
Abstract
Rationale
Gaboxadol is a selective extrasynaptic GABAA agonist, previously in development for the treatment of insomniac patients.
Objective
To evaluate the acute efficacy and safety of gaboxadol in primary insomnia (PI).
Methods
This was a randomised, double-blind, four-way crossover, polysomnograph study comparing gaboxadol 10 and 20 mg (GBX20) to placebo in 40 adults with the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, criteria for PI. Zolpidem 10 mg was used as an active reference. Treatment was administered on two consecutive nights in each treatment session. Next-day residual effects were evaluated 2 and 9 h after lights on.
Results
Efficacy analysis included the per-protocol population (n = 38) from night 2. GBX20 reduced wake after sleep onset (p < 0.01). Both doses of gaboxadol, but not zolpidem, reduced the number of night awakenings (p < 0.001). GBX20 and zolpidem increased total sleep time (p < 0.05). Neither dose of gaboxadol nor zolpidem significantly reduced sleep onset latency, although a trend was seen for zolpidem. Gaboxadol enhanced slow wave sleep (SWS) dose-dependently (gaboxadol 10 mg: p < 0.01, GBX20: p < 0.001). Patients reported improved sleep quality following GBX20 (p < 0.05). Both doses of gaboxadol were generally well tolerated with almost exclusively mild to moderately severe adverse events (AEs). More frequent and severe AEs followed GBX20. No serious AEs were reported. No drug treatment was associated with next-day residual effects.
Conclusion
Acute administration of gaboxadol improves sleep maintenance and enhances SWS in a dose-dependent manner in adult patients with PI. Gaboxadol was not associated with next-day residual effects. Gaboxadol was generally well tolerated, although gaboxadol showed a dose-dependent increase in incidence and severity of AEs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The predominant current pharmacological approach to the treatment of insomnia involves manipulation of GABA, the major inhibitory neurotransmitter in the central nervous system. Benzodiazepine-site ligands such as traditional benzodiazepines (e.g. triazolam) and non-benzodiazepines (e.g. zolpidem) allosterically modulate synaptically located α1βγ2-containing receptors via interaction with the benzodiazepine binding site (Sigel 2005). Although effective, these traditional hypnotics tend to cause an increase in the “lighter” stages of sleep (e.g. stage 2) while either having no effects on, or even suppressing, the “deeper” stages of sleep [i.e. slow wave sleep (SWS)—stages 3 and 4) (Brunner et al. 1991; Feinberg et al. 2000; Mitler 2000; Parrino and Terzano 1996; Trachsel et al. 1990) that some researchers suggest may be the most restorative type (Benington and Heller 1995; Horne 1992). For some of these agents, concerns have also been raised about the possibility, over a course of treatment, of next-day hangover effects, the development of tolerance and dependence, or rebound insomnia (Petursson 1994; Sateia and Nowell 2004; Vermeeren 2004).
Gaboxadol is a selective extrasynaptic GABAA agonist (SEGA), distinctly different from the current treatments for insomnia (Ebert et al. 2006). Although gaboxadol is no longer in clinical development for the treatment of insomnia, the unique mechanism of action and SWS-enhancing capabilities is of genuine scientific interest. Gaboxadol’s mechanism of action is unique in that it directly activates extrasynaptically located δ-containing receptors via interaction with the GABA binding site (Belelli et al. 2005; Drasbek and Jensen 2006; Jia et al. 2005). The extrasynaptic δ-containing receptors are predominantly expressed in the thalamus, cerebral cortex, and limbic system (Belelli et al. 2005; Brunner et al. 1991; Orser 2006), regions which may have important implications for sleep regulation and synchronisation of cortical activity (Saper et al. 2001, 2005; Steriade et al. 1993). Studies in animals, healthy young and elderly subjects, and insomnia patients have shown that gaboxadol increases the time spent in non-rapid eye movement (NREM) sleep, increases NREM sleep continuity, and increases SWS (Faulhaber et al. 1997; Lancel 1997, 1999; Lancel and Faulhaber 1996; Lancel et al. 2001; Mathias et al. 2001, 2005; Deacon et al. 2007; Walsh et al. 2007). The objective of the present early-phase clinical study was to perform an initial evaluation of the hypnotic properties and safety of gaboxadol up to 20 mg after two nights of treatment in adult patients with primary insomnia. This study extends the knowledge of the efficacy and safety of gaboxadol using a higher therapeutic dose range compared to the authors’ previously published study (Deacon et al. 2007). This is also the first published study in patients with primary insomnia that provides an initial insight into how gaboxadol compares with zolpidem. Zolpidem has proven hypnotic efficacy (Scharf et al. 1994, Holm and Goa 2000) and was included as an active control for assessing study sensitivity in this early phase II clinical study.
Methods
Design
This was an early-phase, exploratory, randomised, double-blind, four-way crossover, sleep laboratory polysomnographic (PSG) study to compare the effects of gaboxadol 10 and 20 mg vs placebo on traditional hypnotic efficacy measures, sleep architecture, and safety and tolerability. Zolpidem 10 mg was included as an active control. The study was conducted at a single investigative site (Institute For Research in Neurosciences, Neuropharmacology and Psychiatry, Centre Hospitalier, Rouffach, France). The Lundbeck study number was 99311.
Patients
Patients aged 18–65 years who met the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV), criteria for primary insomnia (American Psychiatric Association 1994) were enrolled. Patients were required to have continuous complaints of sleep difficulties for the last month or longer, a score >5 on the Pittsburgh Sleep Quality Index (Buysse et al. 1989), and the following criteria during the last night of a three-night PSG screening session: (1) sleep onset latency (SOL) >20 min and (2) wakefulness during sleep >48 min or >10 night awakenings. Patients were not eligible if they had been taking any of the following medications prior to the screening visit: within 2 weeks, triazolam, zolpidem or zopiclone; within 4 weeks, other benzodiazepines, anti-cholinergics, anti-epileptic drugs, anti-histamines, centrally acting anti-hypertensives, sympathicomimetics or psychotropics; within 3 months, fluoxetine.
The main source of patient recruitment was via advertisement and, to a smaller extent, from a local psychiatric clinic where patients presenting with insomnia complaints were informed about the ongoing study. Patients were paid for their inconvenience and travel expenses incurred participating in the study. The ethics committee approved all patient payments. All patients gave written informed consent and the study was approved by the ethics committee, Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale, Strasbourg.
Procedure
Patients attended a screening visit during which their demographic data; medical, psychiatric, and medication histories; and symptoms of primary insomnia according to the DSM-IV criteria were recorded. A physical examination was also performed. Patients who satisfied preliminary eligibility criteria then attended the sleep laboratory for a screening session consisting of three nights of PSG recording lasting from 23:00 hours to 7:00 hours. Specific PSG exclusion criteria for periodic limb movement disorder (PLMD) were a periodic leg movement arousal index of >10/h and, for sleep apnea syndrome, an apnea/hypopnea index of >5/h. A wake EEG was performed to detect abnormal brain activity. Patients meeting the PSG eligibility criteria then entered the double-blind, treatment phase of the study and were randomly assigned to one of four treatment sequences according to a Williams Latin square design, in which every treatment followed every other treatment once. The randomisation code was generated independently from the study site. The treatments – gaboxadol 10- or 20-mg tablets, zolpidem 10-mg tablet or placebo tablet – were encapsulated to ensure study blinding. Patients were administered the allocated treatment 30 min before bedtime at 23:00 hours on two consecutive nights during four separate treatment sessions, each separated by a washout period of 7–14 days. PSG was recorded from 23:00 hours (lights off) to 07:00 hours (lights on) on each of the two nights per session. The patients’ own evaluation of their sleep was recorded the morning after each study medication had been administered, 30 min after awakening (07:00 hours, lights on), using the Leeds Sleep Evaluation Questionnaire (LSEQ) (Parrott and Hindmarch 1980). Next-day residual effects were evaluated using a selection of tests from the cognitive drug research (CDR) test battery (CDR, Goring-on-Thames, UK) given at 09:00 hours and 16:00 hours the day after each dose of test drug. All patients returned for a follow-up visit 7–14 days after the final PSG session. Adverse events were recorded throughout the study and were rated by the investigator with regard to severity and likelihood of being drug-related. Vital signs, ECG, routine laboratory assessments, and physical examinations were performed at regular intervals.
Assessments
PSG/EEGs were analysed by personnel without access to the treatment code. Visual scoring was performed in 30-s epochs according to the criteria described by Rechtschaffen and Kales (1968). Visually scored measures of hypnotic efficacy included: total sleep time (TST) defined as time spent in REM + NREM sleep excluding movement time; number of awakenings (NAW) defined as the number of times from sleep onset that at least one epoch of stage 0 occurred separated by at least one epoch of non-wake; wake after sleep onset (WASO) defined as the total amount of time spent awake from the start of 20 consecutive epochs of stages 1–4 or REM to lights on; sleep efficiency index (SEI) defined as 100 × TST/time in bed; and number of stage shifts (NSS) defined as the number of epoch-to-epoch shifts from one stage to another (excluding movement) during time in bed; SOL defined as the first 30 s epoch from lights off scored as stage 2, 3, 4 or REM. Effects on sleep architecture were evaluated by measuring the duration of each sleep stage, as well as latency to REM sleep, and proportion of the sleep period time spent in REM, NREM and SWS.
Self reported measures of sleep were evaluated using the LSEQ (Parrott and Hindmarch 1980). This questionnaire consists of ten 100-mm visual analogue scales pertaining to four aspects of sleep: (1) getting to sleep, (2) quality of sleep, (3) awakening from sleep and (4) behaviour following wakefulness. A score of 100 mm indicates the largest possible positive change experienced after drug administration. Conversely, 0 mm indicates the largest possible negative change experienced after drug administration.
To assess next-day residual effects, a selection of tasks from the CDR computerised cognitive assessment system (CDR, Reading, UK) were chosen to assess a range of cognitive functions including attention, working memory, long-term memory and skilled motor co-ordination. Assessments were performed at 09:00 hours (2 h after lights on) and 16:00 hours (9 h after lights on) on both days following treatment the night before. The battery consisted of tests of picture recognition (sensitivity index, speed in milliseconds), simple reaction time (speed in milliseconds), digit vigilance (speed of detection in milliseconds, percent of targets detected), choice reaction time (speed in milliseconds), spatial working memory (sensitive index, speed in milliseconds), digit symbol substitution test (number correct), visual tracking (average distance from target in millimeters), and critical flicker fusion (threshold in hertz). The tests were administered in the order listed above.
Data analysis
Efficacy analyses (PSG and LSEQ) were performed on a per-protocol data set (PPS) which excluded patients who met criteria for protocol violation or who did not have PSG assessments in all four-treatment periods. The data were analysed using the SAS® version 8 statistical software package. The analysis was based on a general linear model with fixed effects for treatment, sessions and sequence, and with a random effect of patients within sequence. Planned contrasts were performed between placebo and each active dose. Given the exploratory nature of the study, p values are reported without any adjustment for multiplicity. Data were assessed for normality and, if appropriate, a logarithmic transform was applied. The last night of the screening session (night 3) was used as the baseline. The study was designed to provide adequate lengths of washout periods to avoid potential carryover effects. The lack of carryover effects was confirmed from exploratory statistical analyses by period and analyses of potential sequence and treatment by period interactions.
Analyses of routine safety measures (e.g. adverse events, laboratory values) were performed on the all-patients-treated data set, defined as the group of patients who took at least one dose of study medication. Descriptive summary statistics were calculated for these assessments. The analysis of the CDR cognitive test battery was based on the completers data set, defined as the group of patients who completed the study and CDR assessments per protocol. Data were collected in full from all patients apart from two. The SAS® PROC MIXED procedure was used to conduct ANOVA at each time point, fitting dosing condition as a fixed factor and patient as a random factor. The SAS® LS MEANS procedure was used to make contrasts between placebo and each active dose.
Results
Patient accounting and baseline characteristics
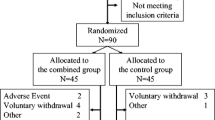
A total of 126 patients were screened to randomise 40 patients. The main reason for ineligibility during screening was a SOL < 20 min on the third screening night (n = 23, 18.3%). Other frequent (>2%) reasons for exclusion were PLMD (n = 14, 11.1%), sleep apnea (n = 10, 7.9%), abnormal clinical haematology/chemistry laboratory results (n = 8, 6.4%), abnormal EEG (n = 6, 4.8%), abnormal ECG (n = 6, 4.8%), other sleep entry criteria exclusions (abnormal bedtimes/shiftwork/Pittsburg Sleep Quality Index; n = 5, 4.0%), other medical history (n = 4, 3.2%) and personal reasons (n = 3, 2.4%). The 40 patients randomised consisted of 26 women and 14 men with a mean age of 34.2 years (SD 10.7), mean body mass index of 23.4 kg/m2 (SD 3.2), and mean Pittsburgh Sleep Quality Inventory score of 11.2 (SD 2.2). Among the 40 patients randomised, two were protocol violators and were excluded from the PPS (n = 38) used for the efficacy analyses; one protocol violator was withdrawn from the study due to a positive drug screen for opiates and the other completed the study but not in accordance with the randomised treatment order. Mean (SE) PSG sleep maintenance characteristics at baseline (night 3) were TST = 379.6 (7.8) minutes, WASO = 52.2 (6.6) minutes, NAW = 20.1 (1.3) and SEI = 79.0 (1.6) percent. Mean SOL at entry/baseline was 45.5 (SE 3.3) minutes. For key sleep architecture variables, patients had baseline means (SE) of 70.9 (4.5) minutes of SWS, 81.5 (3.5) minutes of REM sleep and 66.0 (3.8) minutes latency to REM sleep.
Patients had a mean history of insomnia for approximately 6.4 years (SD 7.0; range from at least 1 month to 30 years). There were no other clinically significant medical conditions that were ongoing at screening. Prior neurological history revealed four patients with headache and one with migraine which were ongoing at entry into the study. Neither condition was considered clinically significant. Eleven patients had a previous history of anxiety and/or depression but none were ongoing at time of entry into the study (exclusion criteria). Five patients had previously taken hypnotics (within 3 months of entry into study); two patients had taken one dose only, one had taken zolpidem for 7 years, one had taken bromazepam for 1 month and another had taken zolpidem for 10 months. There were no reports of non-drug treatment in the medical history.
The analysis of the CDR cognitive test battery was based on the completers data set, defined as the group of patients who completed the study and CDR assessments. Data were collected in full from all patients apart from two.
Efficacy
The results from the analyses of sleep maintenance and sleep induction parameters on night 2 for the PPS are presented in Table 1. Gaboxadol 20 mg reduced WASO (by about 8 min vs placebo). Gaboxadol 20 mg and zolpidem 10 mg improved TST (by about 10 min vs placebo for both treatments). Both gaboxadol doses reduced NAW (by about 4.5 vs placebo), whereas zolpidem did not differ significantly from placebo. Also, both gaboxadol doses reduced NSS (by about 11 vs placebo), whereas zolpidem did not differ significantly from placebo on this measure. With regard to sleep initiation, neither gaboxadol nor zolpidem had a statistically significant effect on SOL, although a trend for a reduction was observed with zolpidem.
The results of the analysis of visually scored sleep architecture data for night 2 are presented in Table 1. Gaboxadol 20 mg impressively enhanced SWS duration by 25 min compared with placebo; this was mainly due to enhancement of stage 4 sleep, although a significant enhancement of stage 3 sleep was also observed. Gaboxadol 20 mg also significantly reduced stage 1 duration (by about 3 min vs placebo) and REM duration (by about 8 min vs placebo) and increased REM latency (by about 16 min vs placebo). The proportion of REM sleep following gaboxadol 20 mg was also reduced when compared to placebo treatment. Gaboxadol 20 mg also increased the proportions spent in NREM and SWS relative to placebo. Gaboxadol 10 mg significantly enhanced SWS duration by 15 min compared with placebo, mainly due to a significant enhancement of stage 4 sleep, and significantly reduced stage 1 duration (by about 3 min vs placebo). Gaboxadol 10 mg also increased the proportion of the sleep period time spent in SWS but had no effect on the proportions spent in REM or NREM relative to placebo. The main finding for zolpidem was that it increased stage 2 duration by about 17 min vs placebo; by contrast, neither dose of gaboxadol affected this sleep stage. Zolpidem had no significant effect on SWS but reduced REM duration by about 7 min vs placebo. Zolpidem also reduced the proportion of the sleep period time spent in REM and increased the proportion spent in NREM but had no effect on the proportion spent in SWS relative to placebo.
With regard to subjective evaluation of sleep and next-day feeling/behaviour assessed by the LSEQ, gaboxadol 20 mg significantly improved “quality of sleep” (p = 0.043) and showed a non-significant trend for improving “getting to sleep” (p = 0.066), without any deleterious effects on the “awakening from sleep” and “behaviour following sleep” components (Table 2). There were no significant effects of gaboxadol 10 mg or zolpidem 10 mg on any of the four components.
Safety
Both doses of gaboxadol and zolpidem were generally well tolerated in this short-term study (Table 3). There were no serious adverse events and no patients withdrew due to an adverse event. The percentages of patients with adverse events were greater in the active treatment groups than in the placebo group (placebo = 33%, zolpidem = 51%, gaboxadol 10 mg = 45%, gaboxadol 20 mg = 48%). All but two of the 116 adverse events were rated as mild or moderate in severity by the investigator. The severity of adverse events following gaboxadol appeared to be dose-related; the numbers of events that were at least moderate in severity were three for placebo, nine for zolpidem, 12 for gaboxadol 10 mg, and 17 for gaboxadol 20 mg. The only two adverse events rated as severe in intensity, comprising panic attack and vomiting, occurred in the gaboxadol 20 mg group. Both events were transient and did not result in the patients being discontinued from the trial. The most common adverse events associated with gaboxadol, which showed an increase vs placebo, were gastrointestinal symptoms such as nausea, gastroenteritis and vomiting (Table 3).
There appeared to be a gender effect with regard to adverse events. In the 14 males, there were a total of 20 adverse events; the numbers of males with adverse events were comparable in the placebo (n = 3, 21%), gaboxadol 10 mg (n = 3, 21%) and gaboxadol 20 mg (n = 2, 14%) groups, and highest in the zolpidem group (n = 8, 62%). In the 26 females there were a total of 96 adverse events; the numbers of females with adverse events were higher in the gaboxadol 20 mg (n = 17, 65%), gaboxadol 10 mg (n = 15, 58%) and zolpidem (n = 12, 46%) groups compared with the placebo group (n = 10, 38%).
No clinically relevant treatment effects were seen for mean or individual changes in biochemistry, haematology, urinalysis, vital sign or ECG values, and no noteworthy changes were observed on physical or neurological clinical examinations. There was no evidence of adverse cognitive effects for any treatment using the CDR test battery (data not shown). There were two significant findings—a faster response time for zolpidem over placebo of approximately 12 ms in digit vigilance speed (p = 0.023) at 09:00 hours on day 2 and a faster response time for gaboxadol 10 mg over placebo of approximately 47 ms in picture recognition speed at the 09:00 hours time point on day 3 (p = 0.016).
Discussion
The results of the present study indicated that short-term treatment with gaboxadol improves sleep maintenance in patients with primary insomnia. The effect is particularly robust following 20 mg in that sleep parameters WASO, TST and NAW are improved. The effects on PSG endpoints in the present study are associated with a higher patient rating of the sleep quality. Some dose dependency was observed in that gaboxadol 10 mg only had positive effects on NAW. Positive effects by short-term gaboxadol treatment on sleep maintenance parameter TST have previously been reported for doses 5 and 15 mg (Deacon et al. 2007). However, there were no effects on WASO or NAW, further indicating a dose dependency in the robustness effects on sleep maintenance. The relatively low statistical power in the two studies should be taken into consideration as a source of variability in assessing dose effect relationship. Future studies with more statistical power will have to confirm the dose-related effect profile of gaboxadol. The finding that NSS was reduced with gaboxadol also suggests benefits on sleep continuity (Stepanski 2002).
In agreement with previous publications, zolpidem 10 mg increased TST. However, the pharmacological effect on sleep maintenance was not robust enough to have a significant effect on WASO or NAW, nor did it result in improved patient-rated sleep quality.
Neither doses of gaboxadol nor zolpidem had positive effects on sleep initiation in the present study. While a consistent effect on sleep initiation has previously been observed for zolpidem 10 mg in the treatment of patients with chronic insomnia (e.g. Scharf et al. 1994; Holm and Goa 2000), this questions whether the patient population had severe enough sleep onset problems to appropriately assess the efficacy of hypnotic on sleep initiation. This sleep-inducing effect is particularly marked in patients with prolonged sleep latency (i.e. >30 min) and is not always seen in studies of healthy volunteers (Brunner et al. 1991). Positive effects on sleep initiation have previously been observed following gaboxadol 15 mg using a similar study design (Deacon et al. 2007). A less severe patient population in combination with a different evaluation of sleep onset efficacy using latency to persistent sleep may help to explain the difference in effect between the two studies on sleep initiation. Indeed, the baseline characteristics for SOL in the patient population seem slightly shorter in the present study (45.5 min) compared to those of Deacon et al. (57.7 min, Deacon, personal communication). While both studies used advertisement as the main source for recruitment, the less severe patient population in this reported study does not seem to be a result of a smaller portion of severe treatment seeking patients but rather a result of a difference in selection criteria.
As expected based on previous findings in animals, normal healthy volunteers and patients, gaboxadol markedly enhanced SWS (“deep sleep”) duration in a dose-related manner, with no effects on stage 2 (“light sleep”) duration. This contrasts with the effect of zolpidem that, in this sample of patients suffering from insomnia, increased stage 2 sleep duration with no effects on SWS duration. A slight REM (and stage 1) suppressant effect was observed after gaboxadol 20 mg compared to placebo together with a delay in REM onset. While REM suppression was observed for gaboxadol 20 mg compared to placebo, there was no observable difference compared to baseline values. No REM suppression has been reported for gaboxadol in earlier studies with lower doses (Deacon et al. 2007; Walsh et al. 2007).
The elimination half-life of gaboxadol (approximately 1.5 h; Lund et al. 2005) is slightly shorter than that of zolpidem (approximately 2.5 h; Drover 2004), and yet, there appears to be a beneficial effect of gaboxadol on the sleep maintenance measures of wakefulness (number and duration). Traditionally, the prediction of sleep maintenance efficacy for benzodiazepine-site ligands such as zolpidem has focused on the pharmacokinetics of the drug. The described effect of gaboxadol on the sleep maintenance parameters of wakefulness (number and duration), which were not observed for zolpidem, indicates that the mechanism of action may also be important for the achieved hypnotic effects.
It has been suggested that differences between stage 2 (and spindle activity) and SWS (predominantly delta activity) result from different degrees of hyperpolarisation of thalamocortical neurons that implicate GABAergic mechanisms (Belelli et al. 2005; Steriade 2003). Gaboxadol may be more potent than zolpidem for inducing this hyperpolarisation resulting in more delta than spindle activities. More hyperpolarisation may result in a greater sleep-protective effect; in other words, internal or external sleep-disturbing stimuli need to be more sizeable to induce an arousal. This could explain why gaboxadol and not zolpidem lowers NAW. This is also reflected in reduced stage 1 sleep and reduced NSS because, for each awakening, there is a transition time through stage 1 to reach stage 2 sleep or higher. Moreover, the observed different spectral profile during NREM sleep following gaboxadol, i.e. increased slow wave activity and theta activity (Lundahl et al. 2006), may also play an important role in the regulation of the overall sleep maintenance.
Short-term use of gaboxadol 10 and 20 mg in patients with primary insomnia was generally well tolerated, although the severity of the adverse events appeared to be dose-related. Also, a gender effect was observed in the study, with females reporting more adverse events than males across all treatment arms (including placebo), but a proportionally greater increase was observed for gaboxadol 20 mg. The only two adverse events that were rated as severe in intensity (panic disorder and vomiting) both occurred in females in the gaboxadol 20 mg treatment arm. Previous human studies using gaboxadol doses up to 15 mg have not reported similar gender effects. Although larger studies will be necessary to confirm the therapeutic dose range, one may speculate that 20 mg as a bedtime dose exceeds the maximum therapeutic dose, especially in women.
Residual daytime sleepiness and impairment of psychomotor and cognitive functioning the day after bedtime administration is one of the main problems associated with the use of hypnotics (Vermeeren 2004). In the present study, next-day hangover effects were not observed in insomniac patients following a bedtime dose of 20 mg gaboxadol. Although the results would be further strengthened by the presence of a positive control, the observation seems valid based on the previously shown sensitivity of the test battery (O’Neill et al. 2000). Also, the 20-mg dose of gaboxadol seems clinically relevant based on its robust effects on sleep maintenance.
In conclusion, gaboxadol had a robust positive effect on sleep maintenance following a 20-mg dose in that it improves the PSG recorded wakefulness after sleep onset, NAW and TST. Patient-rated sleep quality was also improved following the 20-mg dose. Although improving sleep maintenance, both gaboxadol 10 mg and zolpidem 10 mg were not associated with a similar robust effect on sleep onset characteristics. Neither dose of gaboxadol nor the active reference zolpidem was associated with treatment effects on SOL, making general conclusions on the sleep-promoting properties of gaboxadol difficult. Gaboxadol, but not zolpidem, robustly and dose dependently enhanced SWS. Gaboxadol was generally well tolerated, but more frequent adverse events and an increased intensity of these events were observed at the 20-mg dose compared to the 10-mg dose. A gaboxadol dose up to 20 mg was not associated with any residual effects in the morning after bedtime administration.
References
American Psychiatric Association (1994) American Psychiatric Association diagnostic and statistical manual of mental disorders, 4th edn. American Psychiatric Association, Washington, DC
Belelli D, Peden DR, Rosahl TW, Wafford KA, Lambert JJ (2005) Extrasynaptic GABA(A) receptors of thalamocortical neurons: A molecular target for hypnotics. J Neurosci 25:11513–11520
Benington JH, Heller HC (1995) Restoration of brain energy metabolism as the function of sleep. Prog Neurobiol 45:347–360
Brunner DP, Dijk DJ, Munch M, Borbely AA (1991) Effect of zolpidem on sleep and sleep EEG spectra in healthy–young men. Psychopharmacology 104:1–5
Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh sleep quality index—a new instrument for psychiatric practice and research. Psychiatry Res 28:193–213
Deacon S, Staner L, Staner C, Legters A, Loft H, Lundahl J (2007) Effect of short-term treatment with gaboxadol on sleep maintenance and initiation in patients with primary insomnia. Sleep 30(03):281–287
Drover DR (2004) Comparative pharmacokinetics and pharmacodynamics of short-acting hypnosedatives: zaleplon, zolpidem and zopiclone. Clin Pharmacokinet 43:227–238
Drasbek K, Jensen K (2006) THIP, a hypnotic and antinociceptive drug, enhances an extrasynaptic GABAA receptor mediated conductance in mouse neocortex. Cereb Cortex 16(8):1134–1141
Ebert B, Wafford KA, Deacon S (2006) Treating insomnia: current and investigational pharmacological approaches. Pharmacol Ther 112:612–629
Faulhaber J, Steiger A, Lancel M (1997) The GABAA agonist THIP produces slow wave sleep and reduces spindling activity in NREM sleep in humans. Psychopharmacology (Berl) 130:285–291
Feinberg I, Maloney T, Campbell IG (2000) Effects of hypnotics on the sleep EEG of healthy young adults: new data and psychopharmacologic implications. J Psychiatr Res 34:423–438
Holm KJ, Goa KL (2000) Zolpidem: an update of its pharmacology, therapeutic efficacy and tolerability in the treatment of insomnia. Drugs 59:865–889
Horne J (1992) Human slow wave sleep: a review and appraisal of recent findings, with implications for sleep functions and psychiatric illness. Experientia 48:941–954
Jia F, Pignataro L, Schofield CM, Yue M, Harrison NL, Goldstein PA (2005) An extrasynaptic GABAA receptor mediates tonic inhibition in thalamic VB neurons. J Neurophysiol 94:4491–4501
Lancel M (1997) The GABA(A) agonist THIP increases non-REM sleep and enhances non-REM sleep-specific delta activity in the rat during the dark period. Sleep 20:1099–1104
Lancel M (1999) Role of GABAA receptors in the regulation of sleep: initial sleep responses to peripherally administered modulators and agonists. Sleep 22:33–42
Lancel M, Faulhaber J (1996) The GABAA agonist THIP (gaboxadol) increases non-REM sleep and enhances delta activity in the rat. Neuroreport 7:2241–2245
Lancel M, Wetter TC, Steiger A, Mathias S (2001) Effect of the GABAA agonist gaboxadol on nocturnal sleep and hormone secretion in healthy elderly subjects. Am J Physiol Endocrinol Metab 281:E130–E137
Lund J, Lundahl J, Nielsen GM, Mengel H (2005) The pharmacokinetic properties of gaboxadol, a new hypnotic, in young and elderly men. Sleep 28:A48
Lundahl J, Staner L, Deacon S (2006) Spectral profiles during NREM sleep for gaboxadol and zolpidem in the treatment of patients with primary insomnia. Sleep 29(abstract Suppl):A244
Mathias S, Steiger A, Lancel M (2001) The GABA(A) agonist gaboxadol improves the quality of post-nap sleep. Psychopharmacology (Berl) 157:299–304
Mathias S, Zihl J, Steiger A, Lancel M (2005) Effect of repeated gaboxadol administration on night sleep and next-day performance in healthy elderly subjects. Neuropsychopharmacology 30:833–841
Mitler MM (2000) Nonselective and selective benzodiazepine receptor agonists—where are we today? Sleep 23(Suppl 1):S39–S47
O’Neill W, Hanks G, Simpson P, Fallon M, Wesnes K (2000) The cognitive and psychomotor effects of morphine in healthy subjects: a randiomised controlled trial of repeated (four) oral doses of dextropropoxyphene, morphine, lorazepam and placebo. Pain 85:209–215
Orser BA (2006) Extrasynaptic GABAA receptors are critical targets for sedative–hypnotic drugs. J Clin Sleep Med 2(2):S12–S18
Parrino L, Terzano MG (1996) Polysomnographic effects of hypnotic drugs. A review. Psychopharmacology (Berl) 126:1–16
Parrott AC, Hindmarch I (1980) The Leeds sleep Evaluation Questionnaire in psychopharmacological investigations—a review. Psychopharmacology 71:173–179
Petursson H (1994) The benzodiazepine withdrawal syndrome. Addiction 89:1455–1459
Rechtschaffen A, Kales A (1968) A manual of standardized terminology, techniques and scoring system for sleep stages of human subject. National Institute of Health, publication 204. APT (Association of Polysomnographic Technologists). Government Printing Office, Washington, DC
Saper CB, Chou TC, Scammell TE (2001) The sleep switch: hypothalamic control of sleep and wakefulness. Trends Neurosci 24:726–731
Saper CB, Scammell TE, Lu J (2005) Hypothalamic regulation of sleep and circadian rhythms 1. Nature 437:1257–1263
Sateia MJ, Nowell PD (2004) Insomnia. Lancet 364:1959–1973
Scharf M, Roth T, Vogel WV, Walsh J (1994) A multicenter, placebo-controlled study evaluating zolpidem in the treatment of chronic insomnia. J Clin Psychiatry 55:192–199
Sigel E (2005) Mapping of the benzodiazepine recognition site on GABA-A receptors. Curr Top Med Chem 2:833–839
Stepanski EJ (2002) The effect of sleep fragmentation on daytime function. Sleep 25:268–276
Steriade M (2003) The corticothalamic system in sleep. Front Biosci 8:878–899
Steriade M, McCormick DA, Sejnowski TJ (1993) Thalamocortical oscillations in the sleeping and aroused brain. Science 262:679–685
Trachsel L, Dijk DJ, Brunner DP, Klene C, Borbely AA (1990) Effect of zopiclone and midazolam on sleep and EEG spectra in a phase-advanced sleep schedule. Neuropsychopharmacology 3:11–18
Vermeeren A (2004) Residual effects of hypnotics: epidemiology and clinical implications. CNS Drugs 18:297–328
Walsh JK, Deacon S, Dijk DJ, Lundahl J (2007) Gaboxadol improves sleep onset and maintenance and enhances low frequency components of NREM sleep EEG in a model of transient insomnia. Sleep 30(5):593–602
Acknowledgments
This study complied with the local country requirements for the conduct of clinical studies. This research was supported by H. Lundbeck A/S. J. Lundahl, H. Loft and S. Deacon are employees of H. Lundbeck A/S. L. Staner and C. Staner have received funding from H. Lundbeck A/S to perform the studies. The authors from both the sponsor company and clinical research organisation [Institute For Research in Neurosciences, Neuropharmacology and Psychiatry (FORENAP)] were involved in the study design, analysis, review and interpretation of the data and the writing and approval of the report and manuscript. All authors had full control of primary data. The authors would like to acknowledge the assistance of Annelies Legters (H. Lundbeck A/S) in monitoring the study, FORENAP staff in performing the study at the site, Francoise Calvi-Gries (FORENAP) in helping to analyse the data, and Christopher Lines (Merck Research) in helping us draft the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was funded by H. Lundbeck A/S.
Rights and permissions
About this article
Cite this article
Lundahl, J., Staner, L., Staner, C. et al. Short-term treatment with gaboxadol improves sleep maintenance and enhances slow wave sleep in adult patients with primary insomnia. Psychopharmacology 195, 139–146 (2007). https://doi.org/10.1007/s00213-007-0866-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-007-0866-0