no infusion group, acting as control group (n = 35 vs. n = 209). To investigate possible differences depending on type of surgery, further stratification was made into the following: group 1, simple mastectomy (SM); group 2, mastectomy + sentinel node (M + SN); group 3, mastectomy + axillary node dissection (M + ALND).
Patients received different types of opioid agonists. For comparative reasons, all opioid drugs were converted into oral morphine equivalents (OMEQs), using a Web-based converter [7]. One OMEQ being equal to 1 mg orally administered morphine [7, 12]. The use of morphine is also stated as used morphine PO and parenteral (PE) for explanatory use.
Propensity score matching (PSM) was performed prior to statistical analysis, with a propensity score being calculated for each patient on the basis of a logistic regression on the probability of being in the infusion group, using age, BMI, and type of surgery. Nearest neighbor matching was used as matching algorithm, matching each patient in the infusion group, with four patients in the no infusion group. We ran nearest neighbor matching for ratios 1:1–1:5, resulting in the ratio of 1:4 being used as this was the ratio resulting in the least difference between our group covariates. No maximum caliper width was specified, resulting in a full matching of all patients in the treatment group. As a result, the statistical analysis included 35 patients in the infusion group and 140 in the control group. Sixty-nine patients in the control group were excluded.
The normality of distribution of the initial data was assessed using the Shapiro-Wilk W test. Equality of variance was estimated using a variance-ratio test. Most data were not normally distributed according to the Shapiro-Wilk W test. When variances did not differ statistically significantly and were estimated to be equal, the Student’s t test was used for comparing means. For data where variances did differ, the Welch t test was used, as it allows for unequal variances. Association between categorical variables was analyzed using Pearson’s goodness of fit, chi-squared test.
P < 0.05 was chosen as the cutoff point for significance. PSM was performed using R, and statistical analysis was made using STATA 13.
Results
The characteristics of the women participating in the two groups were similar, and no significant difference was found when comparing the stratified groups (Tables 1 and 2). We investigated VAS scores for pain and nausea at arrival and departure from recovery room. For all groups, median VAS was 0 and no significant differences were found.
Performing the PSM reduced the differences in covariates between the infusion and the no infusion group. Looking at Table 1, the mean difference in age between the two groups was reduced from 0.9 to 0.1 years. For BMI, the original difference was 0.9 and only 0.1 after performing the PSM. Table 2, illustrating the distribution of patients by operation type, also shows a great reduction in the differences in distribution between our groups.
Outcomes of interest are shown in Table 3. There was no difference between the two groups when looking at time spent in the recovery unit (p = 0.7205). Regarding the use of both morphine PO and morphine PE, the two groups were almost identical with a difference of only 1 mg. When looking at OMEQs, with all opioids converted, a reduction of 6.1 OMEQs was seen in the infusion group compared to the no infusion group. This corresponds to an absolute reduction of 6.1 mg orally administered morphine, and relative reduction of 52 %. The reduction was, however, not found to be statistically significant (p = 0.1208).
When comparing OMEQ use between the groups stratifying into subcategories, we found a reduction in opioid use in the M + SN group and an increase in the SM and M + ALND group. With the differences between the infusion and no infusion group being SM diff = 16.2, M + SN diff = −6.4, and M + ALND diff = 2.3. No subcategory p value for OMEQs reached level of significance. In number of administrations of OMEQs, there was no difference between the groups.
The use of paracetamol was equal in the two groups, with a mean of 0.9 g (p = 0.7679). A trend of reduction in the use of ibuprofen was seen in the infusion group compared to the no infusion group (11.1 vs 37.1 mg) (p = 0.1028).
Conclusions
The present study found, although not statistically significant, a reduction in the use of postoperative morphine (OMEQs) when patients were given a one-time infusion of bupivacaine in the wound following mastectomy.
The included population was selected from a random period of time, came from all over the county of Funen and is therefore regarded as being a representative group of the Danish population.
There are several methods of finding a comparative value for drugs in drug consumption studies, with the most widely used being “defined daily dose” (DDT). DDT has a different value depending on what indication it is given for. OMEQ was chosen as measurement unit over DDT, because of the homogeneity in indication of analgesics in our population. Additionally, a Norwegian study concluded that OMEQ better reflects clinical dosing compared to DDT [12]. The OMEQ allowed the converting of different opioid agonists, opioid alternatives, and analgesics containing opioids and other substances, into the equivalent dose of oral morphine, hence making the comparison of used analgesics more defined, uniform, and arguably more transmissible into everyday clinical life. For patients stating allergies toward morphine, alternatives were given. These alternative drugs are not included in the calculations when looking at morphine alone. As this only applies to three patients, all in the no infusion group, the influence on our results should be small. The morphine alternatives are all included in the OMEQ. The OMEQ is therefore regarded as the most accurate when comparing the opioid use of our patients.
When looking at total administered OMEQs, a reduction of 6.1 OMEQs was seen in the infusion group compared to the no infusion group. At the same time, there was no difference in number of administrations of morphine between the groups, raising the question of the clinical relevance of the reduction. Still, with the reduction being 52 %, it suggests that it is possible to reduce the use of opioids among patients experiencing lower degrees of pain and that infusion should be taken into consideration when treatment is planned.
Our results regarding the use of OMEQs, indicating a reduction when applying LA to operation wound, are in line with the large RCT published by Laso et al. and the majority of studies included in the Danish review by Byager et al. [2, 11]. When investigating the effect of continuous infusion of LA by pump, they found a significant reduction in postoperative pain. Our results with the median VAS pain score being 0 in all groups suggests that patients undergoing mastectomies at OUH, in general, experience low levels of postoperative acute pain. As our results did not reach level of significance, compared to the previously mentioned studies, one could argue that continuous infusion of LA by pump is more effective than a one-time infusion. On the other hand, the low-pain levels seen in our patients make a possible reduction hard to find. Regarding the RCT by Laso et al., several differences in their methods compared to ours, could explain some of the increased effect seen in their study [11]. First of all, the patients in the mentioned RCT received a total of 100 ml 5 mg/ml levobupivacaine + 30 ml levobupivacaine 2.5 mg/ml, compared to our patients who only received 20 ml 5 mg/ml bupivacaine. The amount LA administered was therefore around six times higher in their study. Second, Laso et al. administered the drugs by pump for a duration of 48 h, while we used a single perioperative infusion. Third, levobupivacaine used in the RCT, compared to bupivacaine, has a longer duration of action, possibly increasing its analgesic effect. Finally, Laso et al. recorded patient use of analgesics for 48 h compared to our 24 h, leading to a higher total analgesics use per patient. This could arguably have made an effect easier to find. As most of our patients are discharged within 24 h, monitoring their analgesics longer than this was not an option. All of these factors could explain why our study failed to show the same effect as this large RCT did. Regarding postoperative nausea, we did not see an effect of infusion of LA, a result in line with Laso et al.
The degree of trauma should correlate with the degree of postoperative pain. If this is the case, we would have seen tendency of the least morphine administered in the SM group and the greatest use in the M + ALND group. This is supported by a study published by Gärtner et al. with results showing an increase in pain present postoperatively in patients undergoing M + ALND compared to M + SN (OR (95 % CI), 1.77 (1.43–2.19)) [4]. No such tendency was seen in our results. This might be due to blurring of a trend by the generally low pain scores.
Our results were calculated without taking the effect of comorbidity into consideration, including previous breast and thoracic surgery. Comorbidity could therefore have affected the results, but since no allocation into groups due to comorbidity has occurred, it seems reasonable to assume that patients with comorbidity were equally distributed in the two groups.
One major drawback of this study is the fact that all surgeries in the infusion group were performed by the same surgeon, while the no infusion group had five different surgeons. Intersurgeon differences in procedure, affecting the results of this study, could therefore be present. Every surgeon was meticulously trained by the same surgeon and are all obliged to follow the procedural guidelines made by the Danish Breast Cancer Cooperative Group regarding mastectomies when performing these surgeries. All have reported doing so in their postoperative notes. Potential differences in procedures should therefore arguably be minor. As previously mentioned, all patients were assigned the first available time of operation. The allocation of surgery may, however, still be biased and as we are comparing our study to studies where allocation have been randomized, caution should be taken. In an effort to reduce the effect of allocation bias and to mimic a RCT, we used propensity score matching when preparing our data for statistical analysis. Prior to analysis, each patient in the intervention group was matched with one or more patients in the control group. By accounting for the covariates that predict receiving treatment, we could estimate the effect of the intervention more accurately. When looking at the characteristics of our groups in Tables 1 and 2, we can clearly see that the PSM contributed in making the covariates across our groups more similar. The difference of means decreased, and the p values are now even stronger in indicating that the groups are not significantly different. This, in other words, helped transform our study into a quasi-randomized study. We chose to compare our cases with four patients in the intervention group, as this made for the most balanced dataset. A portion of our original control group was therefore excluded from our statistical analysis, but this was in our opinion acceptable as the quasi-randomization is a great addition to our study design. As PSM only accounts for observed covariates, latent variables may have been present after matching, but they should arguably be covariates of lesser importance.
In conclusion, a single perioperative infusion of bupivacaine may have a morphine sparing effect in the first 24 h after mastectomy, with our results showing a reduction of 52 % in OMEQs. The infusion technique was completely without complications. It is a simple, fast, and low-cost technique which might prevent the often seen vicious cycle of nausea and impaired coping with postsurgical pain when patients are introduced to opioids. However, the results were not statistically significant when tested on this low-pain surgical procedure. Further investigation to examine the potential of infusion as a way of reducing postoperative use of opioids is needed.
References
Perkins FM, Kehlet H (2000) Chronic pain as an outcome of surgery. A review of predictive factors. Anesthesiology 93(4):1123–1133
Byager N, Hansen MS, Mathiesen O, Dahl JB (2014) The analgesic effect of wound infiltration with local anaesthetics after breast surgery: a qualitative systematic review. Acta Anaesthesiol Scand 58(4):402–410
Fassoulaki A, Melemeni A, Staikou C, Triga A, Sarantopoulos C (2008) Acute postoperative pain predicts chronic pain and long-term analgesic requirements after breast surgery for cancer. Acta Anaesthesiol Belg 59(4):241–248
Gartner R, Jensen MB, Nielsen J, Ewertz M, Kroman N, Kehlet H (2009) Prevalence of and factors associated with persistent pain following breast cancer surgery. JAMA 302(18):1985–1992
Bokhari FN, McMillan DE, McClement S, Daeninck PJ (2012) Pilot study of a survey to identify the prevalence of and risk factors for chronic neuropathic pain following breast cancer surgery. Oncol Nurs Forum 39(2):E141–149
Dahl V, Raeder JC (2000) Non-opioid postoperative analgesia. Acta Anaesthesiol Scand 44(10):1191–1203
Handberg G JN, Maagaard R (2015) Rene agonister. Dansk Lægemiddel information A/S. http://pro.medicin.dk/Laegemiddelgrupper/Grupper/227010. Accessed 30 Jan 2015
Campbell I, Cavanagh S, Creighton J et al (2014) To infiltrate or not? Acute effects of local anaesthetic in breast surgery. ANZ J Surg. doi:10.1111/ans.12541
Zielinski J, Jaworski R, Smietanska I, Irga N, Wujtewicz M, Jaskiewicz J (2011) A randomized, double-blind, placebo-controlled trial of preemptive analgesia with bupivacaine in patients undergoing mastectomy for carcinoma of the breast. Med Sci Monit 17(10):CR589–597
Scott NB (2010) Wound infiltration for surgery. Anaesthesia 65(Suppl 1):67–75
Ferreira Laso L, Lopez-Picado A, Lamata L et al (2014) Postoperative analgesia by infusion of local anesthetic into the surgical wound after modified radical mastectomy: a randomized clinical trial. Plast Reconstr Surg 134(6):862e–870e
Svendsen K, Borchgrevink P, Fredheim O, Hamunen K, Mellbye A, Dale O (2011) Choosing the unit of measurement counts: the use of oral morphine equivalents in studies of opioid consumption is a useful addition to defined daily doses. Palliat Med 25(7):725–732
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
This study received no funding.
Conflict of interest
Martin Sollie and Camilla Bille declare that they have no conflict of interest.
Ethical standards
This study was performed as a retrospective case study, and therefore, approval from the regional ethical committee was not necessary.
Patient consent
Patient provided written consent before their inclusion in this study.
Rights and permissions
About this article

Cite this article
Sollie, M., Bille, C. The use of a single local analgesics infusion in operation cavity following mastectomy and its effect on postoperative pain—a retrospective cohort study. Eur J Plast Surg 39, 273–278 (2016). https://doi.org/10.1007/s00238-016-1195-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00238-016-1195-5