
Abstract
Varying the gain of the feedback signal during a target-matching task alters the synaptic input onto the motor neuron pool. The purpose was to determine the influence of the gain of the feedback signal on the time to failure for men and women when maintaining arm position while supporting a submaximal inertial load with the elbow flexor muscles. While seated with the upper arm vertical, 15 women and 14 men maintained a constant elbow angle (1.57 rad) and supported a load equal to 15% of maximal voluntary contraction (MVC) force until failure. The task was performed on separate days with either a low gain or a high gain for the joint-angle signal. The percent decline in MVC force after the fatiguing contraction was similar for the low- and high-gain conditions (P = 0.24), and did not differ for men and women (P = 0.11). The discharge of motor units in biceps brachii declined at a greater rate during the high-gain condition for men and women, but only the women experienced a briefer time to failure for the high-gain session (8.7 ± 2.3 min) compared with the low-gain session (11.9 ± 4.8; P = 0.003). The men had similar times to failure for the low- (6.0 ± 2.2 min) and high-gain conditions (5.9 ± 2.1 min; P = 0.35). Linear and stepwise, multiple-regression analyses revealed that the time to failure for the men was associated with the absolute target force, the standard deviation (SD) for the resultant wrist acceleration, and the brachialis aEMG (P ≤ 0.02), whereas the time to failure for the women was associated with the rate of decline in motor unit discharge, the SD for the resultant wrist acceleration, and the changes in mean arterial pressure and heart rate (P ≤ 0.001). Despite each subject exerting the same net muscle torque during the two gain conditions and a similar effect of feedback gain on the discharge rate of motor units for all subjects, the time to failure for the fatiguing contractions was limited by different mechanisms for the men and women.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Synaptic input onto the motor neuron pool varies with the requirements of the task during a submaximal fatiguing contraction. For example, indirect measures of central neural activity, such as mean arterial pressure, heart rate, fluctuations in motor output, and perceived exertion, increased more rapidly when subjects were required to support a submaximal load while maintaining the position of the limb (position task) compared with exerting an equivalent force against a rigid restraint (force task) (Hunter et al. 2002; Hunter and Enoka 2003; Maluf et al. 2005; Rudroff et al. 2005). The enhanced rate of increase in these neural indices was associated with a briefer time to failure for the position task, a greater reduction in the motor unit discharge rate, a more pronounced increase in discharge rate variability, and an augmented recruitment of motor units compared with the force task (Mottram et al. 2005). The briefer time to failure for the position task was thus attributed to a more rapid recruitment of the motor neuron pool (Maluf et al. 2005).
Although each subject exerted the same net muscle torque when performing the force and position tasks, the synaptic inputs onto the motor neuron pools must have differed to produce the observed differences in motor unit activity. Differences in the synaptic input during the force and position task, for example, likely involve alterations in muscle spindle sensitivity, which is augmented during postural tasks that require fine precision (Hulliger 1993; Kakuda et al. 1996; Ribot-Ciscar et al. 2000) and when the limb acts against a compliant load compared with a rigid restraint (Akazawa et al. 1983; De Serres et al. 2002).
In addition to the type of load supported during a fatiguing contraction, however, the synaptic input onto a motor neuron pool can be influenced by such criteria as the requisite attentiveness and the perceived anxiety of the task. For example, an increase in the attentiveness required for a task, which can be accomplished by increasing the gain of the visual feedback signal, is accompanied by increases in motor unit synchronization (Schmied et al. 2000) and sensitivity of the muscle spindle (Nafati et al. 2004). Furthermore, operating a computer mouse with enhanced gain of the visual feedback can lead to errors in target matching as high as 70% (Klatzky et al. 2003), indicating that visual feedback of hand position may greatly influence performance.
The response to an imposed stressor, such as increasing feedback gain, can differ for men and women and influence the performance characteristics of the task. For example, women reported greater anxiety and exhibited greater 1–2 Hz oscillations in force than men when a stressor was imposed during a submaximal pinch grip task (Christou et al. 2004) and were less accurate than men when performing a pinch task during an imposed stressor (Noteboom et al. 2001). Accordingly, varying the gain for the feedback signal during the position task may increase anxiety and evoke different responses in men and women.
The purpose of the study was to determine the influence of the gain of the feedback signal on time to failure for men and women when maintaining arm position while supporting a submaximal inertial load with the elbow flexor muscles. The hypothesis was that the gain of the feedback signal would influence both the rate of decline in motor unit discharge and the time to failure for the sustained contraction, and that the extent of these effects would be greater for the women. The findings indicated that despite the two contractions requiring the same net muscle torque, the condition involving the more sensitive joint-angle signal was associated with enhanced central activity, including a greater reduction in the discharge rate of motor units for all subjects, but a decrease in the time to failure of the fatiguing contraction for only the women. Some of these data have been presented previously in abstract form (Mottram et al. 2005b).
Methods
Twenty-nine healthy adult subjects (15 women; 24.4 ± 5.5 years; range, 18–38 years) participated in the study. All subjects were moderately active and were right-handed (average Laterality Quotient score was 0.78 ± 0.18; range: 0.25–1.0), as identified by the Edinburgh Handedness Inventory (Oldfield 1971). None of the subjects had any known neurological disorder or cardiovascular disease and all subjects were naive to the purpose of the experiment. The Human Research Committee at the University of Colorado approved the procedures and the experiments were performed in accordance with the Declaration of Helsinki. All subjects gave written informed consent prior to participating in the study.
Experimental arrangement
Subjects were seated upright in an adjustable chair with the non-dominant arm abducted approximately 0.26 rad and the elbow resting on a padded support. The non-dominant arm was used for all subjects during the fatiguing contraction to reduce variability between subjects (Williams et al. 2002). The elbow joint was flexed to 1.57 rad and positioned midway between pronation and supination with the forearm parallel to the ground. Activation of the elbow flexor muscles caused an upward force to be applied at the wrist. One strap was placed around the subject’s waist and chair, and one nylon strap was placed vertically over each shoulder to restrain the subject and to minimize shoulder movement. The hand, wrist, and forearm were secured in a modified wrist-hand-thumb orthosis (Orthomerica; Newport Beach, CA, USA).
The force applied at the wrist in the vertical direction was measured with a force transducer that was mounted on a custom-designed, adjustable support. The orthosis was rigidly attached to the force transducer. The maximal voluntary contraction (MVC) force of the elbow flexor muscles was measured in the upward vertical direction at the wrist with the JR-3 Force-Moment Sensor (0-900-N range, 89.7 N/V JR-3 Inc., Woodland, CA, USA) prior to performing each fatiguing contraction. The force detected by the transducer was recorded online using a Power 1401 analog-to-digital converter and Spike2 (Version 5.02) software (Cambridge Electronics Design, Cambridge, UK). The force exerted in the vertical direction was displayed on a 17-inch monitor that was located at eye level approximately 1.2 m in front of the subject.
Elbow angle during the fatiguing contraction was measured with an electrogoniometer (SG110 and K100, Biometrics, Cwmfelinfach, Gwent, UK) that was secured on the lateral side of the left elbow joint. Two uniaxial piezoresistive accelerometers (model 7265A-HS, Endevco; linear range of acceleration response ± 100 m/s 2, San Juan Capistrano, CA, USA) were mounted on the orthosis near the thumb to record acceleration in the vertical and horizontal (side-to-side) directions. Output from the electrogoniometer and accelerometers were recorded online. Elbow angle was displayed on the 17-inch monitor located 1.2 m in front of the subject.
The compressive force under the elbow joint was recorded with an Entran transducer (ELW-D1-100L, 273.37 mV range, Fairfield, NJ, USA) that was placed under the padded elbow support. The compression force was displayed on an oscilloscope and collected online.
The EMG of the short and long heads of the biceps brachii and the triceps brachii muscles was recorded with bipolar surface electrodes (8-mm diameter; silver-silver chloride) that were placed 16 mm apart (center-to-center) on the skin overlying the respective muscles. Electrodes were placed between the innervation zone and the distal tendons (Freriks et al. 1999; Merletti et al. 2001). Reference electrodes were placed over the dorsal surface of the ulna at the elbow, and over the superior surface of the acromion. The EMG of the brachialis muscle was measured with an intramuscular bipolar electrode inserted 3–4 cm proximal to the antecubital fold. The electrode comprised two stainless-steel wires (100-μm diameter) that were insulated with Formvar (California Fine Wire Company, Grover Beach, CA, USA). One wire in each pair had the insulation removed for approximately 2 mm to increase the recording volume of the electrode. A surface electrode (8-mm diameter) placed on the lateral epicondyle of the humerus served as the reference electrode. Surface and intramuscular EMG signals were amplified (500–2,000×) and band-pass filtered (13–1,000 Hz) with Coulbourn modules (Coulbourn Instruments, Allentown, PA, USA) prior to being displayed on an oscilloscope and online.
Muscle fiber action potentials from single motor units in the biceps brachii were recorded with subcutaneous electrodes (stainless steel, 50-μm diameter; California Fine Wire Company, Grover Beach, CA, USA). The electrode contained three exposed areas where the insulation was removed: two on one wire (branched) and one on the other wire (monopolar) directly across from the midpoint of the branched pair (Gydikov et al. 1986; Enoka et al. 1988). Each exposed area had a width of 0.75–1 mm, and the space between each exposed area was 0.75–1 mm. Thus, the entire length of the branched (two short-circuited surfaces) and the monopolar-exposed surfaces was 3–5 mm. The wires were secured together with all-purpose gel, leaving the recording sites exposed. A disposable 25-gauge hypodermic needle was used to insert the branched bipolar electrode under the skin (not penetrating the fascia) and over the belly of the biceps brachii muscle for a distance of 3–8 cm, and was removed prior to recording motor unit activity. The electrode was positioned perpendicular to the direction of the muscle fibers. Prior to determining the recruitment threshold, the position of the electrode was altered to optimize the detection of action potentials from a single motor unit, and was not moved again until the experiment was completed. Single motor unit recordings were amplified (1,000–2,000×), bandpass filtered (20–8,000 Hz), and displayed on an oscilloscope and recorded online.
Experimental procedures
Each subject participated in one familiarization and two experimental sessions that were separated by at least 1 week. The main task in each experimental session was to sustain an isometric contraction at 15% of maximum with the elbow flexor muscles of the left arm for as long as possible while maintaining the elbow angle at 1.57 rad. The gain for the elbow-angle signal differed for the two experimental sessions: there was a high gain (0.13°/cm) in one session and a low gain (30°/cm) in the other session. Subjects were not informed that the gain of the feedback signal differed across sessions. The gain values were chosen to be 15 times less and greater than the gain (2°/cm) used in a previous study (Hunter et al. 2003) in which subjects performed the fatiguing contraction with a moderate visual gain for elbow angle and exhibited no differences in time to failure, or in the rates of increase in perceived exertion, pressor response, or standard deviation (SD) for acceleration across three sessions.
Prior to the experimental sessions, each subject visited the laboratory for an introductory session to become familiar with the equipment and the procedures, and to perform several trials of the MVC task. The experimental sessions consisted of (1) an assessment of the MVC force for the elbow flexor and extensor muscles, (2) measurement of the EMG-force relation with 5-s isometric contractions at 20, 40, and 60% MVC, (3) measurement of the recruitment threshold of a single motor unit in the biceps brachii, and (4) performance of the fatiguing contraction and a subsequent MVC. The gain of the elbow-angle signal (high or low) during the fatiguing contraction was randomized across sessions.
MVC force
The protocol began with the subject performing three isometric MVC trials with the elbow flexor muscles and three trials with the elbow extensor muscles. The MVC task consisted of a gradual increase in force from zero to maximum over 3 s, with the maximal force held for 3 s. Efforts that the subject did not regard as maximal, which were associated with lower forces, were rejected and the visual gain of the force feedback was varied across trials to minimize the subject’s awareness of differences in performance (Gandevia 2001). Subjects were given a 60–90-s rest between trials. When the peak forces from two of the three trials were not within 5% of each other, additional trials were performed until this was accomplished. The greatest force achieved by the subject was defined as the MVC force and was used as the reference for determining the 15% MVC target force for the fatiguing contraction.
EMG activity
To evaluate the reliability of the EMG measurements for each subject across sessions, subjects performed an isometric contraction for 5 s at absolute target forces of 20, 40, and 60% of MVC force. The subject was given a 60-s rest between each contraction. The order of the contractions was randomized across subjects, but remained constant for each individual subject on the 2 experimental days.
Motor unit recruitment threshold
With the non-dominant wrist attached to the force transducer, the subject gradually increased the force exerted by the elbow flexor muscles to a level that was sufficient to sustain a minimal, repetitive discharge of an isolated motor unit. Subjects were given audio feedback of action potential discharge and visual feedback of elbow flexor force to assist in achieving and maintaining a minimal repetitive discharge. The force at which the discharge rate of the isolated motor unit was minimal and repetitive was defined as the recruitment threshold (Spiegel et al. 1996). The isolated motor unit was characterized by the shape and amplitude of its action potential, which was monitored on an oscilloscope during the performance of the fatiguing contraction. In 7 of 58 experimental sessions (n = 6 subjects), a single motor unit was not isolated.
Fatiguing contraction
The fatiguing contraction was performed at a target force of 15% MVC as determined from the MVC performed on that day. There was no appreciable difference in the load hung from the wrist across sessions for the men (0.15 ± 0.15 kg; range 0.01–0.58 kg) or the women (0.17 ± 0.13 kg; range 0.02–0.41 kg). The subject was required to maintain the elbow joint angle at 1.57 rad while supporting an inertial load equivalent to 15% of maximum hung from the wrist. To avoid movement of the load outside the plane of the forearm, the load was rigidly attached to the orthosis with a solid plastic mold that hung from the orthosis. Subjects were provided with visual feedback of elbow angle and were verbally encouraged to sustain the task for as long and as precisely as possible. Criteria for task termination were similar to a previous study (Hunter et al. 2002): either a reduction in the elbow angle by 0.17 rad from a right angle or deviation of the forearm from a neutral position in a sagittal plane for greater than 5 s, despite strong verbal encouragement. The position of the forearm was assessed by close visual inspection of its location. These criteria were identical for the two conditions and were monitored by the same investigator for all sessions. The time from the beginning to the end of the fatiguing contraction was recorded as the time to failure.
Cardiovascular measures
Heart rate and blood pressure were monitored with an automated beat-by-beat, blood pressure monitor (Finapres 2300, Ohmeda; Madison, Wisconsin, USA). The blood pressure cuff was placed around the middle finger of the dominant hand and the arm was supported on a table at heart level with both the shoulder abducted and the elbow flexed to 1.57 rad.
Measures of exertion
The rating of perceived exertion (RPE) was assessed with the modified Borg 10-point scale (Borg 1982). Subjects were instructed to focus the assessment of effort on the arm muscles performing the task. The scale was anchored so that 0 represented the resting state and 10 corresponded to the strongest effort that the arm muscles could perform. The measures of exertion, mean arterial pressure, and heart rate were recorded at 30-s intervals throughout the contraction duration.
Data analysis
Force, acceleration, elbow angle, and EMG were recorded online and subsequently digitized (A/D converter, 16-bit resolution) and analyzed offline using the Spike2 (version 5.02) data-analysis system. The single motor unit recordings were digitized at 16.5 k samples/s and the surface and intramuscular EMGs were recorded at 2,083 samples/s. The force, position, and acceleration signals were digitized at 200 samples/s.
The MVC force was quantified as the peak force obtained during the MVC task. The maximal EMG for each muscle was determined as the average value over a 0.5-s interval that was centered about the peak of the rectified EMG during the MVC.
Wrist acceleration during the fatiguing contraction was measured in the vertical and horizontal (side-to-side) directions and the fluctuations were quantified as the SD of the resultant (vertical and horizontal) acceleration for the first 30 s, 15 s on either side of 25, 50, and 75% of the time to failure, and the last 30 s of the contraction. The EMG activity of the biceps brachii, brachialis, and triceps brachii muscles during the fatiguing contraction (Fig. 1) was quantified in two ways: (1) for statistical purposes, as averages of the rectified EMG (aEMG) over the first 30 s, 15 s on either side of 25, 50, and 75% of time to failure, and the last 30 s of the contraction; and (2) for graphic presentation, as aEMG for every 1% of the contraction time. The EMG was normalized to the peak EMG obtained during the MVC for the elbow flexor and extensor muscles. The mean arterial pressure, heart rate, and perceived exertion were quantified at the same 25% interval time points as the other variables.

Representative data for the contractions performed to failure by a woman for the high-gain condition (a) and the low-gain condition (b). The time to failure was 8 min for the high-gain condition and 12 min for the low-gain condition. The interference EMG of the brachialis, long head of the biceps brachii, and triceps brachii increased progressively and similarly for the two gain conditions. The interference EMG for the short head of biceps brachii did not increase for either gain condition. The average elbow angle remained constant during both gain conditions and the task was terminated due to an inability of the subject to maintain the forearm in the sagittal plane
To quantify the number and duration of the EMG bursts of the elbow flexor muscles throughout the fatiguing contraction, the same analyses were used as in a previous study (Hunter et al. 2002). Briefly, the rectified EMG signal was (1) smoothed with a low pass filter at 2 Hz for surface EMG signals, and at 3.8 Hz for the intramuscular EMG (brachialis); (2) differentiated to identify rapid changes in the EMG signal; and (3) divided by the average of the rectified EMG so that muscles with different EMG amplitudes could be compared. A burst was identified when the smoothed, differentiated signal increased by more than 0.33 s−1, which corresponded to ∼3 SDs above the mean of the differentiated EMG signal based on pilot samples when the EMG signal displayed minimal bursting during the contraction. The burst rate was quantified at one-fifths of the time to task failure.
Action potentials discharged by single motor units in biceps brachii were discriminated using a computerized, spike-sorting algorithm (Spike2, version 5.02; Cambridge Electronic Design Ltd., Cambridge, UK), which identified the potentials belonging to a single motor unit based on waveform amplitude, duration, and shape (Fig. 2). When it was possible to discriminate the isolated motor unit throughout the entire contraction, the first, middle, and last 10–30 s of the contractions were analyzed. The interspike intervals of identified motor units were visually discriminated on a spike-by-spike basis for every trial to ensure accuracy in identifying discharges of the same motor unit. Mean discharge rate was determined from the interspike intervals using custom-designed software written in Matlab (Mathworks Inc, Natick, MA, USA). The interspike intervals were detrended (Laidlaw et al. 2000) prior to determining the SD and coefficient of variation for the discharge rate, and then converted to instantaneous frequencies. Discharge rates that were below 4 pps or above 50 pps (2.0 ± 1.3% of discharges) were considered outliers and were not included in subsequent analyses.

Representative trains of action potentials for one motor unit in the low-gain session and another motor unit in the high-gain session for one subject. The motor unit potentials correspond to a 4-s duration of activity at the beginning (top) and end (bottom) of the low-gain (left) and high-gain (right) sessions. The recruitment threshold of the motor unit was 11% MVC for both gain sessions. The expanded waveforms represent multiple potentials that are superimposed to indicate the accuracy of the discrimination at the beginning and end of each fatiguing contraction. The dots above the trains of potentials represent the corresponding interspike intervals and the scatter denotes the variability in discharge rate. Although the discharge rate of the single motor units was similar at the start of the two gain sessions (10.5 pps), the discharge rate was lower at the end of the high-gain session (right lower panel, 4.5 pps) compared with the low-gain session (left lower panel, 6 pps) for this subject
Statistical analysis
A mixed two-factor ANOVA (SPSS version 13.0) (2 gains × 2 sexes) with repeated measures on gain was used to compare the time to failure between sessions. A mixed four-factor ANOVA (4 muscles × 2 gains × 5 time points × 2 sexes) with repeated measures on muscle, gain, and time was used to compare aEMG of the elbow flexor (short and long heads of biceps brachii, brachialis) and extensor muscles and the burst rate of the elbow flexor muscles during the fatiguing contraction. A mixed three-factor ANOVA (3 muscles × 2 gains × 3 intensities) with repeated measures on muscle, gain, and intensity was used to compare the EMG-force relation for the isometric contractions of the elbow flexor muscles at three intensities of contraction (20, 40, 60%). Separate mixed factor ANOVAs with repeated measures on gain and time were used to compare the other dependent variables across gains, sex, and time points. These dependent variables included the MVC force before and after the fatiguing contraction, the compressive elbow force, perceived exertion, and the resultant SD for wrist acceleration, mean arterial pressure, heart rate, motor unit discharge rate, and coefficient of variation for discharge rate. Slope analyses were conducted for the two gain conditions at absolute time points to determine the rate of change in the dependent variables. These analyses were performed separately for the men and the women.
Linear regression analyses examined the associations between the rate of decline in motor unit discharge and the time to failure, and the absolute target force and time to failure, and difference in time to failure across conditions. Stepwise, multiple-regression analyses evaluated the contribution of the dependent variables (SD for the resultant wrist acceleration, rate of increase and change in mean arterial pressure, heart rate, and perceived exertion, and the aEMG for the biceps brachii short head, biceps brachii long head, brachialis, and triceps brachii) to the time to failure for the two gain conditions for the men and women. A predictor variable was considered a significant contributor to the time to failure if its P value from the regression was < 0.05.
Dependent t-tests were used to compare the recruitment threshold across gain conditions, and the percent change in the MVC after the fatiguing contractions for both gain conditions. When ANOVAs yielded significant interactions, post-hoc comparisons using the Bonferroni adjustment for multiple comparisons, and dependent and independent t-tests (non-parametric for motor unit data) were performed to locate differences between tasks and men and women at the appropriate time points. The alpha level for all statistical tests was 0.05, except for paired comparisons when the alpha level was adjusted with a Bonferroni correction. Data are reported as means ± SD within the text, and displayed as means ± SE in the figures.
Results
The fatiguing contractions performed in the two sessions required similar net muscle torques and produced comparable amounts of fatigue. The initial MVC force (Table 1) was similar across sessions for all subjects (P = 0.29) and for the women (P = 0.17) and the men (P = 0.53), which resulted in each subject supporting a similar load during the two fatiguing contractions. Furthermore, the mean vertical force under the elbow joint was similar across sessions for the women (low gain, 24 ± 28 N; high gain, 21 ± 24 N; P = 0.63) and the men (low gain, 30 ± 44 N; high gain, 28 ± 41 N; P = 0.70). The percent decline in MVC force (Table 1) was similar for the low- and the high-gain conditions (P = 0.24), and did not differ for men and women (P = 0.11).
Time to failure
Two criteria were used to denote task failure: deviation of either elbow angle or forearm location from an initial position. The elbow-angle criterion was met in 17 of 28 sessions for the men and in 23 of 30 sessions for the women, and the forearm criterion was met in 11 of 28 sessions for the men and in 7 of 30 sessions for the women.
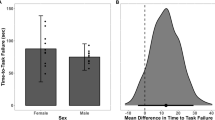
The time to failure during the two sessions only differed for the women (gain × sex interaction, P = 0.007): it was 8.7 ± 2.3 min during the high-gain condition and 11.9 ± 4.8 min during the low-gain condition (P = 0.003; Fig. 3). The times to failure for the men were 6.0 ± 2.2 min for the low-gain condition and 5.9 ± 2.1 min for the high-gain condition (P = 0.35; Fig. 3). The significant gain × sex interaction (P = 0.003) remained when strength was covaried with the time to failure. Furthermore, there was a significant main effect for sex (P < 0.001), indicating that the time to failure was longer for the women than the men in both the low- and high-gain conditions.

The time to failure for the 15 women and 14 men for the two gain conditions. Data above the line of identity indicate that the time to failure was briefer for the high-gain condition. The time to failure for the men was similar for the two gain conditions (P = 0.35), whereas it was briefer for the high-gain condition for the women (P = 0.003)
The time to failure for the fatiguing contractions was negatively associated with the absolute target force for the men (P = 0.02, r 2 = 0.19), but not the women (P = 0.64, r 2 = 0.007). However, the absolute target force was not related to the difference in the time to failure across gain conditions for either the women (P = 0.19) or the men (P = 0.21), and thus cannot explain their different responses to varying the feedback gain during the sustained contractions.
Motor unit activity
Single motor units were recorded in 51 of 58 experimental sessions (low gain, n = 26; high gain, n = 25). Sufficient data were not available at the beginning, middle, and end of the fatiguing contractions for 17 motor units, which resulted in data on 18 units during the low-gain condition and 16 during the high-gain condition for intervals of 20 ± 6 s at the start, middle, and end of the fatiguing contractions (Table 2). Each motor unit was treated as an independent factor in the statistical analysis, and not as a repeated measure, as the motor units differed within subjects across sessions. The mean recruitment threshold of the motor units (Table 2) did not differ across gains (P = 0.41) or between women and men (low gain, P = 0.25; high gain, P = 0.12).
Mean discharge rate began at similar values (P = 0.21) during the two fatiguing contractions and declined progressively (Table 3). Although the mean discharge rates were similar in the middle of the two contractions (P = 0.20), the decrease was greater by the end of the contraction during the high-gain condition (P = 0.04). The reduction in discharge rate was similar for men and women (P = 0.99). Nonetheless, the rate of decline in discharge rate was associated with the time to failure for the fatiguing contractions only for the women (P = 0.001, r 2 = 0.50) and not the men (P = 0.15, r 2 = 0.11). The variability in discharge rate, expressed as the coefficient of variation (Table 3), increased during both gain conditions (P < 0.001) for the men and the women (P = 0.72).
Factors contributing to the sex difference
Because feedback gain influenced the discharge rate of motor units in all subjects but the time to failure of only the women, other factors must have contributed to the different responses of the men and women. This possibility was assessed by comparing changes in measures of central neural activity (perceived exertion, mean arterial pressure, and heart rate) and motor output (wrist acceleration and EMG activity).
Central neural activity
Perceived exertion was similar at the start of the contractions for the women (low gain, 0.7 ± 0.4; high gain, 0.9 ± 0.5; P = 0.17), but increased more rapidly during the high-gain condition (P = 0.006; Fig. 4a). For the men, however, there was no difference in either the initial value or the rate of change in RPE between the two gain conditions (P = 0.82; Fig. 4b).

Increase in the rating of perceived exertion (RPE) during fatiguing contractions performed during the low- and high-gain conditions by the women (a) and men (b). Values are indicated as mean ± SE. Measurements were made at the beginning of each task and at increments of 25% of task duration. The horizontal error bars denote the variability in task duration between subjects. The RPE increased more rapidly during the high-gain condition for the women (P = 0.006), but not for the men (P = 0.82)
In contrast, the rates of increase in the mean arterial pressure and heart rate for the men and women were similar for the two conditions. Mean arterial pressure was similar at the start (low gain, 87 ± 11 mmHg; high gain, 87 ± 12 mmHg) and end (low gain, 130 ± 21 mmHg; high gain, 125 ± 14 mmHg) of the fatiguing contractions for the two gain conditions (P = 0.13). Heart rate was also similar across gain conditions for the women at the start (low gain, 82 ± 17 bpm; high gain, 81 ± 13 bpm) and end (low gain, 107 ± 21 bpm; high gain, 103 ± 18 bpm) of the fatiguing contractions for the two gain conditions (P = 0.24).
Similarly, mean arterial pressure for the men was similar at the start (low gain, 95 ± 16 mmHg; high gain, 90 ± 9 mmHg) and end (low gain, 134 ± 16 mmHg; high gain, 130 ± 14 mmHg) of the fatiguing contractions for the two gain conditions (P = 0.95). Heart rate was also similar across gain conditions for the men at the start (low gain, 78 ± 13 bpm; high gain, 77 ± 12 bpm) and end (low gain, 110 ± 18 bpm; high gain, 109 ± 17 bpm) of the fatiguing contractions for the two gain conditions (P = 0.25).
Motor output
The SD for the resultant wrist acceleration increased progressively during the two tasks (P < 0.001), and was similar for the men and women for the two gain conditions (P = 0.47; Fig. 5). The SD of acceleration during the low- and high-gain conditions was similar for the women at the start (0.19 ± 0.15 and 0.12 ± 0.06 m/s2, respectively) and end (0.85 ± 0.47 and 0.76 ± 0.23 m/s2, respectively) of the fatiguing contractions (P = 0.34; Fig. 5a). Slope analyses indicated that the rate of increase in the SD of acceleration for the women was greater for the high-gain condition due to the briefer time to failure (P = 0.009; Fig. 5b). The SD of acceleration for the men was not significantly different for the low- and high-gain conditions at the start (0.14 ± 0.01 and 0.14 ± 0.02 m/s2, respectively) and end (0.98 ± 0.07, and 0.84 ± 0.11 m/s2, respectively) of the fatiguing contractions (P = 0.08; Fig. 5c). Furthermore, the rate of increase in the SD of acceleration was not significantly different for the two gain conditions for the men (P = 0.08; Fig. 5d).

The SD of the resultant wrist acceleration increased during the low- and high-gain fatiguing contractions performed by the women (a, b) and men (c, d). The data (mean ± SE) are shown at the start, and at the times that corresponded to 25, 50, 75, and 100% of task duration for the women (a) and men (c). The horizontal error bars denote the variability in task duration between subjects. The SD of wrist acceleration was similar for the two gain conditions for the women (P = 0.11) and the men (P = 0.53). The rate of increase in the SD of wrist acceleration was greater for the high-gain condition for the women (P = 0.009; b), but was similar across the two conditions for the men (P = 0.08; d)
The aEMG for the elbow flexor muscles was determined at the beginning of the two sessions with isometric contractions held at 20, 40, and 60% MVC force. There was no difference in the aEMG between men and women (P = 0.36). Average EMG increased with target force (P < 0.001) and was similar across sessions (P = 0.79). A muscle × target force interaction (P < 0.001) indicated that the aEMG for the brachialis muscle at the 20 and 40% MVC forces was about twice that for the short and long heads of biceps brachii.
The aEMG (% MVC EMG) for the elbow flexor muscles during the fatiguing contractions was similar for the two gain conditions, and did not differ for men and women (P = 0.78; Fig. 6a, b). The aEMG of the brachialis muscle was greater than that for the short and long heads of biceps brachii during the two conditions (P < 0.001): the mean aEMG for the brachialis muscle during the low- and high-gain conditions (19.7 ± 9.4 and 20.0 ± 8.2%, respectively) was significantly greater (P < 0.001) than that for the short (7.8 ± 4.2 and 6.9 ± 3.2%, respectively) and long (9.1 ± 4.0 and 8.2 ± 3.6%, respectively) heads of biceps brachii. The mean aEMG of triceps brachii increased with time (P < 0.001) similarly during the low-gain (2.5 ± 1.5%) and high-gain conditions (2.6 ± 1.7%, P = 0.46).

The amplitude of the aEMG for the elbow flexor muscles during the fatiguing contractions performed during the low- (a) and high-gain contractions (b). The aEMG was normalized to the maximal values recorded during the MVC trials. Each data point corresponds to an average value for 1–100% of the average contraction duration in minutes. Standard error bars are indicated at the start, middle, and end of each aEMG. Average EMG activity (aEMG) was similar across gain conditions for the women and men (P = 0.75). The aEMG increased at the same significant rate for the long head of biceps brachii and brachialis during the two conditions (P < 0.001). The change in the aEMG for the short head of biceps brachii during the two conditions was not reliable (P ≥ 0.06). The brachialis muscle had twice the normalized aEMG compared with biceps brachii (P < 0.001) during the two contractions for the men and the women
The fatiguing contractions were characterized by a progressive increase in the number of EMG bursts for both gain conditions (P < 0.001). The average burst rate for the elbow flexor muscles differed across gain conditions for the women (P = 0.007), but not the men (P = 0.19). Burst rate during the high-gain condition for the women was lower at 75% of task duration (0.47 ± 0.93 bursts min−1) and at task termination (1.3 ± 1.5 bursts min−1) compared with the low-gain condition (0.87 ± 1.4 and 2.0 ± 2.2 bursts min−1, respectively).
Predictors of the time to failure for men and women
Stepwise, multiple-regression analyses revealed that different variables predicted the time to failure for the men and women across both gain conditions. The predictors of the time to failure for the women (R 2 = 0.76, P < 0.001; Fig. 7a) were the rate of increase in the SD of resultant wrist acceleration (r = −0.65, P < 0.001), the change in the heart rate (r = 0.37, P = 0.005), and the change in the mean arterial pressure (r = 0.26, P = 0.04). In contrast, the predictors of the time to failure for the men (R 2 = 0.64, P < 0.001; Fig. 7b) were the rate of increase in the SD of resultant wrist acceleration (r = −0.53, P < 0.001) and the mean aEMG of the brachialis muscle (r = 0.34, P = 0.02).

Relations between the observed and predicted times to failure for the two gain conditions for the women (a) and men (b). Each symbol represents the predicted versus observed time to failure for each subject for the two gain conditions. Three variables (rate of increase in resultant wrist acceleration, change in heart rate, and change in mean arterial pressure) predicted the time to failure for the women, whereas two variables (rate of increase in resultant wrist acceleration, aEMG of the brachialis) predicted the time to failure for the men. The time to failure for the women was predicted with the equation 9.883 + (31.262 × rate of increase in resultant wrist acceleration) + (0.1 × change in heart rate) + (0.09 × change in mean arterial pressure). The time to failure for the men was predicted with the equation 8.252 + (10.819 × rate of increase in resultant wrist acceleration) + (0.088 × brachialis aEMG). Three women were removed from the analyses (a) due to technical difficulties in measuring blood pressure
Discussion
The purpose of the study was to determine the influence of the gain of the feedback signal on time to failure for men and women when maintaining arm position while supporting a submaximal inertial load with the elbow flexor muscles. The gain of the feedback signal was manipulated (230-fold difference across conditions) to alter the attentiveness required to perform the task and thereby the output from the spinal cord as subjects performed the fatiguing contraction to failure. The intervention had the intended effect, as the discharge rate of single motor units in the biceps brachii was lower at the end of the fatiguing contraction during the high-gain condition compared with the low-gain condition. The time to failure for the fatiguing contractions, however, differed across gain conditions only for the women and not the men, and the decrease in discharge rate was related to the time to failure for only the women.
Gain of the feedback signal and motor unit activity
The hypothesis was that the gain of the feedback signal would influence both the rate of decline in motor unit discharge and the time to failure for the sustained contraction, and that these effects would be greater for the women. Contrary to expectations, the decline in discharge rate was greater during the high-gain condition for both the men and women, and was likely due to alterations in the descending command and the sensitivity of the muscle spindle (Schmied et al. 2000; Johansen-Berg and Matthews 2002; Nafati et al. 2004; Carson et al. 2005). Reports have indicated, for example, that improved coordination during augmented visual feedback is mediated by changes in excitability of contralateral motor pathways (Carson et al. 2005), and that attention to movement modulates cortical excitability (Johansen-Berg and Matthews 2002). Furthermore, the response of single motor units to tendon taps is greater when the gain of the feedback signal is increased (Nafati et al. 2004), and the discharge of primary Ia afferents and tendon reflexes are enhanced during precision movements (Kakuda et al. 1996) and mental computation tasks (Ribot-Ciscar et al. 2000; Rossi-Durand 2002). It has been proposed that attention-induced enhancements of the Ia reflex loop assist the visual system in controlling the motor output during demanding tasks (Prochazka 1989; Llewellyn et al. 1990). Accompanying these heightened responses, however, the amplitude of the Hoffmann (H) reflex has been observed to decline with increases in task demands, which suggests an augmentation of presynaptic inhibition under these conditions (Llewellyn et al. 1990; Rossi-Durand 2002; Nafati et al. 2004).
The greater decline in the discharge rate of motor units in biceps brachii during the high-gain condition for all subjects and the lower burst rate in the aEMG of the elbow flexor muscles at task failure for the women during the high-gain condition are consistent with the presence of a reduction in net excitation of the motor neuron pool with an increase in the gain of the feedback signal. The similar rate of increase in the mean arterial pressure across gain conditions suggests that the decrease in excitation of the motor neuron pool (Duchateau and Hainaut 1993; Butler et al. 2003) was not due to an increase in inhibitory input from metabotropic afferents (Kaufman et al. 1988; Rowell and O’Leary 1990). An alternative explanation is that the level of presynaptic inhibition of afferent feedback varied with the gain of the feedback signal (Llewellyn et al. 1990; Rossi-Durand 2002; Nafati et al. 2004), as has been demonstrated during tasks requiring greater attentiveness.
Despite the greater decline in discharge rate during the high-gain contraction, the aEMG of the elbow flexor muscles increased at a similar rate for all subjects during the two gain conditions. This dissociation underscores the insensitivity of the interference EMG to relatively modest changes in motor unit activity (Day and Hulliger 2001; Farina et al. 2004). It is also possible that additional motor unit recruitment or increased action potential duration of the already active motor units contributed to maintaining the surface EMG amplitude. Although the gain of the feedback signal did influence the rate of increase in the fluctuations in wrist acceleration for the women, there was no difference in the increase in discharge rate variability across the two gain conditions for the men and women. Conversely, the transient recruitment of motor units, as suggested by the burst rate in aEMG activity (Hunter et al. 2004; Hunter and Enoka 2003), was lower at task termination for the women during the high-gain condition and the decline in discharge rate was a predictor of the time to failure for the women, but not the men.
Increase in aEMG and synergist muscles
In the present study, there were differences in the rate of increase in the aEMG among the elbow flexor muscles: the short head of biceps brachii did not show the characteristic increase in activation as observed for the long head of biceps brachii, brachioradialis, and brachialis muscles. The exceptional behavior of the short head of biceps brachii has been observed previously (Hunter et al. 2003). In contrast, the increase in aEMG for the short head of biceps brachii was similar to that of the long head of biceps brachii and brachioradialis muscles during contractions in which the force was maintained at 20% of MVC force (Hunter et al. 2002). This difference in the aEMG for the short head of biceps brachii suggests a task-specific activation of motor unit populations within the biceps brachii, as has been demonstrated previously in single motor unit experiments (Tax et al. 1990; Van Zuylen et al. 1988).
Sex and the time to failure
As has been reported previously (Hunter and Enoka 2001; Hunter et al. 2001), women can sustain a submaximal contraction at relative target forces for a longer duration than stronger men. The current findings extend this observation by reporting a sex difference in motor performance associated with varying the gain of the visual feedback signal. To identify the mechanisms responsible for the sex difference, the absolute target force and the dependent variables were examined with linear and multiple-regression analyses separately for men and women. The analyses indicated that although the time to failure for the fatiguing contractions was related to the absolute target force for the men, the difference in the time to failure across gain conditions was not associated with the absolute target force for the men. This result suggests that the magnitude of the absolute force did not contribute to the lack of difference in time to failure across gain conditions (Hunter and Enoka 2001; Hunter et al. 2004).
Rather, it appears that the different response of the men and women to variation in the gain of the feedback signal was attributable to a difference in the mechanisms responsible for task failure. For example, the rates of increase in the SD of acceleration and perceived exertion were similar for the men, but not the women, across the two gain conditions. Possibly the heightened sensitivity of the muscle spindle in the high-gain condition contributed to the greater rate of increase in the SD of acceleration and earlier task failure for the women. Multiple regression analyses revealed that different variables predicted the time to failure for the women and men. The time to failure for the women was predicted by the rate of increase in the SD of wrist acceleration, the change in the heart rate, and the change in the mean arterial pressure. Even though the mean arterial pressure and heart rate increased at similar rates for men and women, these variables were significant factors for task performance only for the women. In contrast, the predictors of the time to failure for the men were the rate of increase in the SD of wrist acceleration and the mean aEMG of the brachialis.
Performance of the fatiguing contraction during the high-gain condition was likely a stressful task. Accordingly, subjects reported greater difficulty performing the fatiguing contraction when the gain of the feedback signal was high, even though they were not informed that the gain varied across sessions. In support of this interpretation, task performance has been reported to decline when a cognitive task is performed simultaneously during a submaximal fatiguing contraction (Lorist et al. 2002). Nonetheless, only the women experienced a greater rate of increase in perceived exertion during the high-gain condition, which suggests that their sense of effort (Carson et al. 2002) was influenced by the gain of the feedback signal. There is evidence that the sex differences in response to stress are centrally mediated. For example, women reported a more intense perception of a noxious stimulus on the hand that was associated with greater activation of the contralateral thalamus and anterior insula compared with men (Paulson et al. 1998). Furthermore, women reported greater pain and exhibited greater pupil dilation than men when sustained pressure was applied to their fingers (Ellermeier and Westphal 1995). Animal studies indicate that plasma levels of adrenocorticotropic hormone are higher in females than males in response to electrical shocks (Rivier 1999). Taken together, these observations suggest that there was greater activation of higher centers for the women when performing the high-gain contraction when greater attentiveness was required to perform the task.
In conclusion, manipulating the gain of the feedback signal reduced motor unit discharge rate during the high-gain condition for all subjects. Only the women, however, exhibited a decrease in the time to failure during the high-gain condition. The influence of feedback gain for the women was associated with differences in the rates of change for perceived exertion, SD of acceleration, and discharge rate of the motor units. Furthermore, the burst rate was lower at task failure for the women during the high-gain condition. Despite each subject exerting the same net muscle torque during the two gain conditions and a comparable influence of feedback gain on motor unit discharge for all subjects, the time to failure for the fatiguing contraction was limited by different mechanisms for the men and women.
References
Akazawa K, Milner TE, Stein RB (1983) Modulation of reflex EMG and stiffness in response to stretch of human finger muscle. J Neurophysiol 49:16–27
Borg GA (1982) Psychophysical bases of perceived exertion. Med Sci Sports Exerc 14:377–381
Butler JE, Taylor JL, Gandevia SC (2003) Responses of human motoneurons to corticospinal stimulation during maximal voluntary contractions and ischemia. J Neurosci 23:10224–10230
Carson RG, Riek S, Shahbazpour N (2002) Central and peripheral mediation of human force sensation following eccentric or concentric contractions. J Physiol 539:913–925
Carson RG, Welsh TN, Pamblanco-Valero MA (2005) Visual feedback alters the variations in corticospinal excitability that arise from rhythmic movements of the opposite limb. Exp Brain Res 161:325–334
Christou EA, Jakobi JM, Critchlow A, Fleshner M, Enoka RM (2004) The 1- to 2-Hz oscillations in muscle force are exacerbated by stress, especially in older adults. J Appl Physiol 97:225–235
Day SJ, Hulliger M (2001) Experimental simulation of cat electromyogram: evidence for algebraic summation of motor-unit action-potential trains. J Neurophysiol 86:2144–2158
De Serres SJ, Bennett DJ, Stein RB (2002) Stretch reflex gain in cat triceps surae muscles with compliant loads. J Physiol 545:1027–1040
Duchateau J, Hainaut K (1993) Behaviour of short and long latency reflexes in fatigued human muscles. J Physiol 471:787–799
Ellermeier W, Westphal W (1995) Gender differences in pain ratings and pupil reactions to painful pressure stimuli. Pain 61:435–439
Enoka RM, Robinson GA, Kossev AR (1988) A stable, selective electrode for recording single motor-unit potentials in humans. Exp Neurol 99:761–764
Farina D, Merletti R, Enoka RM (2004) The extraction of neural strategies from the surface EMG. J Appl Physiol 96:1486–1495
Freriks B, Hermens H, Disselhorst-Klug C, Rau, G (1999) The recommendations for sensors and sensor placement procedures for surface electromyography. In: Hermens H, Freriks B, Merletti R, Stegeman D, Blok J, Rau G, Disselhorst-Klug C, Hägg G (eds) European recommendations for surface electromyography. Roessingh Research and Development b.v., pp 15–53
Gandevia SC (2001) Spinal and supraspinal factors in human muscle fatigue. Physiol Rev 81:1725–1789
Gydikov A, Kossev A, Trayanova N, Radicheva N (1986) Selective recording of motor unit potentials. Electromyogr Clin Neurophysiol 26:273–281
Hulliger M (1993) Fusimotor control of proprioceptive feedback during locomotion and balancing: can simple lessons be learned for artificial control of gait? Prog Brain Res 97:173–180
Hunter SK, Critchlow A, Shin IS, Enoka RM (2004) Men are more fatigable than strength-matched women when performing intermittent submaximal contractions. J Appl Physiol 96:2125–2132
Hunter SK, Enoka RM (2001) Sex differences in the fatigability of arm muscles depends on absolute force during isometric contractions. J Appl Physiol 91:2686–2694
Hunter SK, Enoka RM (2003) Changes in muscle activation can prolong the endurance time of a submaximal isometric contraction in humans. J Appl Physiol 94:108–118
Hunter SK, Lepers R, MacGillis CJ, Enoka RM (2003) Activation among the elbow flexor muscles differs when maintaining arm position during a fatiguing contraction. J Appl Physiol 94:2439–2447
Hunter SK, Ryan DL, Ortega JD, Enoka RM (2002) Task differences with the same load torque alter the endurance time of submaximal fatiguing contractions in humans. J Neurophysiol 88:3087–3096
Johansen-Berg H, Matthews PM (2002) Attention to movement modulates activity in sensori-motor areas, including primary motor cortex. Exp Brain Res 142:13–24
Kakuda N, Vallbo AB, Wessberg J (1996) Fusimotor and skeletomotor activities are increased with precision finger movement in man. J Physiol 492(Pt 3):921–929
Kaufman MP, Rotto DM, Rybicki KJ (1988) Pressor reflex response to static muscular contraction: its afferent arm and possible neurotransmitters. Am J Cardiol 62:58E–62E
Klatzky RL, Lederman SJ, Langseth S (2003) Watching a cursor distorts haptically guided reproduction of mouse movement. J Exp Psychol Appl 9:228–235
Laidlaw DH, Bilodeau M, Enoka RM (2000) Steadiness is reduced and motor unit discharge is more variable in old adults. Muscle Nerve 23:600–612
Llewellyn M, Yang JF, Prochazka A (1990) Human H-reflexes are smaller in difficult beam walking than in normal treadmill walking. Exp Brain Res 83:22–28
Lorist MM, Kernell D, Meijman TF, Zijdewind I (2002) Motor fatigue and cognitive task performance in humans. J Physiol 545:313–319
Maluf KS, Shinohara M, Stephenson JL, Enoka RM (2005) Muscle activation and time to task failure differ with load type and contraction intensity for a human hand muscle. Exp Brain Res 167:165–177
Merletti R, Rainoldi A, Farina D (2001) Surface electromyography for noninvasive characterization of muscle. Exerc Sport Sci Rev 29:20–25
Mottram CJ, Jakobi JM, Semmler JG, Enoka RM (2005a) Motor-unit activity differs with load type during a fatiguing contraction. J Neurophysiol 93:1381–1392
Mottram CJ, Anderson MK, Hunter SK, Enoka RM (2005b) Motor unit activity differs with the gain of the position-feedback signal for a submaximal fatiguing contraction. In: American college of sports medicine annual meeting, Nashville, TN
Nafati G, Rossi-Durand C, Schmied A (2004) Proprioceptive control of human wrist extensor motor units during an attention-demanding task. Brain Res 1018:208–220
Noteboom JT, Fleshner M, Enoka RM (2001) Activation of the arousal response can impair performance on a simple motor task. J Appl Physiol 91:821–831
Oldfield RC (1971) The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 9:97–113
Paulson PE, Minoshima S, Morrow TJ, Casey KL (1998) Gender differences in pain perception and patterns of cerebral activation during noxious heat stimulation in humans. Pain 76:223–229
Prochazka A (1989) Sensorimotor gain control: a basic strategy of motor systems? Prog Neurobiol 33:281–307
Ribot-Ciscar E, Rossi-Durand C, Roll JP (2000) Increased muscle spindle sensitivity to movement during reinforcement manoeuvres in relaxed human subjects. J Physiol 523(Pt 1):271–282
Rivier C (1999) Gender, sex steroids, corticotropin-releasing factor, nitric oxide, and the HPA response to stress. Pharmacol Biochem Behav 64:739–751
Rossi-Durand C (2002) The influence of increased muscle spindle sensitivity on Achilles tendon jerk and H-reflex in relaxed human subjects. Somatosens Mot Res 19:286–295
Rowell LB, O’Leary DS (1990) Reflex control of the circulation during exercise: chemoreflexes and mechanoreflexes. J Appl Physiol 69:407–418
Rudroff T, Poston B, Shin IS, Bojsen-Moller J, Enoka RM (2005) Net excitation of the motor unit pool varies with load type during fatiguing contractions. Muscle Nerve 31:78–87
Schmied A, Pagni S, Sturm H, Vedel JP (2000) Selective enhancement of motoneurone short-term synchrony during an attention-demanding task. Exp Brain Res 133:377–390
Spiegel KM, Stratton J, Burke JR, Glendinning DS, Enoka RM (1996) The influence of age on the assessment of motor unit activation in a human hand muscle. Exp Physiol 81:805–819
Tax AA, Denier van der Gon JJ, Gielen CC, Kleyne M (1990) Differences in central control of m. biceps brachii in movement tasks and force tasks. Exp Brain Res 79:138–142
Van Zuylen EJ, Gielen CC, Denier van der Gon JJ (1988) Coordination and inhomogeneous activation of human arm muscles during isometric torques. J Neurophysiol 60:1523–1548
Williams DM, Sharma S, Bilodeau M (2002) Neuromuscular fatigue of elbow flexor muscles of dominant and non-dominant arms in healthy humans. J Electromyogr Kinesiol 12:287–294
Acknowledgements
The research was supported by an award (NS43275) to RME from the National Institute of Neurological Disorders and Stroke and a PODS II scholarship from the Foundation for Physical Therapy and an American College of Sports Medicine Foundation Research Grant to CJM. The authors thank Drs. Evangelos Christou, Benjamin Barry, Katrina Maluf, and Richard Carson for comments on a draft of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mottram, C.J., Hunter, S.K., Rochette, L. et al. Time to task failure varies with the gain of the feedback signal for women, but not for men. Exp Brain Res 174, 575–587 (2006). https://doi.org/10.1007/s00221-006-0498-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-006-0498-3