
Abstract
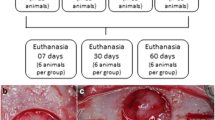
The aim of this study was to evaluate the morphological bone response in animal experiments by applying hydroxyapatite grafts in critical and non-critical size bone defects. Current report followed the guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Animal experiments were selected by assessing repair of bone defects with hydroxyapatite as bone graft and with blood clot only as control. Eight articles were identified in specialized literature and included in the meta-analysis. Statistical analysis was carried out with a random-effect model (p = 0.05). Subgroup analyses were further performed to investigate bone repair in critical and non-critical bone defects. Comprehensive analysis of bone repair outcome showed a statistically significant difference between hydroxyapatite and blood clot control (p < 0.05). Subgroup analyses showed statistically significant difference for critical bone defects (p < 0.05). No statistically significant difference was reported in non-critical bone defects (p > 0.05). Although animal studies revealed a high risk of bias and results should be interpreted with caution, the literature suggests that non-critical bone defects may heal spontaneously and without the need of a bone graft. Conversely, when critical-size defects are present, the use of hydroxyapatite bone graft improves the bone repair process.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Bone is a composite natural tissue susceptible to fracture which may be caused by trauma, pathology and resorption [1]. Defects and functional disorders of the tissue have become a global health care problem and tissue engineering has turned to be an important approach in bone regeneration research [2]. Bone tissue engineering involves the use of suitable materials for temporary tridimensional matrix to guide cell adhesion, differentiation, proliferation and subsequent tissue regeneration [3]. Techniques for bone engineering currently include the replacement of damaged bone with autograft, allograft, xenografts and artificially synthesized bone materials [4]. Autologous grafts, or tissues from the patient, are considered the gold standard since they have all the characteristics necessary for the growth of new bone [5]. In the case of autologous bone grafting, bone is transplanted from one site of the body, usually the iliac crest, to another site of the same patient [6]. However, autografting has several drawbacks, such as risks and discomfort to the patient due to additional surgery for bone tissue removal, pain at the donor site, limited bone supply at the donor site or even infections in the region [4, 7].
The above difficulties have triggered researchers for solutions, and as result, the development of bone repair materials has become a hotspot in research. The use of natural bone substitutes or synthetic grafts may overcome the disadvantages of using autologous bone grafts [6]. Biocompatibility, non-toxicity, low cost, non-carcinogenicity, with excellent osteoconductive and osteoinductive properties, are among the desirable characteristics of biomaterials for bone replacements [8].
The primary materials that have been used in bone fracture repair include bone, bone cements, metals, ceramics, polymers and composites [9]. Calcium orthophosphate ceramics (CaPs) is one of the most popular bone substitutes since its chemical composition is almost identical to bone mineral [4]. These materials have excellent biological behavior (biocompatibility, bioactivity and osteoconductivity); they are low cost and widely available [10]. CaPs represents a large family of substances with a Calcium/Phosphate molar ratio between 0.2 and 2.0, including tricalcium phosphate (TCP), hydroxyapatite (HA), biphasic calcium phosphates (BCP), monocalcium phosphate monohydrate (MCPM) and unsaturated apatite (AP) [11].
HA is a widely available bioactive and bioresorbable calcium phosphate that constitutes most of the inorganic component of bone tissue [7]. HA Ca10(PO4)6(OH)2 may be found in chemically identical natural or synthetic forms, differing only in their physical microstructure, crystal size and porosity [4]. HA directly bonds with live bone after implantation in cases of bone defects [3]. This feature enhances appropriate vascularization and stem cell proliferation, and guides bone regeneration without causing any local or systemic toxicity [11]. Both natural and synthetic HA are available in pastes, putties, solid matrices, and granules [12].
Histological evaluation is the primary means in assessing the effect of bone substitutes in tissues [13]. However, tissue removal is mandatory in this type of analysis, precluding its use in clinical trials. Therefore, most studies on bone repair employ animal experiments which provide relatively reproducible and quantifiable information. The current systematic review evaluates morphological bone response in animal models by applying hydroxyapatite grafts in bone defects characterized as critical and non-critical size. Hypothesis tested whether hydroxyapatite would enhance bone repair in bone defects.
Materials and Methods
Current systematic review followed the guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA Statement). The main research question is: do hydroxyapatite grafts improve bone healing in bone defects of critical and non-critical size in animal models?
Systematic Literature Search
Research in specialized literature was conducted by two independent reviewers until October 2016, with no limit in publication year. The following databases were searched: PubMed (MedLine), ISI Web of Science, Lilacs, Ibecs, BBO, Scopus and Scielo. Search strategy developed for PubMed (MedLine) is listed in Table 1, and was adapted for use in other databases. Terms related to hydroxyapatite and animal experiments were crossed to optimize the retrieval of relevant documents and references cited in the papers were also hand-searched to identify other potentially relevant articles. All documents were imported into Endnote X7 software (Thompson Reuters, Philadelphia, PA, USA) to remove duplicates. The reviewers assessed titles and abstracts of all the documents.
Study Selection
Two reviewers independently searched the eligible items according to eligibility criteria (Table 2). As inclusion criteria, it was included animal experiments with hydroxyapatite both natural or synthetic applied in circumscribed bone defects. We included animal experiments once they are the step before clinical evaluation in humans, and their results may provide valuable data for translational research. Moreover, in order to represent the physiological bone healing process it was only included studies in which the defects unfilled (only blood clot) were used as the control group. As exclusion criteria, studies that hydroxyapatite was used in periodontal or alveolar defects, or in tissue engineering approaches (with growth factors or stem cells) were not included, since our purpose was to evaluate the morphological response of hydroxyapatite grafts alone in critical and non-critical size bone defects. Besides, studies investigating only macroscopic, microtomography or x-ray results were not included, once the morphological response with histological analysis could not be evaluated. When relevant information to eligibility criteria was not available in the abstract, the article was selected for full reading. If reviewers disagreed further discussion ensued till consensus. Only articles that fulfilled all eligibility criteria were accepted.
Data Extraction
Data were retrieved by standardized form in Microsoft Office Excel 2013 software (Microsoft Corporation, Redmond, WA, USA). If any information was missing, the authors of the included papers were contacted via e-mail to provide the specific data. Reviewers tabulated the following data of all included studies: authors, country, year, type and number of animals, sex, size defect, local defect, type of hydroxyapatite and number of bone defects evaluated (Table 3). Table 4 shows studies included in the meta-analysis, whilst Table 5 describes the main data.
Statistical Analysis
Analyses were performed by Review Manager Software 5.2 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). The first global analysis was carried out using a random-effect model and pooled-effect estimates were obtained by comparing standardized mean difference of bone repair in hydroxyapatite group with the control treatments (unfilled bone defects), at p < 0.05 significance. Additionally, subgroup analyses were performed for the analysis of bone repair only in critical and non-critical bone defects. Statistical heterogeneity of treatment effect among studies was assessed with Cochran’s Q test and inconsistency with I 2 test, in which rates greater than 50% indicated substantial heterogeneity [14].
Quality Assessment
The methodological quality of each included study was independently assessed by the two reviewers, based on the SYRCLE’s risk of bias tool for animal studies [15]. The studies were evaluated to provide a framework for judging the methodological quality of animal experiments according to the following information: random sequence generation (selection bias), baseline characteristics (selection bias), allocation concealment (selection bias), random housing (performance bias), blinding of caregivers and/or investigators (performance bias), random outcome assessment (detection bias), blinding of outcome assessment (detection bias), incomplete outcome data (attrition bias), selective reporting (reporting bias) and other biases. Each component was graded as low, unclear or high risk of bias in software RevMan 5.2 (The Cochrane Collaboration, Denmark).
Results
Search Strategy
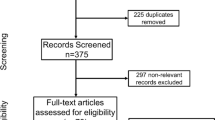
Initial search in databases identified 4101 potentially relevant records. Figure 1 shows the flowchart that summarizes the article selection process according to the PRISMA Statement. Duplicates were removed and 3414 records were examined by titles and abstracts. Seventy-five articles were focused for full-text reading, after which 41 were excluded because they failed to meet eligibility criteria. Thirty-two studies fulfilled all selection criteria and were included in this review.

Search flow (as described in the PRISMA statement)
Descriptive Analysis
Table 3 shows data on studies in which six different types of animals were evaluated, namely, 13 rabbits [16,17,18,19,20,21,22,23,24,25,26,27,28], 10 rats [29,30,31,32,33,34,35,36,37,38], 4 dogs [39,40,41,42], 3 pigs [43,44,45], one sheep [46] and one goat [47]. Twelve out of the 33 articles used males [17, 26, 28, 29, 31, 33,34,35,36,37, 39, 40], 4 used females [16, 19, 27, 44], 3 used both sex [20, 21, 47] and 13 failed to report gender [18, 22,23,24,25, 30, 32, 38, 41,42,43, 45, 46]. Regarding to the site for holding the bone defect, the preference sites comprised skull [16, 20, 23, 24, 26,27,28,29,30, 32, 34,35,36, 42, 44, 45], jaws [25, 38, 39, 43, 46], tibia [29], femur [22, 31, 33, 37], tibia [18, 19, 21, 41], radius [47], humerus [40] and hind limbs [17]. More than half (21) used size defects informed by the author as non-critical, whereas only 10 articles qualified the defects as critical [16, 19, 27, 28, 30, 34,35,36, 42, 44]. There was doubt whether the defect really exhibited any critical size occurred only in a single article [40]. Although there were great variations in the hydroxyapatite used, coral-derived hydroxyapatite was predominant [16, 17, 22, 27, 30, 38, 42, 43, 45, 48].
Meta-Analysis
A meta-analysis was performed with 8 animal studies [21, 23, 24, 29, 35, 40, 42, 43]. The global analysis of bone repair with hydroxyapatite (Fig. 2) showed a statistically significant difference when compared with control (p < 0.05). Although the rate of I 2 test was 75%, in the subgroup analysis with only non-critical bone defects, 5 studies could be included (Fig. 3a), with no statistically significant difference of hydroxyapatite when compared to control (p = 0.05; I 2 = 85%). Further, there were statistically significant differences between treatments (p = 0.03; I 2 = 60%) in the use of hydroxyapatite in critical bone defects (Fig. 3b).

Results for the global analysis of bone repair with hydroxyapatite compared to control treatments using random-effects models. Statistically significant differences between groups (p = 0.05) were observed

Results for the subgroup analysis of bone repair with hydroxyapatite in a non-critical and b critical bone defects compared to control treatments. Statistically significant differences between groups only in critical bone defects analysis (p = 0.03)
Quality Assessment
With regard to assessment of risk of bias, Fig. 4 summarizes the information used to assess the studies´ methodological quality. Studies scored particularly poorly on the following items: random sequence generation (selection bias), random housing (performance bias), blinding of caregivers and/or investigators (performance bias), random outcome assessment (detection bias), blinding of outcome assessment (detection bias) and selective reporting (reporting bias).

Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies
Discussion
The systematic review of animal experiments revealed improvement of bone repair by hydroxyapatite. However, in non-critical bone defects, the use of hydroxyapatite failed to improve the bone repair process when the latter was compared to blood clot control. Consequently, the hypothesis above was only partially proved. Several studies could not be included in the meta-analysis because the quantitative results were incomplete or their results were only qualitative. Further, deep heterogeneity was detected in the meta-analysis of animal studies, which varied according to the animals evaluated, induced bone defect and different types of hydroxyapatite employed.
By definition, a critical-sized defect (CSD) is the smallest size intraosseous defect in a particular bone that fails to heal completely during the natural lifetime of an animal [49]. In these cases, critical defects are not adequately filled by bone tissue since it lacks spontaneous healing capacity due to its size. Studies analyzed in this review corroborate the above statement. In fact, when a critical size defect is employed, a minimal amount of bone growth has occurred in groups in which no bone graft was used [35, 40, 42]. Results from current meta-analyses suggest that hydroxyapatite may be used successfully as material for bone repair when a CSD was induced.
It has been previously demonstrated that several calcium-phosphate ceramics, including HA, prop new bone formation [50]. These materials, main keys in bone formation, deposit extracellular matrix within the bone defects [11]. Moreover, the presence of Ca2+ ions on the material surfaces enhance protein absorption, which facilitates bone-forming cell adhesion and subsequent bone matrix deposition, osteoblast activity and angiogenesis [51,52,53]. Complex interaction processes between cells and micro-environment, which result in the bone regeneration process, may also be affected by the topography, geometry, composition, grain size and percent porosity of the scaffolds used [54, 55].
Several researchers discovered that the original definition of CSD is not truly functional and suggested that the critical-size defect in animal research should refer to the size of a defect that will not heal throughout the duration of the study and not to the entire life of the animal [56, 57]. It has also been suggested that critical defects cannot only be defined by their size, but should depend on other factors too, including age, species phylogeny and metabolic and systemic conditions [58, 59]. Five studies were included in the subgroup analysis considering only non-critical bone defects [21, 23, 24, 29, 43]. Meta-analysis of data derived from these studies showed that the use of a bone graft did not improve the healing process, and spontaneous regeneration occurred among the defects evaluated. The latter proves that the injured bone is able to recover itself from small bone defects. The natural healing of bone defects resembles bone formation during organogenesis. After bone injury, an inflammatory response occurs and extravascular blood cells form a blood clot. This initial response involves the secretion of growth factors which recruit inflammatory cells and promote angiogenesis. After early immune reaction, a soft callus around the injury site is formed leading to a disorganized structure termed woven bone. In later phases of bone regeneration, the woven bone is gradually replaced by a highly organized lamellar bone. Eventually, woven bone and fracture callus are replaced by lamellar or trabecular bone produced by osteoblasts [60, 61].
In general, studies with non-critical size defects show that, during the initial follow-up, the progression of bone growth in the control defects occurs more quickly than in the defects filled with hydroxyapatite. The above corroborates few reports that have described an initial negative cellular response in the presence of calcium orthophosphate ceramics in which low proliferation of osteoblastic cells did not enhance in vitro osteogenesis due to insufficient activation of signaling that forced the cell cycle to progress [62,63,64]. Since subsequent events leads towards a complete healing, there are indications that the influence of calcium orthophosphate materials (similar to HA) on bone repair may also dependent on other factors, such as animal species, anatomic defect location, fracture stabilization, associated soft tissue and biomechanical conditions, as well as metabolic and systemic conditions, and morbidities affecting defect healing [65].
Since the exact mechanisms of osteoinduction of bone graft materials are still unclear, it is important to mention that the use of small defects in studies with bone substitutes is also extremely relevant when the primary objective refers to the evaluation of tissue response and not merely to the ability to improve regeneration. Other methods are extant to evaluate the growth of bone in bony defects, such as microtomography or x-ray. The histological approach to evaluate the biological performance of bone grafts continues to be very important to report on the qualitative and qualitative fracture repair process [66]. Unfortunately, for ethical reasons, the histological approach is not allowed on humans and different animal models should be used.
Although this is the best currently available evidence demonstrating that hydroxyapatite in critical bone defects is beneficial, only animal studies have been analyzed and the strength of the clinical inference is not strong. Besides, results should be interpreted with caution since animal studies revealed a high risk of bias. The studies also showed heterogeneity concerning the type of hydroxyapatite used and to treatment protocol, which precluded direct comparison. Additionally, the majority of the selected studies investigated calvarial defects, notwithstanding, in humans, bone defects affect more long bones or mandible. It should be noted that clinical application in animal models represents the final step before clinical application in humans, and the results from these studies have provided insights for translational research. Further, the quality of the included studies emphasized the need for further well-designed, randomized and controlled animal studies to highlight the benefits in the employment of hydroxyapatite in bone defects. Factors such as random sequence generation, sample size calculation, blinding outcome assessment, and use of different evaluation methods may improve the quality of more in-depth studies in this research field. Although only a few included studies were published after the publication of Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines [67], the compliance to standards in reports on animal studies may improve their quality and facilitate the comparison between different treatments in future systematic reviews.
Evidence found in current systematic review supports the use of pure HA bone grafts, natural or synthetic, to enhance adequate bone healing in critical and non-critical sized defects. Regardless of the form (block, granules or particles), it seems that ceramic calcium orthophosphate ceramic favors bone regeneration in several clinical conditions. In the current review, the analysis of isolated HA without any growth factor or stem cells demonstrated the performance of the substrate as an osteoconductive material which may be an ideal material for scaffolds in future tissue-engineering approaches.
Finally, significant challenges are still extant in bone tissue repair and regeneration. As far as is known, no ideal bone substitute has been developed. The best combination between micro and macro characteristics to achieve adequate osteoconductive properties, coupled to a simple process for manufacturing, are still required. Further, large bone defects still represent a major challenge and future research will have to focus on the development of bone grafts and biomimetics with the appropriate controlled release of osteogenic factors. Although the above are significant challenges, it is becoming evident that the successful development of materials in this research field has long-lasting benefits that surpass potential risks.
References
Gu Y, Wang G, Zhang X et al (2014) Biodegradable borosilicate bioactive glass scaffolds with a trabecular microstructure for bone repair. Mater Sci Eng C Mater Biol Appl 36:294–300. doi:10.1016/j.msec.2013.12.023
Chen FM, Liu X (2016) Advancing biomaterials of human origin for tissue engineering. Prog Polym Sci 53:86–168. doi:10.1016/j.progpolymsci.2015.02.004
Gao C, Deng Y, Feng P et al (2014) Current progress in bioactive ceramic scaffolds for bone repair and regeneration. Int J Mol Sci 15:4714–4732. doi:10.3390/ijms15034714
Tan L, Yu X, Wan P, Yang K (2013) Biodegradable materials for bone repairs: a review. J Mater Sci Technol 29:503–513. doi:10.1016/j.jmst.2013.03.002
Zhang J, Liu W, Schnitzler V et al (2014) Calcium phosphate cements for bone substitution: chemistry, handling and mechanical properties. Acta Biomater 10:1035–1049. doi:10.1016/j.actbio.2013.11.001
García-Gareta E, Coathup MJ, Blunn GW (2015) Osteoinduction of bone grafting materials for bone repair and regeneration. Bone 81:112–121. doi:10.1016/j.bone.2015.07.007
Sheikh Z, Najeeb S, Khurshid Z et al (2015) Biodegradable materials for bone repair and tissue engineering applications. Materials 8:5744–5794. doi:10.3390/ma8095273
Ricciardi BF, Bostrom MP (2013) Bone graft substitutes: claims and credibility. Semin Arthroplast 24:119–123. doi:10.1053/j.sart.2013.07.002
Mahyudin F, Widhiyanto L, Hermawan H (2016) Biomaterials in orthopaedics. In: Advanced structured materials. pp 161–181
Zhang J, Liu W, Schnitzler V et al (2013) Review: calcium phosphate cements (CPCs) for bone substitution: chemistry, handling and mechanical properties. Acta Biomater 10:1035–1049. doi:10.1016/j.actbio.2013.11.001
Yu X, Tang X, Gohil SV, Laurencin CT (2015) Biomaterials for bone regenerative engineering. Adv Healthc Mater 4:1268–1285. doi:10.1002/adhm.201400760
Pepla E, Besharat LK, Palaia G et al (2014) Nano-hydroxyapatite and its applications in preventive, restorative and regenerative dentistry: a review of literature. Ann Stomatol 5:108–114
Schortinghuis J, Ruben JL, Meijer HJA et al (2003) Microradiography to evaluate bone growth into a rat mandibular defect. Arch Oral Biol 48:155–160. doi:10.1016/S0003-9969(02)00172-3
Higgins JPT, Green S (2011) Cochrane handbook for systematic reviews of interventions version 5.1.0 [updated March 2011]. In: Cochrane Collab. p Table 7.7.a: formulae for combining groups
Hooijmans CR, Rovers MM, de Vries RBM et al (2014) SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol 14:43. doi:10.1186/1471-2288-14-43
Ashby ER, Rudkin GH, Ishida K, Miller TA (1996) Evaluation of a novel osteogenic factor, bone cell stimulating substance, in a rabbit cranial defect model. Plast Reconstr Surg 98:420–426
Bilkay U, Alper M, Celik N et al (2004) Comparing the osteogenic capacities of bone substitutes: hydroxyapatite, high-density porous polyethylene, and bone collagen: a biochemical and histological analysis. J Craniofac Surg 15:585–593
Calasans-Maia MD, Ascoli FO, Novellino ATNA et al (2009) Avaliação histológica comparativa de reparo ósseo em tíbia de coelho tratada com xenoenxertos. Acta Ortop Bras 17:340–343. doi:10.1590/S1413-78522009000600005
De Girolamo L, Arrigoni E, Stanco D et al (2011) Role of autologous rabbit adipose-derived stem cells in the early phases of the repairing process of critical bone defects. J Orthop Res 29:100–108. doi:10.1002/jor.21184
Klinge B, Alberius P, Isaksson S, Jönsson J (1992) Osseous response to implanted natural bone mineral and synthetic hydroxylapatite ceramic in the repair of experimental skull bone defects. J Oral Maxillofac Surg 50:241–249. doi:10.1016/0278-2391(92)90320-Y
Kucukkolbasi H, Mutlu N, Isik K et al (2009) Histological evaluation of the effects of bioglass, hydroxyapatite, or demineralized freeze-dried bone, grafted alone or as composites, on the healing of tibial defects in rabbits. Saudi Med J 30:329–333
Kühne JH, Bartl R, Frisch B et al (1994) Bone formation in coralline hydroxyapatite. Effects of pore size studied in rabbits. Acta Orthop Scand 65:246–252. doi:10.3109/17453679408995448
Lee SW, Kim SG, Balázsi C et al (2012) Comparative study of hydroxyapatite from eggshells and synthetic hydroxyapatite for bone regeneration. Oral Surg Oral Med Oral Pathol Oral Radiol 113:348–355. doi:10.1016/j.tripleo.2011.03.033
Lindholm TC, Gao TJ, Lindholm TS (1994) The role of autogeneic bone marrow in the repair of a skull trephine defect filled with hydroxyapatite granules in the rabbit. Int J Oral Maxillofac Surg 23:306–311. doi:10.1016/S0901-5027(05)80116-X
Abdul Razak NH, Al-Salihi KA, Samsudin AR (2004) An in vivo study of a locally-manufactured hydroxyapatite-based material as bone replacement material. Med J Malaysia 59(Suppl B):119–120
Sawada Y, Hokugo A, Yang Y et al (2011) A novel hydroxyapatite ceramic bone substitute transformed by ostrich cancellous bone: characterization and evaluations of bone regeneration activity. J Biomed Mater Res Part B Appl Biomater 98:217–222. doi:10.1002/jbm.b.31783
Turk AE, Ishida K, Jensen JA et al (1993) Enhanced healing of large cranial defects by an osteoinductive protein in rabbits. Plast Reconstr Surg 92:593–600
Zhou AJ-J, Clokie CML, Peel SAF (2013) Bone formation in algae-derived and synthetic calcium phosphates with or without poloxamer. J Craniofac Surg 24:354–359. doi:10.1097/SCS.0b013e318267ba3f
Andrade A, Sant’Ana D, Mendes Junior J et al (2013) Effects of cigarette smoke inhalation and coffee consumption on bone formation and osseous integration of hydroxyapatite implant. Braz J Biol 73:173–177. doi:10.1590/S1519-69842013000100018
Doll BA, Towle HJ, Hollinger JO et al (1990) The osteogenic potential of two composite graft systems using osteogenin. J Periodontol 61:745–750. doi:10.1902/jop.1990.61.12.745
Eftekhari H, Farahpour MR, Rabiee SM (2015) Histopathological evaluation of potential impact of beta-tricalcium phosphate (HA + beta-TCP) granules on healing of segmental femur bone defect. Bratisl Lek Listy 116:30–34
Hamerschmidt RR, dos Santos RF, Araújo JC et al (2011) Hydroxyapatite granules used in the obliteration of mastoid cavities in rats. Braz J Otorhinolaryngol 77:315–321
Moreira ASB, Pastoreli MT, Damasceno LHF, Defino HLA (2003) Estudo experimental da influência das dimensões dos grânulos de hidroxiapatita na integração óssea. Acta Ortopédica Bras 11:240–250. doi:10.1590/S1413-78522003000400007
Notodihardjo FZ, Kakudo N, Kushida S et al (2012) Bone regeneration with BMP-2 and hydroxyapatite in critical-size calvarial defects in rats. J Cranio-Maxillofacial Surg 40:287–291. doi:10.1016/j.jcms.2011.04.008
Park JW, Jang JH, Bae SR et al (2009) Bone formation with various bone graft substitutes in critical-sized rat calvarial defect. Clin Oral Implants Res 20:372–378. doi:10.1111/j.1600-0501.2008.01602.x
Rojbani H, Nyan M, Ohya K, Kasugai S (2011) Evaluation of the osteoconductivity of α-tricalcium phosphate, β-tricalcium phosphate, and hydroxyapatite combined with or without simvastatin in rat calvarial defect. J Biomed Mater Res Part A 98:488–498. doi:10.1002/jbm.a.33117
Sotto-Maior BS, Senna PM, Aarestrup BJV et al (2011) Effect of bovine hydroxyapatite on early stages of bone formation. Rev Odonto Ciência 26:198–292
Soccol AT, Bettega S, Noronha L et al (2006) Comparação entre os bioenxertos de hidroxiapatita de cálcio e submucosa de intestino delgado porcino no preenchimento de defeitos ósseos criados em mandíbula de ratos. Rev Bras Otorrinolaringol 72:195–199
Appleford MR, Oh S, Oh N, Ong JL (2009) In vivo study on hydroxyapatite scaffolds with trabecular architecture for bone repair. J Biomed Mater Res Part A 89:1019–1027. doi:10.1002/jbm.a.32049
Carvalho AL, Faria PEP, Grisi MFM et al (2007) Effect of granule size on the osteoconductivity of bovine and synthetic hydroxyapatite: a histologic and histometric study in dogs. J Oral Implantol 33:267–276. doi:10.1563/1548-1336(2007)33[267:EOGSOT]2.0.CO;2
Franco KL, Borges APB, Vilória MIV et al (2001) Hidroxiapatita sintética pura, hidroxiapatita sintética associada ao colágeno e hidroxiapatita sintética associada ao lipossoma como substitutos ósseos em defeitos provocados na tíbia de cães: aspectos da osteointegração à microscopia de luz transmitida. Arq Bras Med Vet e Zootec 53:431–436. doi:10.1590/S0102-09352001000400007
Lemperle SM, Calhoun CJ, Curran RW, Holmes RE (1998) Bony healing of large cranial and mandibular defects protected from soft-tissue interposition: a comparative study of spontaneous bone regeneration, osteoconduction, and cancellous autografting in dogs. Plast Reconstr Surg 101:660–672. doi:10.1097/00006534-199803000-00013
Buser D, Hoffmann B, Bernard JP, Lussi A, Mettler DSR (1998) Evaluation of filling materials in membrane protected bone defects. A comparative histomorphometric study in the mandible of miniature pigs. Clin Oral Implant Res 9:137–150
Thorwarth M, Wehrhan F, Srour S et al (2007) Evaluation of substitutes for bone: comparison of microradiographic and histological assessments. Br J Oral Maxillofac Surg 45:41–47. doi:10.1016/j.bjoms.2006.03.013
Reedy BK, Pan FH, Kim WS et al (1999) Properties of coralline hydroxyapatite and expanded polytetrafluoroethylene membrane in the immature craniofacial skeleton. Plast Reconstr Surg 103:20–26. doi:10.1097/00006534-199901000-00005
Houshmand B, Rahimi H, Ghanavati F et al (2007) Boosting effect of bisphosphonates on osteoconductive materials: a histologic in vivo evaluation. J Periodontal Res 42:119–123. doi:10.1111/j.1600-0765.2006.00923.x
Nandi SK, Kundu B, Ghosh SK et al (2008) Efficacy of nano-hydroxyapatite prepared by an aqueous solution combustion technique in healing bone defects of goat. J Vet Sci 9:183–191. doi:10.4142/jvs.2008.9.2.183
Celik EU, Sirin TC, Ergucu Z et al (2008) Can different chlorhexidine agents be used as cavity disinfectants? Gen Dent 56:e33–e37
Schmitz JP, Hollinger JO (1986) The critical size defect as an experimental model for craniomandibulofacial nonunions. Clin Orthop Relat Res. doi:10.1097/00003086-198604000-00036
LeGeros RZ (2008) Calcium phosphate-based osteoinductive materials. Chem Rev 108:4742–4753. doi:10.1021/cr800427g
Nandi SK, Kundu B, Mukherjee J et al (2015) Converted marine coral hydroxyapatite implants with growth factors: in vivo bone regeneration. Mater Sci Eng C Mater Biol Appl 49:816–823. doi:10.1016/j.msec.2015.01.078
Jun SH, Lee EJ, Jang TS et al (2013) Bone morphogenic protein-2 (BMP-2) loaded hybrid coating on porous hydroxyapatite scaffolds for bone tissue engineering. J Mater Sci Mater Med 24:773–782. doi:10.1007/s10856-012-4822-0
Xiao W, Fu H, Rahaman MN et al (2013) Hollow hydroxyapatite microspheres: a novel bioactive and osteoconductive carrier for controlled release of bone morphogenetic protein-2 in bone regeneration. Acta Biomater 9:8374–8383. doi:10.1016/j.actbio.2013.05.029
Hu J, Zhou Y, Huang L et al (2014) Effect of nano-hydroxyapatite coating on the osteoinductivity of porous biphasic calcium phosphate ceramics. BMC Musculoskelet Disord 15:114. doi:10.1186/1471-2474-15-114
Guo Y-P, Long T, Tang S et al (2014) Hydrothermal fabrication of magnetic mesoporous carbonated hydroxyapatite microspheres: biocompatibility, osteoinductivity, drug delivery property and bactericidal property. J Mater Chem B 2:2899–2909. doi:10.1039/c3tb21829e
Cooper GM, Mooney MP, Gosain AK et al (2010) Testing the critical size in calvarial bone defects: revisiting the concept of a critical-size defect. Plast Reconstr Surg 125:1685–1692. doi:10.1097/PRS.0b013e3181cb63a3
Gosain AK, Song L, Yu P et al (2000) Osteogenesis in cranial defects: reassessment of the concept of critical size and the expression of TGF-beta isoforms. Plast Reconstr Surg 106:360–371. doi:10.1097/00006534-200008000-00018
Frame JW (1980) A convenient animal model for testing bone substitute materials. J Oral Surg 38:176–180
Hollinger J, Kleinschmidt J (1990) The critical size defect as an experimental model to test bone repair materials. J Craniofac Surg 1:60–68. doi:10.1017/CBO9781107415324.004
Marsell R, Einhorn TA (2011) The biology of fracture healing. Injury 42:551–555. doi:10.1016/j.injury.2011.03.031
Loi F, Córdova LA, Pajarinen J et al (2016) Inflammation, fracture and bone repair. Bone 86:119–130. doi:10.1016/j.bone.2016.02.020
Roguska A, Hiromoto S, Yamamoto A et al (2011) Collagen immobilization on 316L stainless steel surface with cathodic deposition of calcium phosphate. Appl Surf Sci 257:5037–5045. doi:10.1016/j.apsusc.2011.01.018
Moura CCG, Souza MA, Dechichi P et al (2010) The effect of a nanothickness coating on rough titanium substrate in the osteogenic properties of human bone cells. J Biomed Mater Res, Part A 94A:103–111. doi:10.1002/jbm.a.32661
Lee Y-J, Ko JS, Kim H-M (2006) The role of cell signaling defects on the proliferation of osteoblasts on the calcium phosphate apatite thin film. Biomaterials 27:3738–3744. doi:10.1016/j.biomaterials.2006.02.032
Mills LA, Simpson AHRW (2012) In vivo models of bone repair. J Bone Joint Surg Br 94:865–874. doi:10.1302/0301-620X.94B7.27370
von Rechenberg B (2014) Animal models in bone repair. Drug Discov Today Dis Model 13:23–27. doi:10.1016/j.ddmod.2015.02.001
Kilkenny C, Browne WJ, Cuthill IC et al (2013) Improving bioscience research reporting: the arrive guidelines for reporting animal research. Animals 4:35–44. doi:10.3390/ani4010035
Acknowledgements
CECS wants to thank PRODEP/México for the scholarship.
Author information
Authors and Affiliations
Contributions
HLO, WLOR and EP designed the study. HLO and CECS prepared the first draft of the paper. NLVC, AFS, TNG and OAD contributed to the experimental work. WLOR was responsible for statistical analysis of the data. HLO, CECS, WLOR and EP prepared the final draft of the manuscript. All authors revised the paper critically for intellectual content and approved the final version. All authors agree to be accountable for the work and to ensure that any questions relating to the accuracy and integrity of the paper are investigated and properly resolved.
Funding
This study was financed by Coordination for the Improvement of Higher Education Personnel, CAPES/MEC-Brazil.
Corresponding author
Ethics declarations
Conflict of interest
Authors Héllen L. Oliveira, Wellington L. O. Rosa, Carlos E. Cuevas-Suárez, Neftali L. V. Carreño, Adriana F. Silva, Thomas N. Guim, Odir A. Dellagostin and Evandro Piva declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Oliveira, H.L., Da Rosa, W.L.O., Cuevas-Suárez, C.E. et al. Histological Evaluation of Bone Repair with Hydroxyapatite: A Systematic Review. Calcif Tissue Int 101, 341–354 (2017). https://doi.org/10.1007/s00223-017-0294-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-017-0294-z