
Abstract
Abnormalities of bone metabolism and increased vascular calcification are common in chronic kidney disease (CKD) and important causes of morbidity and mortality. The Wnt signaling pathway may play a role in the bone and vascular disturbances seen in CKD, termed collectively “CKD–MBD.” The aim of the study was to investigate the possible association of circulating concentrations of the secreted Wnt signaling inhibitors DKK1 and sclerostin with BMD and arterial stiffness in predialysis CKD. Seventy-seven patients (48 M, 29 F), mean age 57 (SD = 14) years with CKD stages 3B (n = 32) and 4 (n = 45) were studied. Sclerostin, DKK1, PTH, and 1,25(OH)2D were analyzed. BMD was measured at the lumbar spine (LS), femoral neck (FN), total hip (TH), and forearm (FARM). Arterial stiffness index was determined by contour analysis of digital volume pulse (SIDVP). There was a positive correlation between sclerostin and age (r = 0.47, p < 0.000). Sclerostin was higher in men than women (p = 0.013). Following correction for age and gender, there was a negative association between GFR and sclerostin (p = 0.002). We observed a positive association between sclerostin and BMD at the LS (p = 0.0001), FN (p = 0.004), and TH (p = 0.002). In contrast, DKK1 was negatively associated with BMD at the FN (p = 0.038). A negative association was seen between DKK1 and SIDVP (p = 0.027). Our data suggest that the Wnt pathway may play a role in CKD–MBD. Prospective studies are required to establish the clinical relevance of sclerostin and DKK1 as serological markers in CKD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Vascular calcification (VC) and bone/mineral disorders, described as chronic kidney disease (CKD) mineral bone disorder (MBD), are common findings in patients with CKD and are major causes of morbidity and mortality [1]. Increased VC is linked with vascular stiffness [2]. Both VC and arterial stiffness result in hypertension, left ventricular hypertrophy, ischemic heart disease and cardiovascular events, and reduced survival in this population [3].
Evidence over the last decade suggests a molecular link between the dysregulation in bone metabolism and the process of VC, although the mechanistic pathways involved are still incompletely understood [4]. VC is a complex process which involves cellular phenotypic changes from vascular smooth muscle cells (VSMCs) to mineralizing osteoblast-like cells. These cells are able to express several osteogenic genes such as the osteoblastic transcription factor, cbfa1/Runx2, bone morphogenetic protein 2 (BMP2), and Msx2 (a promoter of early osteoblast development) [5]. Evidence, derived mainly from animal models, also suggests that the Wnt signaling pathway may be implicated in the pathogenesis of VC [6]. Msx2-expressing cells promote VC, via the activation of Wnt signals. Canonical Wnts signal via the heterodimeric LDL receptor–related proteins LRP5 and LRP6 to stimulate osteogenic gene expression via nuclear β-catenin-dependent transcription [7]. To add further support to this hypothesis, several inhibitors of Wnt signaling, including secreted frizzled-related proteins (SFRPs 1, 2, and 4) have been shown to be overexpressed in areas of aortic calcification [8]. Furthermore, expression of Dickkopf-1 (DKK1, an inhibitor of the canonical Wnt pathway) is enhanced in advanced atherosclerotic lesions [9]. Sclerostin, another Wnt signaling inhibitor, has been shown to be upregulated during VSMC calcification in vitro [10]. Circulating DKK1 concentrations have been shown to be elevated in patients with angina compared to healthy controls, although this was not found when platelet-poor plasma was assayed [9]. However, the associations between circulating concentrations of the Wnt signaling inhibitors sclerostin and DKK1, different levels of renal function, and vascular stiffness in CKD, where extensive VC occurs, remains unknown.
The importance of Wnt signaling in the regulation of bone formation is well established and was first identified when loss-of-function mutations in LRP5 led to disorders associated with osteoporosis and gain-of-function mutations caused disorders of increased bone mass such as Van Buchem disease [11]. Sclerostin is expressed mainly in bone, primarily osteocytes [12]. Circulating concentrations of sclerostin have recently been associated with bone density in postmenopausal women [13, 14]. Circulating concentrations have been found to be higher in men and in postmenopausal women with osteoporosis and during immobility [14, 15]. In a recent study in CKD patients on dialysis, sclerostin was negatively correlated with histomorphometric parameters of bone turnover and osteoblast numbers, although DKK1 did not correlate with any histomorphometric parameter [16]. Abnormalities in DKK1 expression and concentrations have also been reported in bone disorders. Circulating DKK1 is negatively correlated with bone mineral density (BMD) [17], and higher concentrations have been reported in patients with lytic bone disease in multiple myeloma [18]. DKK1 is more widely expressed than sclerostin and has been implicated in colon cancer and rheumatoid arthritis [19, 20].
In light of the increasing evidence of a pathological link between bone abnormalities and VC/arterial stiffness in CKD, we hypothesized that a common regulatory pathway may involve the soluble Wnt signaling inhibitors sclerostin and DKK1. The aim of the study was to investigate the possible association of circulating concentrations of DKK1 and sclerostin with BMD and arterial stiffness in predialysis CKD.
Materials and Methods
Subjects
Seventy-seven ambulant predialysis patients (48 M, 29 F), mean age 57 (SD = 14) years, attending the renal unit with CKD stages 3B and 4 were recruited into this cross-sectional study during consecutive weekly renal outpatient clinics at Guy’s Hospital over 9 months. Informed written consent was obtained from each subject who participated in this study, in accordance with the Helsinki Declaration. The study was approved by the Research and Ethics Committee of Guy’s and St. Thomas’ NHS Trust. Patients were divided into two groups according to the severity of kidney disease based on the estimated glomerular filtration rate (eGFR), calculated using the MDRD formula [21]: group 1, eGFR 30–45 mL/min (CKD stage 3B); group 2, eGFR <30 mL/min (CKD stage 4). Exclusion criteria included patients who had a history of previous parathyroidectomy or recent hospital admissions (<1 month), were on renal replacement therapy, or were on or had previously received treatment with active vitamin D metabolites (1-alfacalcidol, calcitriol), phosphate binders, or bisphosphonates. The demographics and clinical details of the study population obtained from a questionnaire completed by all participants are summarized in Table 1. Routine biochemical analytes were measured immediately from random nonfasting blood, while additional serum samples were frozen and stored at −70 °C for subsequent analysis of DKK1 and sclerostin. At the renal clinic, blood pressure and digital volume pulse (DVP) were measured, and a dual-energy X-ray absorptiometric (DXA) scan was requested on all study participants to assess BMD at the total hip (TH), femoral neck (FN), lumbar spine (LS), and forearm (FARM).
Laboratory Measurements
Routine biochemical tests, such as serum creatinine, potassium, calcium, phosphate, albumin, total cholesterol, triglycerides, and HDL, were measured by standard laboratory methods on Roche Modular analyzers (Roche Diagnostics, Burgess Hill, UK). High-sensitivity C-reactive protein (CRP) was determined by particle-enhanced immunonephelometry (Dade Behring, Newark, DE) using the BN ProSpec analyser. Serum intact PTH was measured by electrochemiluminescence immunoassay on the Roche Elecsys 2010 analyzer (Roche Diagnostics, Indianapolis, IN). 25-Hydroxyvitamin D [25(OH)D] was measured by radioimmunoassay (RIA) (Diasorin, Stillwater, MN). Interassay coefficients of variation (CV) were 7.9 and 7.3 % at serum 25(OH)D of 40.4 and 131.8 nmol/L, respectively. Levels of 1,25(OH)2D were measured by RIA (IDS, Boldon, UK) as previously described [22].
Sclerostin was measured using a commercially available enzyme-linked immunosorbent assay (ELISA) (Biomedica Gruppe, Vienna, Austria) as previously reported [13]. The detection limit of the assay was 2.6 pmol/L, and the assay CV was 4.2 %. Serum DKK1 was measured by an ELISA (DuoSet ELISA; R&D Systems, Abingdon, UK) according to the manufacturer’s instructions and as used in previous studies [16, 18]. The 96-well microtiter plates were coated with 100 μL of anti-DKK1 monoclonal antibody diluted to 8.0 μg/mL. The detection antibody (goat anti-human DKK1) was diluted to a concentration of 100 μg/mL. The minimum detection limit was 631 pg/mL, and the assay CV was 1.45 % at a serum DKK1 concentration of 889 pg/mL.
BMD
DXA (Discovery-A QDR Series; Hologic, Waltham, MA, USA) was used to determine BMD of the TH, FN, LS, and FARM. The CV for BMD measurements of the TH, FN, and LS were 1.6, 2.5, and 1.6 %, respectively [23].
Arterial Stiffness Index
Contour analysis of DVP, which provides an index of large artery stiffness, was used to assess arterial stiffness as previously described [24]. DVP was measured by passing an infrared light through the finger pulp, which produces a typical waveform made up of a direct component and a reflected component. The pressure wave transmitted directly from the left ventricle to the finger produces the direct or systolic component, while the reflected or diastolic component is produced by the pressure wave transmitted along the aorta to small arteries in the lower limb, from where it is reflected back along the aorta to the finger. The stiffness index (SI) is given by the height of the individual divided by the time delay between the direct and reflected waves in the DVP. SI derived from the analysis of digital volume pulse (SIDVP) shows good correlation with pulse wave velocity (PWV), which is the gold standard and normally determined by carotid–femoral PWV (PWFcf) [25, 26]. SIDVP has also been associated with cardiovascular risk scores and shown to be useful in identifying high-risk populations [27]. The mean value of SIDVP was derived from a minimum of three measurements done on each study participant by the same investigator. Mean within-subject CV were 8 and 5 % at values of 4 and 10 m/s, respectively.
Statistical Analysis
Statistical calculations were performed using the standard statistical software package SPSS 17.0 for Windows (LEADTOOLS©; LEAD Technologies, Charlotte, NC, USA). Mean and SD were calculated for all continuous variables. Nonparametric data were log-transformed. Comparisons between groups were performed using Student’s t test for parametric data and the Mann–Whitney U test for nonparametric data. Univariate analyses were carried out using Pearson’s correlation coefficients or Spearman’s rank correlation. Multiple linear regression analysis was employed to explore the association between of DKK1 and sclerostin following correction for age, gender, eGFR, and independent variables selected following univariate analyses. Multiple linear regression analysis was also used to investigate the association of sclerostin and DKK1 with BMD and SIDVP. In all statistical analyses, p < 0.05 (95 % confidence interval) was considered to be statistically significant.
Results
The baseline laboratory parameters SIDVP and BMD (Z scores of TH, FN, LS, and FARM) of the study population are shown in Table 2. They were divided into two groups based on CKD stage: 3B and 4. There was no significant difference in serum calcium, phosphate, and 25(OH)D between the two groups. 1,25(OH)2D was significantly lower in patients with CKD stage 4 compared to stage 3B (p < 0.05). Serum CRP and PTH were significantly higher in patients with CKD stage 4 compared to stage 3B (p < 0.05). No significant difference was found in serum DKK1 and sclerostin between CKD stages 3B and 4.
Association of Sclerostin, DKK1, and Biochemical Parameters
In univariate analyses, serum sclerostin correlated positively with age (r = 0.47, p < 0.0001). Sclerostin was significantly higher in men (mean 50.5 pmol/L, SD = 30) compared to women (mean 34 pmol/L, SD = 15.8) (p = 0.015). No significant correlation was seen between DKK1 and sclerostin. Following correction for age and gender, sclerostin was negatively correlated with eGFR (Table 3). There was a significant negative correlation between DKK1 and 1,25(OH)2D (r = −0.270, p = 0.018), which did not remain after correction for age and gender. No significant correlation was observed between serum sclerostin or DKK1 with calcium, phosphate, 25(OH)D, and PTH.
Association between DKK1, Sclerostin, and BMD
There was no significant difference in BMD between the two groups (CKD stages 3B and 4), although the results tended to be lower in patients with CKD stage 4 (Table 2). Following univariate analyses, there was a significant positive correlation between BMD at the LS and sclerostin only (r = 0.33, p = 0.007) and no significant correlation between DKK1 and BMD at any site. Multiple linear regression analysis of BMD at the LS, FN, TH, and FARM as the dependent variable was carried out, following adjustment for confounders including age, gender, eGFR, BMI, physical activity, smoking habits, alcohol intake, previous fracture, and PTH. In this model, we found that sclerostin was positively associated with BMD at the FN (p = 0.004), TH (p = 0.002), and LS (p = 0.0001) (Table 4). In contrast, DKK1 was inversely associated with BMD at the FN (p = 0.038) (Table 4).
Association between DKK1, Sclerostin, and SIDVP
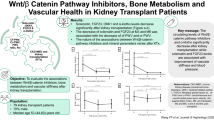
SIDVP did not differ significantly between patients with CKD stages 3B and 4 (Table 2). In univariate analyses of the whole study population, a significant inverse correlation was observed between SIDVP and DKK1 (r = −0.287, p = 0.013), as illustrated in Fig. 1. No significant correlation was found between SIDVP and sclerostin. SIDVP correlated significantly with age (r = 0.276, p = 0.017), systolic blood pressure (r = 0.242, p = 0.038), diastolic blood pressure (r = 0.270, p = 0.021), and total cholesterol (r = 0.227, p < 0.05). Following correction for age, gender, eGFR, diastolic blood pressure, total cholesterol, triglycerides, CRP, and HDL, DKK1 remained a significant negative predictor of SIDVP (p = 0.027). The results are shown in Table 5. This model explained 33 % of the variance in SIDVP.

Correlation between DKK1 and arterial stiffness (SIDVP). Increases in SIDVP are linked with lower DKK1 concentrations
Discussion
This study demonstrates that sclerostin is positively associated with BMD at the hip and lumbar spine in CKD stages 3B and 4, confirming similar findings in hemodialysis patients [28]. In contrast, we observed for the first time a negative association between DKK1 and BMD at the femoral neck. Further, DKK1 was negatively associated with SIDVP.
We observed increases in serum sclerostin in men compared to women and as a function of age as previously reported [13, 28]. Our data demonstrate that the increase in sclerostin with age is also seen in patients with CKD and may mainly reflect changes in sclerostin production with generalized aging. The mechanism of increases in sclerostin in the elderly remains uncertain but may be a consequence of imbalances in skeletal remodeling seen with aging. Whether the elevations in sclerostin with age lead to impairment in bone formation or effects on bone resorption via its effects on the OPG/RANKL/RANK pathway remains to be clarified. Indeed, data from animal studies implicate the Wnt/B-catenin signaling pathways in the regulation of OPG and RANKL [29]. The association was independent of GFR, suggesting that the increases in sclerostin are unlikely to be due merely to reduced renal clearance but may reflect, at least in part, increased production by osteocytes. Higher sclerostin concentrations were observed in men, as previously documented [13, 28], which may reflect larger bone mass in men. A strong negative association was observed between GFR and sclerostin, following correction for age and gender. High sclerostin concentrations have been observed with profoundly abnormal renal function in patients receiving dialysis. This is related mainly to accumulation due to renal impairment, although abnormalities in bone and mineral metabolism may also contribute to some extent [28].
In contrast, DKK1 was not affected by age, gender, or renal function [28]. There was a small but significant negative correlation between 1,25(OH)2D and DKK1, although this was no longer significant when corrected for age, gender, and GFR. DKK1 has previously been shown to be differentially regulated in a tissue-specific manner by 1,25(OH)2D in in vitro studies of human colon cells [30] and murine bone marrow stromal cells [31]. In bone marrow stromal cells, 1,25(OH)2D suppresses DKK1, which could explain, at least in part, the observed small negative association between 1,25(OH)2D and DKK1 in the study population. In our study there was no association between PTH and DKK1, as observed previously in CKD stage 5D (dialysis). The lack of association between PTH and sclerostin seen in our study is, however, different from the findings of other studies [16, 28], which have shown a negative correlation between PTH and sclerostin in CKD stage 5D. Our study is the first to examine these issues in a nondialyzed cohort of renal patients with better preservation of kidney function and, thus, a wider range of renal function and CKD–MBD abnormalities. The negative relationship between sclerostin and PTH has also been demonstrated in some, but not all, studies of patients treated with intermittent PTH [14, 32] and in primary hyperparathyroidism, which normalizes postparathyroidectomy [33, 34]. The lack of association in predialysis CKD may be explained by differences in the study population in terms of the degree of renal impairment or the degree of skeletal resistance to PTH in CKD.
The relationship between circulating sclerostin and bone mass is perplexing. As sclerostin is an inhibitor of bone formation, one would expect to see a negative correlation between this Wnt inhibitor and bone density. However, several studies have now reported a positive relationship between sclerostin and bone density in postmenopausal women and in CKD stage 5D [13, 14, 28]. Our data extend this observation for the first time to patients with predialysis CKD as we found that sclerostin was a significant independent predictor of BMD at the femoral neck, hip, and lumbar spine. One explanation for our findings is that as sclerostin is primarily produced by late osteoblasts and osteocytes, its production may therefore be a direct reflection of bone cell numbers and activity, although other factors such as level of physical activity or age, as discussed above, could also contribute [13, 15]. However, whether circulating sclerostin as measured by the currently available immunoassays is biologically active remains to be elucidated. We observed a negative correlation between circulating DKK1 and BMD at the femoral neck. This is in contrast to other studies in CKD stage 5D, where DKK1 was found to be unrelated to bone measures and did not seem to influence bone status [16, 28]. Our finding of a negative correlation between DKK1 and BMD in predialysis CKD is biologically plausible as it is an inhibitor of bone formation. Indeed, a previous small cross-sectional study showed that serum DKK1 was increased in patients with osteoporosis and correlated negatively with BMD at the lumbar spine and femur [17]. Furthermore, DKK1 has been implicated in myeloma bone disease, where increased concentrations are associated with increases in lytic lesions and reduction in bone formation [18]. The discrepant association seen between DKK1 and sclerostin with BMD may be explained, at least partly, by the differences in tissue distribution of the two Wnt signaling inhibitors. One explanation is that DKKI, unlike sclerostin, is produced not only by the skeleton but also by other tissues implicated in CKD–MBD, such as platelets and vascular cells. Therefore, circulating concentrations of DKK1 may not depend, solely, on skeletal production. However, as DKK1 is a secreted protein, we can speculate that its extraskeletal production can contribute to circulating concentrations, which could in turn have a negative impact on the skeleton. Moreover, DKK1 seems unaffected by renal clearance. Another, more hypothetical explanation of the differences between BMD and the two Wnt inhibitors is that extraskeletal production of DKK1 may have an impact on sclerostin production and/or function as both factors bind to LRP5 and LRP6 to inhibit Wnt signaling.
In addition to its important role in bone remodelling, DKK1 may be implicated in the pathogenesis of VC, a component of CKD–MBD. Indeed, we observed a negative relationship between SIDVP (a surrogate marker of arterial stiffness) and DKK1, suggesting that lower circulating concentrations may lead to a reduction in vascular compliance, presumably due to increases in VC. VC is subject to active osteogenic regulation, which includes BMP2-Msx2 osteogenic signaling pathways [5]. Recent evidence in animal studies suggests than Wnt ligands are upregulated, while Wnt antagonists such as DKK1 are downregulated [6]. On the other hand, other studies have shown increased expression of DKK1 in advanced carotid plaques [9] or, indeed, other Wnt inhibitors such as SFRPs 1, 2, and 4 in severely calcified aortas [8]. It has been suggested that this may be a defensive response, in cases where VC is well established and severe, to block the Wnt pathway in order to reduce ossification and avoid further progression [8]. Taken together these findings, including those of our study, implicate DKK1 in the vascular integrity in CKD. Whether changes in DKK1 are of direct pathological significance or a secondary response remains to be established, but as both VC and vascular stiffness have major impacts on the survival of patients with CKD, this requires further investigations. DKK1 has been shown to be involved in the inflammatory interaction between platelets and endothelial cells, thought to be an important mechanistic pathway in atherogenesis [9]. The use of DKK1 as a serological marker of VC and arterial stiffness in particular merits further studies. We did not observe any association between circulating sclerostin and SIDVP, although expression of sclerostin is upregulated during calcification of VSMCs [10]. However, this may be a local process and may not influence circulating concentrations.
In conclusion, we have shown that the recently reported positive relationship between circulating sclerostin with age and bone mass is also seen in patients with predialysis CKD. Circulating sclerostin is higher in men and is affected, in part, by renal clearance. In contrast, DKK1 was negatively associated with bone mass and arterial stiffness, suggesting a role for this Wnt inhibitor in CKD–MBD. However, an important limitation of our cross-sectional study is that we cannot establish a causal effect of the Wnt signaling inhibitors in the regulation of bone mass and arterial stiffness in predialysis CKD. Nevertheless, our findings are of interest and suggest that the Wnt signaling pathway may be involved in the pathogenesis of CKD–MBD. Further, larger, prospective studies are needed to establish the clinical relevance of sclerostin and DKK1 as serological markers in CKD–MBD.
References
Cannata-Andia JB, Rodriguez-Garcia M, Carrillo-Lopez N, Naver-Diaz M, Diaz-Lopez B (2006) Vascular calcifications: pathogenesis, management and impact on clinical outcomes. J Am Soc Nephrol 17:S267–S273
London GM, Marchais SJ, Guerin AP, Metivier F (2002) Impairment of arterial function in chronic kidney disease: prognostic impact and therapeutic approach. Nephrol Dial Transplant 17(Suppl 11):13–15
Shao JS, Cheng SL, Sadhu J, Towler DA (2010) Inflammation and the osteogenic regulation of vascular calcification: a review and perspective. Hypertension 55:579–592
Sage AP, Tintut Y, Demer LL (2010) Regulatory mechanisms in vascular calcification. Nat Rev Cardiol 7:528–536
Shao JS, Cai J, Towler DA (2006) Molecular mechanisms of vascular calcification: lessons learned from the aorta. Arterioscler Thromb Vasc Biol 26:1423–1430
Towler DA, Shao JS, Cheng SL, Pingsterhaus JM, Loewy A (2006) Osteogenic regulation of vascular calcification. Ann NY Acad Sci 1068:327–333
Shao JS, Cheng SL, Pingsterhaus JM, Charlton-Kachigian N, Loewy AP, Towler DA (2005) Msx2 promotes cardiovascular calcification by activating paracrine Wnt signals. J Clin Invest 115:1210–1220
Román-García P, Carrillo-López N, Fernández-Martín JL, Naves-Díaz M, Ruiz-Torres MP, Cannata-Andía JB (2010) High phosphorus diet induces vascular calcification, a related decrease in bone mass and changes in the aortic gene expression. Bone 46(1):121–128
Ueland T, Otterdal K, Lekva T, Halvorsen B, Gabrielsen A, Sandberg WJ, Paulsson-Berne G, Pedersen TM, Folkersen L, Gullestad L, Oie E, Hansson GK, Aukrust P (2009) Dickkopf-1 enhances inflammatory interaction between platelets and endothelial cells and shows increased expression in atherosclerosis. Arterioscler Thromb Vasc Biol 29(8):1228–1234
Zhu D, Mackenzie NC, Millán JL, Farquharson C, MacRae VE (2011) The appearance and modulation of osteocyte marker expression during calcification of vascular smooth muscle cells. PLoS One 6(5):e19595
Baron R, Rawadi G (2007) Targeting the Wnt/beta-catenin pathway to regulate bone formation in the adult skeleton. Endocrinology 148(6):2635–2643
Winkler DG, Sutherland MK, Geoghegan JC, Yu C, Hayes T, Skonier JE, Shpektor D, Jonas M, Kovacevich BR, Staehling-Hampton K, Appleby M, Brunkow ME, Latham JA (2003) Osteocyte control of bone formation via sclerostin, a novel BMP antagonist. EMBO J 22(23):6267–6276
Mödder UI, Hoey KA, Amin S, McCready LK, Achenbach SJ, Riggs BL, Melton LJ III, Khosla S (2011) Relation of age, gender, and bone mass to circulating sclerostin levels in women and men. J Bone Miner Res 26(2):373–379
Polyzos SA, Anastasilakis AD, Bratengeier C, Woloszczuk W, Papatheodorou A, Terpos E (2012) Serum sclerostin levels positively correlate with lumbar spinal bone mineral density in postmenopausal women—the six-month effect of risedronate and teriparatide. Osteoporos Int 23(3):1171–1176
Gaudio A, Pennisi P, Bratengeier C, Torrisi V, Lindner B, Mangiafico RA, Pulvirenti I, Hawa G, Tringali G, Fiore CE (2010) Increased sclerostin serum levels associated with bone formation and resorption markers in patients with immobilization-induced bone loss. J Clin Endocrinol Metab 95(5):2248–2253
Cejka D, Herberth J, Branscum AJ, Fardo DW, Monier-Faugere MC, Diarra D, Haas M, Malluche HH (2011) Sclerostin and Dickkopf-1 in renal osteodystrophy. Clin J Am Soc Nephrol 6(4):877–882
Butler JS, Murray DW, Hurson CJ, O’Brien J, Doran PP, O’Byrne JM (2011) The role of Dkk1 in bone mass regulation: correlating serum Dkk1 expression with bone mineral density. J Orthop Res 29(3):414–418
Kaiser M, Mieth M, Liebisch P, Oberländer R, Rademacher J, Jakob C, Kleeberg L, Fleissner C, Braendle E, Peters M, Stover D, Sezer O, Heider U (2008) Serum concentrations of DKK1 correlate with the extent of bone disease in patients with multiple myeloma. Eur J Haematol 80(6):490–494
Pendás-Franco N, Aguilera O, Pereira F, González-Sancho JM, Muñoz A (2008) Vitamin D and Wnt/beta-catenin pathway in colon cancer: role and regulation of DICKKOPF genes. Anticancer Res 28(5A):2613–2623
Diarra D, Stolina M, Polzer K, Zwerina J, Ominsky MS, Dwyer D, Korb A, Smolen J, Hoffmann M, Scheinecker C, van der Heide D, Landewe R, Lacey D, Richards WG, Schett G (2007) Dickkopf-1 is a master regulator of joint remodeling. Nat Med 13(2):156–163
Archibald G, Bartlett W, Brown A, Christie B, Elliott A, Griffith K, Pound S, Rappaport I, Robertson D, Semple Y, Slane P, Whitworth C, Williams B (2007) UK Consensus Conference on early chronic kidney disease—6 and 7 February 2007. Nephrol Dial Transplant 22(9):2455–2457
Joseph F, Ahmad AM, Ul-Haq M, Durham BH, Whittingham P, Fraser WD, Vora JP (2008) Effects of growth hormone administration on bone mineral metabolism, PTH sensitivity and PTH secretory rhythm in postmenopausal women with established osteoporosis. J Bone Miner Res 23(5):721–729
Patel R, Blake GM, Rymer J, Fogelman I (2000) Long-term precision of DXA scanning assessed over seven years in forty postmenopausal women. Osteoporos Int 11(1):68–75
Manghat P, Souleimanova I, Cheung J, Wierzbicki AS, Harrington DJ, Shearer MJ, Chowienczyk P, Fogelman I, Goldsmith D, Hampson G (2011) Association of bone turnover markers and arterial stiffness in pre-dialysis chronic kidney disease (CKD). Bone 48(5):1127–1132
Millasseau SC, Kelly RP, Ritter JM, Chowienczyk PJ (2002) Determination of age-related increases in large artery stiffness by digital pulse contour analysis. Clin Sci (Lond) 103(4):371–377
Sollinger D, Mohaupt MG, Wilhelm A, Uehlinger D, Frey FJ, Eisenberger U (2006) Arterial stiffness assessed by digital volume pulse correlates with comorbidity in patients with ESRD. Am J Kidney Dis 48(3):456–463
Gunarathne A, Patel JV, Hughes EA, Lip GY (2008) Measurement of stiffness index by digital volume pulse analysis technique: clinical utility in cardiovascular disease risk stratification. Am J Hypertens 21(8):866–872
Cejka D, Jäger-Lansky A, Kieweg H, Weber M, Bieglmayer C, Haider DG, Diarra D, Patsch J, Kainberger F, Bohle B, Haas M (2012) Sclerostin serum levels correlate positively with bone mineral density and microarchitecture in haemodialysis patients. Nephrol Dial Transplant 27(1):226–230
Kearns AE, Khosla S, Kosteniuk PJ (2008) Receptor activator of nuclear factor-κB ligand and osteoprotegerin regulation of bone remodelling in health and disease. Endocr Rev 29:155–192
Aguilera O, Peña C, García JM, Larriba MJ, Ordóñez-Morán P, Navarro D, Barbáchano A, López de Silanes I, Ballestar E, Fraga MF, Esteller M, Gamallo C, Bonilla F, González-Sancho JM, Muñoz A (2007) The Wnt antagonist DICKKOPF-1 gene is induced by 1alpha,25-dihydroxyvitamin D3 associated to the differentiation of human colon cancer cells. Carcinogenesis 28(9):1877–1884
Cianferotti L, Demay MB (2007) VDR-mediated inhibition of DKK1 and SFRP2 suppresses adipogenic differentiation of murine bone marrow stromal cells. J Cell Biochem 101(1):80–88
Drake MT, Srinivasan B, Mödder UI, Peterson JM, McCready LK, Riggs BL, Dwyer D, Stolina M, Kostenuik P, Khosla S (2010) Effects of parathyroid hormone treatment on circulating sclerostin levels in postmenopausal women. J Clin Endocrinol Metab 95(11):5056–5062
van Lierop AH, Witteveen JE, Hamdy NA, Papapoulos SE (2010) Patients with primary hyperparathyroidism have lower circulating sclerostin levels than euparathyroid controls. Eur J Endocrinol 163(5):833–837
Ardawi MS, Al-Sibiany AM, Bakhsh TM, Rouzi AA, Qari MH (2011) Decreased serum sclerostin levels in patients with primary hyperparathyroidism: a cross-sectional and a longitudinal study. Osteoporos Int
Acknowledgments
This work was supported by a small grant from the Friends of Guy’s Hospital, London, UK.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have stated that they have no conflict of interest.
Rights and permissions
About this article
Cite this article
Thambiah, S., Roplekar, R., Manghat, P. et al. Circulating Sclerostin and Dickkopf-1 (DKK1) in Predialysis Chronic Kidney Disease (CKD): Relationship with Bone Density and Arterial Stiffness. Calcif Tissue Int 90, 473–480 (2012). https://doi.org/10.1007/s00223-012-9595-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-012-9595-4