
Abstract
We studied 12 patients with Parkinson’s disease (PD): 6 with postural instability (Hoehn and Yahr Stage 3) and 6 without (Stage 2 or 2.5), using a quantitative test based on the clinical pull test. Their findings were compared with those for 12 healthy controls. The patients on their usual medications were pulled either forwards or backwards at the level of the shoulders and asked not to take a step in a series of five trials. Acceleration was monitored for the upper trunk, sacrum, and both tibias. EMG was measured in soleus and tibialis anterior (TA) muscles in all and for thigh and truncal muscles in a subgroup. A target of 0.2 g trunk acceleration was used, but smaller perturbations were used in very unstable patients. All the Stage 3 patients lost balance in at least one trial for the posterior perturbations but none for the anterior ones. None of the Stage 2 patients lost balance. There was increased tonic EMG and agonist activity but no difference in EMG onset or initial force production compared to healthy controls. For posterior perturbations, there were two related disorders that separated the PD patients from controls. There was a significantly higher ratio of sacral-to-applied acceleration and both PD groups showed reduced knee acceleration and shortened latency, more so for the Stage 3 group. The increased sacral-to-C7 acceleration ratio was correlated with the tonic level of activation of the hamstrings (HS), quadriceps, and lumbar paraspinal muscles (PS), while the tibial acceleration latency was also correlated with the level of tonic PS activation. We also found that the size of balance responses, 0–200 ms post-perturbation, correlated significantly with the level of tonic activation in nearly all the muscles studied. We confirmed that PD patients show greater instability posteriorly than anteriorly to applied perturbations. Our findings support increasing axial and limb rigidity as the cause of the impaired pull test rather than postural bradykinesia and suggest that tonic truncal and thigh muscle activation may be an important underlying cause.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The development of postural instability in Parkinson’s disease (PD) defines the onset of Hoehn and Yahr Stage III, a phase in which significant disability is generally accepted to occur (Hoehn and Yahr 1967; Munhoz and Teive 2014). Accidental falls are the key consequences of postural instability and lead to injury (Koller et al. 1989; Bloem et al. 2004; Grimbergen et al. 2004; Wielinski et al. 2005). Assessment requires the use of postural disturbances to assess stability (Bloem et al. 2001; Visser et al. 2003; Nonnekes et al. 2015). As described in their report, impairment of righting reflexes was determined by pushing the standing subject (Hoehn and Yahr 1967), whereas Charcot, for example, pulled on the patient’s clothes to demonstrate retropulsion (Goetz 1986). Clinical assessment of postural stability in PD is now usually based on the Pull Test (Hunt and Sethi 2006) and abnormalities on this test have been shown to predict falls (Kataoka et al. 2011). In this test, the patient is pulled backwards at the level of the shoulders, forcefully enough to require one or more steps to compensate. However, the test is difficult to standardise. Munhoz et al. (2004) found that it was common for examiners to pull too lightly. Done carefully, the pull test has a good correlation with the likelihood of falls (Munhoz and Teive 2014).
We have developed a test of postural stability based on the clinical pull test, but one in which the applied perturbation is monitored and standardised (Colebatch et al. 2016). Like the clinical test, the force was applied manually to the upper trunk, but subjects were required not to take a step. We have applied the perturbations both forwards and backwards. The result is a stereotyped group of muscle contractions, with the initial short latency EMG response occurring before a voluntary reaction time (Colebatch and Govender 2018). The findings are little affected by the presence of vision. In this study, we have applied this method to two groups of PD patients one with clinically impaired postural reflexes and one without, and have compared their findings with those of healthy controls, to understand better the changes underlying their postural impairment.
Materials and methods
Patient and normal cohorts
In 12 PD patients (Table 1), half of whom had clinically impaired responses to the pull (-back) test were recruited and tested for this study. The first group required stabilisation on posterior perturbation testing (PD group 1: 69 ± 14 years; 5 males, 1 female) and the other did not (PD group 2: 70 ± 10 years; 5 males, 1 female). All patients were under the care of one of the authors (J.G.C). All met UK Parkinson’s Disease Society Brain Bank criteria (Hughes et al. 1992) for the diagnosis of idiopathic PD and showed definite responses to dopaminergic medication. One patient (P4, 85-year-old female) subsequently came to post-mortem and was pathologically confirmed to have Parkinson’s disease. She had severe instability and her results are referred to specifically at times. The PD patients were tested on their usual medication while standing without assistance. A postural perturbation was applied manually by the experimenter to the upper trunk similar to the method used clinically but with the experimenter able to see a record of the acceleration imparted to the subject at the end of each trial. Healthy controls and PD patients were told not to take a step unless they were going to fall. The perturbations were strong enough, of the order of 40 N, such that they required a conscious response to avoid falling. The patient findings were compared to those for older normal controls (12 subjects, 65 ± 11 years, 7 females, 5 males). Informed consent was given before the experiments, in accordance with the Declaration of Helsinki, and this study was approved by the local ethics committee (South Eastern Sydney Local Health District Human Research Ethics Committee).
Recording equipment
Subjects and patients stood on a force platform (model 9286A, Kistler Instrumente, Winterthur, Switzerland) with their feet comfortably apart, with their feet over a template. Centre of Pressure (CoP) for the anterior–posterior (AP) axis and vertical (Z) force were calculated from the transducer outputs using the manufacturer’s formula. The Z gradient (rate of rise of force, anterior–posterior) was measured over 100–200 ms and 200–500 ms post-onset of the perturbation. Uniaxial accelerometers (model 751-100, Endevco, California, USA) were used to record evoked accelerations of the upper trunk, sacrum, and lower limbs (knees), and were placed on the trunk (C7; n = 12), the sacrum (n = 11), and over the tibial tuberosities (n = 9). Surface EMG potentials were recorded using adhesive electrodes (Cleartrace 1700-030, Conmed Corp., NY, USA). Unilateral recordings were made in 7 patients (P2, P4, and P5 from PD group 1; P7, P8, P11, and P12 from PD group 2) from soleus, tibialis anterior (TA), hamstrings (HS), quadriceps (Quad), lumbar paraspinal (PS), and rectus abdominis (RA) muscle groups (n = 2 right, n = 5 left). Detailed descriptions of electrode locations for each muscle have been previously published (see Colebatch et al. 2016). Inter-electrode distances were 2–3 cm. For convenience, bilateral recordings were made from soleus and TA muscles in the remaining patients and averaged between sides. An earth electrode was placed on the left forearm approximately 5 cm distal to the antecubital fossa. EMG was amplified (1000 or 2500×, D360 Digitimer Co, Welwyn Garden City, UK), band-pass filtered (8 Hz–1.6 kHz). All data were sampled at 4 kHz using a Power1401 and SIGNAL software (Cambridge Electronic Design, Cambridge, UK) for a total of 5 s and realigned prior to averaging off line as described below.
Perturbation stimuli
Rapid, unpredictable perturbations were applied by one experimenter (S.G.) to displace the subjects, whose eyes were open, either forwards or backwards. The same experimenter applied similar perturbations for the normal controls. Perturbations were delivered by holding the subject at the shoulders and pulling the trunk in the anterior (pull-forward) or posterior (pull-back) directions. Neither healthy controls nor PD patients were told when the perturbations would be delivered and both were instructed to attempt to maintain their upright posture without moving their feet. A target of 0.2 g peak acceleration was used, but lower peak accelerations were used in the patients with marked postural instability for their safety. We have previously found that normal controls are able to maintain their posture in response to similar perturbations (Colebatch et al. 2016). An abnormal result was, therefore, defined as the experimenter needing to stabilise the patient to prevent falling for one or more of the five individual perturbation trials delivered. A familiarisation trial was performed and then five individual perturbations were recorded for each direction. Each trial was originally 5 s in total duration with a 1.5 s pre-stimulus interval. The recording of EMG, CoP, and acceleration data was triggered by the experimenter pressing a footswitch at approximately the same time as the applied perturbation. For each individual perturbation, the traces were realigned offline to the onset of acceleration as detected at C7 which was defined as time 0 and, during the same process, EMG was full wave rectified and averaged. This process reduced the length of the recordings to 1 s prior to the new reference and 3 s following it, and was done using custom scripts written in the MATLAB software (Matlab 2007b Mathworks, MA; Colebatch et al. 2016). The averaged recordings were then used for data analysis. Mean-rectified EMG levels were automatically measured for a series of 9 time intervals (baseline, 0–0.2 s, 0.2–0.5 s, 0.5–0.75 s, 0.75–1 s, 1–1.5 s, 1.5–2 s, 2–2.5 s, and 2.5–3 s). For EMG onset latencies, values were determined from rectified EMG using a cumulative sum technique requiring 3 SD deviations remaining consistently above or below from the preceding mean activity levels (Colebatch et al. 2016). Grand averages of each of the three groups were made and used as an indication of the latencies of the important peaks for acceleration and CoP. These values, in turn, were used to guide the manual selection of latencies using the individual recordings. Voluntary contractions were measured during sitting, while PD patients and controls were asked to maximally dorsiflex (TA) and plantar flex (soleus). Mean-rectified EMG levels during voluntary contraction were taken over approximately 1 s.
Statistical analysis
For anterior perturbations, data for both PD groups were combined for subsequent analyses as acceleration, CoP, and EMG profiles did not differ between the two PD groups. Unpaired Student’s t tests were used for amplitude and latency comparisons between groups for acceleration, COP, and EMG onset measurements, and when comparing rates of rise of vertical (Z) force. A repeated-measures ANOVA was carried out using EMG intervals as the within-subjects factor and group (PD group 1, group 2, and healthy controls) as the between-subjects factor for the TA and soleus muscle groups for posterior perturbations. Log-transformed EMG values were used during ANOVA testing to ensure normality (Shapiro–Wilk test). We specifically examined the initial 0–200 ms post-perturbation EMG interval as this period corresponds to balance responses (Bloem et al. 2000) and it is likely that changes in this earliest interval would most strongly affect the subjects’ abilities to maintain upright posture in response to a sudden displacement. EMG levels at 0–100 ms and 100–200 ms post-perturbation intervals in TA and soleus were compared using unpaired Student’s t tests. Linear regression was used to investigate the dependence of sacral-to-truncal acceleration ratios, tibial acceleration amplitude and latency, and balance responses (tonic activity 0–200 ms post-onset of acceleration) upon baseline pre-stimulus EMG levels using data from PD patients and controls.
Results in the text and tables are given as mean ± SD, unless stated otherwise. Graphs depict data as mean ± SEM. The P < 0.01 was taken as the threshold for significance due to the number of groups and comparisons. P values between 0.01 and 0.05 are also given in the text, along with trends between 0.05 and 0.1.
Results
The body mass index (BMI) was not significantly different between healthy controls and PD patients (PD group 1 vs controls: 27.2 vs 24.9 kg/m2; t(16) = 1.4, P = 0.19; PD group 2 vs controls: 28.5 vs 24.9 kg/m2; t(16) = 1.4, P = 0.19). The Levodopa equivalent daily dose (LEDD) was significantly greater for PD group 1 than PD group 2 (Table 1: t(10) = 5.2, P < 0.001). The duration of disease was not significantly different between the groups (t(10) = 1.0, P = 0.32). In PD group 1, patients (P4) and (P5) required stabilisation by the experimenter (S.G) for all five individual trials following posterior macro-perturbations. Support by the experimenter was required for patients (P3) and (P1) for two trials, and for patients (P2), and (P6) for one trial following posterior perturbations. None of the PD group 1 patients required stabilisation following anterior perturbations. None of the healthy controls or any PD group 2 patients required stabilisation for either direction of perturbation.
Voluntary maximal contractions were recorded in 11 healthy controls and were 74.9 ± 50.3 µV (TA) and 58.7 ± 25.4 µV (soleus), while six PD patients (P1, P3–5, P8, and P9) had maximal contraction of 124.4 ± 48.2 µV (TA) and 80.3 ± 54.1 µV (soleus). Maximal contraction tended to be larger for TA in PD patients (t(15) = 2.0, P = 0.07), but did not differ between groups for soleus (t(15) = 1.1, P = 0.27).
Posterior perturbations (pull backwards)
Peak-induced acceleration amplitudes at the trunk were significantly smaller in PD group 1 patients than in healthy controls (t(16) = 2.8, P = 0.01), probably due to the patients’ instability prompting weaker pulls (Fig. 1, Table 2). In contrast, peak acceleration amplitudes at the trunk were not different between PD group 2 and healthy controls (Table 3; t(16) = 1.3, P = 0.22). As sacral accelerations were similar, the ratio of sacral-to-truncal accelerations in PD group 1 patients was higher than that of healthy controls (PD group 1 vs controls: 0.57 ± 0.20 vs 0.35 ± 0.13; t(16) = 2.7, P = 0.02). PD group 2 also showed an increase in the sacral-to-truncal ratio (PD group 2 vs controls: 0.51 ± 0.12 vs 0.35 ± 0.13; t(15) = 2.3, P = 0.04). The ratio of sacral-to-truncal accelerations was not significantly different between the two PD groups (t(9) = 0.5, P = 0.60), whereas both PD groups combined were significantly greater than controls (PD groups combined vs controls: 0.54 ± 0.17 vs 0.35 ± 0.13; t(21) = 3.0, P = 0.007). The two PD patients (P4, P5) with the most frequent loss of balance had average sacral/truncal ratios of 0.69.

Grand mean responses (PD group 1—left column; PD group 2—right column) showing recordings of acceleration, EMG and CoP following posterior perturbations. Upward accelerations reflect anterior (forward) movement. Due to their instability, several PD group 1 patients had smaller applied perturbations than controls, leading to a lower average level of acceleration of the trunk. Despite this, sacral acceleration was similar. Tibial accelerations also show differences between PD groups and controls. The initial anterior acceleration seen in the controls was attenuated for the both PD groups. There were higher tonic levels of EMG activity in HS and Quadriceps particularly for PD group 1 patients. Initial TA EMG levels and CoP changes were similar although with a more prolonged contraction of TA in the PD group 1 patients. TA tibialis anterior, Sol soleus, HS hamstrings, QUAD quadriceps, RA rectus abdominis, PS lumbar paraspinal muscles, CoP centre of pressure
The peak latency of truncal acceleration, sacral acceleration (peak amplitude and latency), and CoP (peak amplitude and onset latency) were not significantly different between either PD group and healthy controls (PD group 1 vs controls: t(16) = 0.1–1.6, P = 0.13–0.96; PD group 2 vs controls: t(15–16) = 0.6–2.0, P = 0.06–0.58). CoP peak latencies were significantly delayed in PD group 1 patients (PD group 1 vs controls: 791.6 vs 438.4 ms; t(16) = 3.5, P = 0.003), but were not significantly different between PD group 2 and healthy controls (t(16) = 0.9, P = 0.36). When comparing between PD groups, CoP peak latencies tended to be later in PD group 1 than PD group 2 (t(10) = 2.4, P = 0.04).
Healthy controls showed a prominent anterior acceleration at the tibias, consistent with knee flexion, which was earlier and attenuated in the PD patients (Tables 2, 3). In PD group 1, L- and R- averaged peak initial tibial accelerations were smaller (t(15) = 2.3, P = 0.03) and earlier (t(15) = 4.2, P < 0.001) compared to healthy controls. PD group 2 patients showed a trend towards smaller tibial accelerations than controls (t(14) = 1.9, P = 0.08), but initial peak tibial latencies were not significantly different (t(14) = 1.2, P = 0.21). When comparing between PD groups, the initial peak tibial latencies tended to be earlier in PD group 1 than PD group 2 (73.3 ± 18.7 vs 106.0 ± 35.8 ms; t(7) = 1.8; P = 0.11). When combining data from both PD groups, tibial accelerations were significantly smaller (44.2 ± 19.7 vs 123.6 ± 76.6 mg; t(19) = 3.0, P = 0.007) and earlier than healthy controls (87.8 ± 30.8 vs 127.1 ± 25.6 ms; t(19) = 3.0, P = 0.007). There was an inverse correlation between the sacral-to-truncal ratio and the latency of the initial peak of tibial acceleration, such that the lower sacral-to-truncal ratios occurred with a later peak tibial acceleration. When PD patients and controls were included, there was a highly significant linear regression (R2 = 0.40, P = 0.002; Fig. 2a). Combining these abnormalities provided a “rigidity index” (sacral-to-truncal ratio divided by the tibial latency in seconds—PD group 1 = 8.9 ± 3.9 s−1; PD group 2 = 4.5 ± 2.4 s−1; controls = 3.0 ± 1.8 s−1). This separated the three groups and gave a significantly higher level in PD group 1 patients than in controls (t(15) = 4.3, P < 0.001; Fig. 2b).

a An inverse relationship was present between tibial latency and the sacral-to-truncal acceleration ratio using data from all 3 cohorts. b The rigidity index (sacral-to-truncal ratio divided by the tibial latency in seconds) was greater in PD group 1 compared to controls but not significantly different between PD groups and between PD group 2 and controls. (n.s. not significant, ***P < 0.001). c Tibial latency was inversely related to the level of paraspinal (PS) EMG at baseline, while d the sacral-to-truncal ratio was positively correlated with PS levels
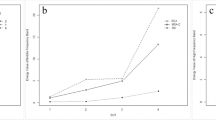
Mean baseline EMG levels were higher in most muscles for PD patients than for healthy controls, except for the soleus and RA muscles (Table 4). Pooled data showed that baseline EMG levels were higher in PD patients for quadriceps (t(17) = 2.0, P = 0.060) and PS muscles (t(17) = 2.9, P = 0.009) than controls. There were a significant linear relationships between EMG responses in the 0–200 ms post-perturbation interval and baseline EMG levels for TA (R2 = 0.19, P = 0.03), soleus (R2 = 0.33, P = 0.003), HS (R2 = 0.96, P < 0.001), quadriceps (R2 = 0.42, P = 0.003), and PS muscles (R2 = 0.48, P = 0.001; Fig. 3). The tibial acceleration latency was inversely related to the level of PS baseline activity (R2 = 0.35; P = 0.008; Fig. 2c). Similar but less significant inverse relationships were present for HS and quadriceps tonic pre-stimulus EMG levels (R2 = 0.15 and 0.24, P = 0.10 and 0.03). There were significant linear relationships of the sacral-to-truncal ratio to PS (R2 = 0.41, P = 0.004; Fig. 2d), Quadriceps (R2 = 0.46, P = 0.002), and HS baseline activity (R2 = 0.47, P = 0.002). TA and soleus baseline levels, however, did not correlate significantly with the sacral-to-truncal ratio or tibial accelerations (initial peak amplitude or latency).

Linear regressions showing that the earliest EMG response post-perturbation (0–200 ms interval) scales linearly with the level of baseline EMG for all muscles recorded. For simplicity, combined data for anterior and posterior perturbations are shown for each muscle, noting that each group and direction is shown separately. All the regressions apart from that for RA, were statistically significant (P < 0.003 for all other muscles). TA tibialis anterior, SOL soleus, QUAD quadriceps, HS hamstrings, RA rectus abdominis, PS lumbar paraspinal
There was no significant difference between the three groups when comparing EMG baseline levels for TA (t(10–16) = 0.2–0.7, P = 0.50–0.85) or soleus (t(10–16) = 0.2–0.7, P = 0.50–0.85). For the main agonist, TA, EMG onset latencies were not significantly different between the two PD groups and healthy controls (t(16) = 0.3 and 1.3, P = 0.20 and 0.80) or between the two PD groups (t(10) = 1.3, P = 0.23). The levels of activation of TA were high particularly from 100 to 200 ms after the perturbation and similar to our subjects’ maximum contraction levels (Tables 2, 3 and Fig. 4). TA EMG levels neither over the 0–100 ms (t(16) = 0.5, P = 0.62) nor the 100–200 ms intervals (t(16) = 0.2, P = 0.87) differed significantly between PD patients and controls. For soleus, PD group 1 patients demonstrated smaller EMG levels than healthy controls over the 100–200 ms post-perturbation interval (22.7 ± 16.4 vs 53.6 ± 30.9 µV; t(16) = 2.3, P = 0.03). Neither TA nor soleus showed any significant difference in EMG levels between PD group 2 and healthy controls across any of the intervals (t(16) = 0.2–0.9, P = 0.40–0.87). Neither TA nor soleus EMG levels differed between PD groups for these earliest intervals (t(10) = 0.5–1.0, P = 0.34–0.65). Overall, TA EMG activation levels were prolonged in PD group 1 compared to PD group 2 and healthy controls (Fig. 5a; interaction between group and EMG interval; F(16,168) = 2.2, P = 0.006), while, for soleus, there was no difference in EMG levels between the three groups (Fig. 5b).

Grand mean EMG traces from TA and soleus muscles from 100 ms before to 500 ms after posterior perturbation onset for PD groups 1 and 2 (darker lines) compared to healthy controls. Grand mean EMG recordings are shown for agonist (TA; top row) and antagonist muscles (soleus; bottom row). Horizontal bars indicate the intervals used to quantify mean EMG levels (0–0.1 s and 0.1–0.2 s) to compare these earliest changes in muscle activity. Levels of TA contraction in PD Group 1 were lower than controls, but this was not significant and was also accompanied by less activation of the antagonist

Rectified EMG level comparisons between groups for levels of activity for the main agonist (TA; a) and antagonist (soleus; b) during posterior perturbations. Note that raw-rectified EMG levels have been log-transformed. The prolonged contraction of TA in Group 1 PD patients was probably a consequence of their inability to compensate for the applied perturbation
The initial rate of change of vertical force was not significantly different between PD groups [t(10) = 1.6 (for 100–200 ms interval) and 0.1 (for 200–500 ms interval), P = 0.15 and 0.92] nor for each PD group compared to healthy controls [t(16) = 0.6 for PD group 1, 0.7 for PD group 2 (100–200 ms interval) and 0.8 for PD group 1, 0.9 for PD group 2 (200–500 ms interval), P = 0.38–0.53].
Anterior perturbations (pull forwards)
Neither PD group required stabilisation and both produced similar acceleration, CoP, and EMG profiles for anterior perturbations (Fig. 6). Thus, data for both PD groups were combined for all analyses. Anterior perturbations evoked rapid accelerations at the trunk (mean latency PD combined: 66.9 ms), followed by the sacrum (107.6 ms) and then the tibias (180.9 ms) in the PD patients. Overall, peak acceleration amplitudes at the upper trunk were smaller in PD patients compared to controls (PD combined vs controls: 162.9 ± 30.6 vs 243.4 ± 76.3 mg; t(22) = 3.4, P = 0.003), but other accelerations and CoP amplitudes did not differ between the groups (t(19–22) = 0.2–0.4, P = 0.71–0.87). The ratio of sacral-to-truncal accelerations was higher in PD patients but not significantly different between them and healthy controls (PD combined vs controls: 0.49 ± 0.22 vs 0.36 ± 0.22; t(21) = 1.5, P = 0.15).

Grand mean (PD group 1—left column; PD group 2—right column) and healthy controls showing recordings of acceleration, EMG, and CoP following anterior perturbations. Truncal acceleration was slightly less in the PD patients but sacral and tibial accelerations were similar in amplitude and latency to controls (grey). EMG levels were similar in soleus and TA but for PD group 1, higher in the hamstrings (HS). The initial trajectory of the CoP was similar for all groups
There was no significant difference for the latencies of peak acceleration (truncal, sacral, and tibial) and CoP (peak) between the combined PD group and healthy controls (t(19–22) = 0.4–0.7, P = 0.46–0.68). P4 showed strong anterior accelerations at all sites, indicating a tendency to move en bloc, unlike controls. CoP onset latencies were earlier in PD patients than controls (PD combined vs controls: 86.9 ± 11.7 vs 103.1 ± 17.0 ms; t(22) = 2.7, P = 0.01).
Overall, mean baseline EMG levels in PD patients were generally higher than for controls (Table 4). Pooled data showed that baseline EMG levels were higher in PD patients for HS (t(17) = 2.9, P = 0.008), quadriceps (t(17) = 3.1, P = 0.007) and PS muscles (t(17) = 3.9, P = 0.001). Soleus baseline levels were not significantly different between PD patients and controls (t(22) = 0.3, P = 0.80), whereas TA baseline levels tended to be larger in PD patients (PD combined vs controls: 23.7 ± 18.3 vs 12.3 ± 12.1 µV; t(22) = 1.8, P = 0.09). Similar to posterior perturbations, there were significant linear relationships between EMG levels in the 0–200 ms post-perturbation interval and baseline EMG levels for all muscles (Fig. 3: TA: R2 = 0.67, soleus: R2 = 0.79, HS: R2 = 0.87, quadriceps: R2 = 0.95, RA: R2 = 0.61, PS: R2 = 0.89; P < 0.001 for all).
EMG activity levels for the main agonist (soleus) did not differ significantly between PD patients and controls (F(8176) = 1.1, P = 0.31; Fig. 7a) and EMG onset latencies for soleus were not significantly different between the groups (t(22) = 0.7, P = 0.49). Over the initial 200 ms post-perturbation, soleus EMG levels for the 0–100 ms and 100–200 ms intervals were very similar for PD patients and controls (t(22) = 0.1–0.3, P = 0.76–0.91; Fig. 8). For the antagonist (TA) EMG levels did, however, show a significant difference between the groups taken over the full duration (F(8,176) = 4.4, P < 0.001; Fig. 7b), but over the initial 200 ms post-perturbation period TA EMG levels for the 0–100 ms and 100–200 ms intervals did not differ between PD patients and controls (t(22) = 0.6 and 1.5, P = 0.13 and 0.53; Fig. 8).

EMG level comparisons between groups for the main agonist (a—soleus) and antagonist (b—TA) involved during anterior perturbations. There was little difference in the main agonist (soleus) activity, while there was higher pre-stimulus and late activation in the antagonist, TA. Raw-rectified EMG levels have been log-transformed. SOL soleus

Grand mean EMG from TA and SOL muscles from 100 ms before to 500 ms after anterior perturbation onset for PD groups 1 and 2 compared to healthy controls. Grand mean EMG recordings are shown for agonist (soleus; top row) and antagonist muscles (TA; bottom row). Horizontal bars indicate the intervals used to quantify mean EMG levels (0–0.1 s and 0.1–0.2 s). Overall, EMG levels for both muscles were nearly identical for all three groups for these initial intervals post-perturbation
The initial rate of change of vertical force was not significantly different between the combined PD group and healthy controls (t(22) = 0.8 (100–200 ms interval) and 1.2 (200–500 ms interval), P = 0.42 and 0.24).
Discussion
The characteristic tendency for patients with PD to fall backwards (“retropulsion”) or forwards, particularly when displaced, was noted in the 19th century (Hunt and Sethi 2006). The mechanism of this instability was not clear. Our test is based on the clinical pull-back test, with a manually applied perturbation at the level of the shoulders, but differs in that PD patients and healthy controls were asked not to take a step in response and the induced acceleration level was monitored. The clinical test, particularly if it is necessary to evoke a step in healthy controls, is likely to use a stronger perturbation than ours. In very unstable patients, some reduction in the applied force is necessary, but the ratio of sacral-to-applied acceleration remains a useful measure. We have shown that, with our method, rapid and predictable patterns of EMG activity are evoked and that normal adults can compensate for perturbations that we apply using a target acceleration of 0.2 g. The responses appear to be independent of height and weight (Colebatch et al. 2016). Our method correlated with clinical assessment in that all the patients tested showed an inability to compensate for at least one posteriorly directed trial. In contrast, our healthy controls did not overbalance in any of the trials, despite having higher average accelerations applied to them. Unexpectedly, we found that the behaviour of two major muscles acting at the ankle (TA, soleus) and the initial forces generated were almost the same for PD patients and controls for both perturbations despite their contrasting outcomes for posterior perturbations.
Maintaining the vertical projection of the CoM within the base of support is an essential requirement for stable stance (Horak et al. 2005). We measured sacral acceleration as a surrogate for centre of mass (CoM). Our location (on average 59% of the height or 41% below the top of the head), is close to the ratio reported by a USAF study, which found a ratio of 56% of the height or 44% below the top of the head (Santschi et al. 1963). The ratio of sacral-to-applied acceleration, thus, gives an indication of the amount of the perturbation transmitted to the CoM. Assuming that our C7 (truncal) location was 90% of subjects’ height, had they behaved as a rigid object one would expect an average of 66% of the applied acceleration to be transmitted to the sacrum. This was one measure that distinguished our PD patients from the control group. Control subjects were able to achieve a significantly lower ratio, thereby reducing the fraction of the perturbation acceleration applied to the CoM. This is consistent with a reduction in effective axial stiffness in the control subjects which acted to attenuate the effects of the applied perturbations. In contrast, the ratio for both groups of PD patients was significantly higher for posterior perturbations and close to that expected for a rigid object.
Anterior perturbations did not destabilise our patients, although the applied acceleration for the more severely affected PD patients was lower than for controls. Similar to posterior perturbations, a higher proportion of the acceleration was transmitted to the sacrum. Acceleration at the tibias was on average posterior, opposite the direction of the applied acceleration and consistent with rotation of the trunk with hip flexion. The postural abnormalities were less for forward displacements for the PD patients, probably because they were able to achieve an equally strong contraction of soleus as controls, which was the main mechanism by which the perturbation was overcome. Although there was evidence for co-contraction of TA, this was not sufficient to reduce the initial rate of force development.
The normal tendency for posterior instability is known to be exacerbated in PD. Horak et al. (2005) investigated postural stability in normal and PD patients off their medication, in response to eight directions of body sway evoked by oppositely directed platform displacements; none of which caused loss of balance. Although PD patients showed less displacement of CoP in all directions, the CoM displacement for the patients was larger, particularly posteriorly, leading to the lowest margin of stability for this direction. The findings applied whether the PD patients stood on a narrow or a wide base. Horak et al. (2005) suggested that the basis of these findings was “postural bradykinesia”, allowing the CoM to be displaced further from its starting position (Schoneburg et al. 2013). Horak et al. (1996), studying forward displacements due to platform displacements, found normal EMG latencies compared to controls but increased tonic activity and co-contraction. This was associated with decreased rates of torque production, particularly for the largest platform displacements. We also found normal EMG latencies and co-contraction of proximal muscles. We did not, however, find any significant difference in the rate of initial agonist force production for either anteriorly or posteriorly directed perturbations. This may be in part because our patients were tested while on their usual medications.
Our PD group 1 patients showed selective impairment for posterior perturbations. Biomechanically, the two directions of perturbations are very different. For an anterior perturbation, the plantar flexors can exert a restoring torque on the body in direct proportion to the level of activation of the calf muscles, including soleus, as they act directly on the underlying surface. In contrast, the force that can be exerted to resist a posterior displacement by the dorsiflexors of the ankles is limited, because the agonist (TA) has no opposing resistance. This means that, no matter how strong the TA contraction, the maximum restoring force is limited to the component of gravity acting to accelerate the body forwards (Colebatch et al. 2016). Assuming the centre of gravity lies 6 cm anterior to the vertical, for a 70 kg subject with the centre of mass (CoM) 1.1 m above the surface, the maximum restoring force with TA activation sufficient to lift the feet off the floor, will be approximately 37 N. An acceleration of 0.1 g (50%) transmitted to the CoM implies a peak force of approximately 70 N, so compensation solely through contraction of TA would not be sufficient in these circumstances. Compensation for a large posterior perturbation is, thus, fundamentally different from that for a small perturbation where changes in TA activation could be fully compensatory.
Movement around more proximal joints also allows for greater resilience, by absorbing some of the applied force as a rotation of the trunk. Like Horak et al. (2005), we also found significantly reduced anterior tibial acceleration in both of our PD patient groups, associated with a shortening of latency. Healthy controls flexed their knees in response to the perturbation and in so doing allowed their trunks to rotate backwards to absorb a part of the imposed force in the form of a rotation of the body around the CoM. Co-contraction is more marked for proximal muscles for PD patients than distal ones (Dimitrova et al. 2004). Grüneberg et al. (2004) showed that artificially increased stiffness due to a corset compromised the ability of young volunteers to respond to displacements laterally and posteriorly. Horak et al. (1992) used the term “postural inflexibility” to apply to the failure of PD patients to be able to suppress postural reflexes when they were not needed. Our patients were unable to reduce their truncal compliance to the same extent as our healthy controls and had significantly higher sacral-to-truncal acceleration ratios. Later, Grimbergen et al. (2004) used the term “postural inflexibility” in a manner closer to “postural rigidity”, meaning a reduction in flexible (compliant) postural responses as a consequence of increased tonic muscle activity. We have shown that, in fact, the increased tonic activity in addition to any effect it has itself also acts to increase resistance to perturbations by increasing the level of initial balance responses to perturbations, as well. Matthews (1986) pointed out that reflexes should be expected to scale in proportion to background activation and we have shown that this applies to balance responses. Grimbergen et al. (2004) also pointed out that stiffening does have some advantages. These particularly apply to small perturbations where the tonic activity may increase postural reflexes and thereby attenuate the effect of the perturbations. This effect would explain the paradoxical reduction in spontaneous sway levels seen for PD patients (Horak et al. 1992). However, this tonic activity can become disadvantageous in particular for a larger perturbation in which responses other than stiffening around joints is required for compensation.
Although we were able to show clear differences from healthy controls, we were unable to fully separate our two PD groups on any measure. Our findings indicate a continuum between Hoehn and Yahr stages 2 and 3 with the pathophysiological differences being a matter of degree, perhaps with a critical threshold. While EMG activity around the ankles was little different between our three groups, we found that the tibial acceleration latency and the truncal rigidity, as measured by the sacral-to-truncal acceleration ratio, were related and both were clearly different from controls. Our rigidity ratio is an expression of this combined deficit. These two parameters can be regarded as related measures of overall rigidity and were more marked for our more severely affected PD group. As patients develop increasing levels of tonic muscle activity and, thus, become more rigid, it becomes increasingly difficult for them to maintain upright stance in response to even modest-sized posterior perturbations. Truncal rigidity means that more of the applied perturbation is transmitted to the CoM and PD patients become unable to generate the more complex response that is required to compensate for posterior perturbations. Increasing truncal and thigh muscle tonic activation and associated balance responses appear to be important contributors to these abnormalities.
References
Bloem BR, Allum JHJ, Carpenter MG, Honegger F (2000) Is lower leg proprioception essential for triggering human automatic postural responses? Exp Brain Res 130:375–391
Bloem BR, Grimbergen YA, Cramer M, Willemsen M, Zwinderman AH (2001) Prospective assessment of falls in Parkinson’s disease. J Neurol 248:950–958
Bloem BR, Hausdorff JM, Visser JE, Giladi N (2004) Falls and freezing of gait in Parkinson’s disease: a review of two interconnected, episodic phenomena. Mov Disord 19:871–884
Colebatch JG, Govender S (2018) Axial reflexes are present in older subjects and may contribute to balance responses. Exp Brain Res 236:1031–1039
Colebatch JG, Govender S, Dennis DL (2016) Postural responses to anterior and posterior perturbations applied to the upper trunk of standing human subjects. Exp Brain Res 234:367–376
Dimitrova D, Horak FB, Nutt JG (2004) Postural muscle responses to multidirectional translations in patients with Parkinson’s disease. J Neurophysiol 91:489–501
Goetz CG (1986) Charcot on Parkinson’s disease. Mov Disord 1:27–32
Grimbergen YA, Munneke M, Bloem BR (2004) Falls in Parkinson’s disease. Curr Opin Neurol 17:405–415
Grüneberg C, Bloem BR, Honegger F, Allum JHJ (2004) The influence of artificially increased hip and trunk stiffness on balance control in man. Exp Brain Res 157:472–485
Hoehn MM, Yahr MD (1967) Parkinsonism: onset, progression and mortality. Neurology 17:427–442
Horak FB, Nutt JG, Nashner LM (1992) Postural inflexibility in parkinsonian subjects. J Neurol Sci 111:46–58
Horak FB, Frank J, Nutt J (1996) Effects of dopamine on postural control in parkinsonian patients: scaling, set and tone. J Neurophysiol 75:2380–2396
Horak FB, Dimitrova D, Nutt JG (2005) Direction-specific postural instability in subjects with Parkinson’s disease. Exp Neurol 193:504–521
Hughes AJ, Daniel SE, Kilford L, Lees AJ (1992) Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiat 55:181–184
Hunt AL, Sethi KD (2006) The pull test: a history. Mov Disord 21:894–899
Kataoka H, Tanaka N, Eng M, Saeki K, Kiriyama T, Eura N, Ikeda MW et al (2011) Risk of falling in Hoehn-Yahr stage III. Eur Neurol 66:298–304
Koller WC, Glatt S, Vetere-Overfield B, Hassanein R (1989) Falls and Parkinson’s disease. Clin Neuropharmacol 12:98–105
Matthews PBC (1986) Observations on the automatic compensation of reflex gain on varying the pre-existing level of motor discharge in man. J Physiol 374:73–90
Munhoz RP, Teive HA (2014) Pull test performance and correlation with falls risk in Parkinson’s disease. Arq Neuropsiquiatr 72:587–591
Munhoz RP, Li J-Y, Kurtinecz M, Piboolnurak P, Constantino A, Fahn S, Lang AE (2004) Evaluation of the pull test technique in assessing postural instability in Parkinson's disease. Neurology 62:125–127
Nonnekes J, Goselink R, Weerdesteyn V, Bloem BR (2015) The retropulsion test: a good evaluation of postural instability in Parkinson’s disease? J Parkinsons Dis. 5:43–47
Santschi WR, DuBois J, Omoto C (1963) Moments of inertia and centers of gravity of the living human body. In: Technical documentary report AMRL-TDR-63-36
Schoneburg B, Mancini M, Horak F, Nutt JG (2013) Framework for understanding balance dysfunction in Parkinson’s disease. Mov Disord 28:1474–1482
Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE (2015) Systematic review of levodopa dose equivalency reporting in Parkinson’s disease. Mov Disord 25:2649–2653
Visser M, Marinus J, Bloem BR, Kisjes H, van den Berg BM, van Hilten JJ (2003) Clinical tests for the evaluation of postural instability in patients with Parkinson’s disease. Arch Phys Med Rehabil 84:1669–1674
Wielinski CL, Erickson-Davis C, Wichmann R, Walde-Douglas M, Parashos SA (2005) Falls and injuries resulting from falls among patients with Parkinson’s disease and other parkinsonian syndromes. Mov Disord 20:410–415
Acknowledgements
We thank the normal volunteers who were part of the Neuroscience Research Australia volunteer database.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Colebatch, J.G., Govender, S. Responses to anterior and posterior perturbations in Parkinson’s disease with early postural instability: role of axial and limb rigidity. Exp Brain Res 237, 1853–1867 (2019). https://doi.org/10.1007/s00221-019-05553-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-019-05553-8