
Abstract
In order to evaluate the usefulness of calcaneal quantitative ultrasound (QUS) in the assessment of male osteoporosis, a cross-sectional, population-based study was performed. A cohort of 4,832 men, randomly selected, community-dwelling, aged 60–80 years and representative of the general older male Italian population was recruited. QUS measurements were assessed in 83 centers distributed all over Italy and equipped with an Achilles device (GE-Lunar, Madison, Wisconsin, USA). All participants were administered a questionnaire covering lifestyle variables and medical history. Low-energy fractures that had occurred since age 50 were recorded. Overall, 43 subjects reported a previous hip fracture and 455 subjects reported other non-spinal fractures. Univariate analysis showed that fractured subjects were older, with a lower level of outdoor physical activity and a more frequent history of prolonged bedridden periods in comparison with unfractured subjects. Men reporting non-spinal fractures showed a higher prevalence of smoking, while no difference was found among groups in anthropometric measures and calcium intake. QUS measurements showed that all QUS parameters were significantly lower in both fracture groups ( p <0.001). Multiple logistic regression analysis demonstrated that each SD reduction in QUS measures was associated with an approximate doubling of the risk for hip fracture, independent of age and other clinical variables (broadband ultrasound attenuation [BUA]: odds ratio [OR]=2.24; 95% confidence interval [CI] 1.61–3.08; stiffness index: OR=2.19; CI 1.56–3.11; speed of sound [SOS]: OR=1.71; CI 1.18–3.24) and with an increase of the risk of other non-spinal fractures (BUA: 1.38; CI 1.22–1.59; stiffness index: OR=1.27; CI 1.17–1.38; SOS: OR=1.14; CI 0.96–1.40). It can be concluded that calcaneal QUS measurement is associated with the risk for hip fracture and any non-spinal fractures among a community-dwelling cohort of elderly men. The strength of the association between QUS measurement and fracture is similar to that observed in elderly women.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Osteoporotic fractures and mainly hip fractures are widely recognized as common and important causes of morbidity and mortality in the elderly [1]. There is uncertainty about the real prevalence of osteoporosis (OP) in men, but it has been estimated that about one-third of all fractures occur in men [2, 3], and more than 25% of the health expenditure attributable to osteoporotic fractures is recognized to be spent on treatment of males [4]. With the rise in the worldwide fracture incidence expected in the next years due to the progressive aging of the world’s male population [5] and the increasing awareness of male OP, a greater demand for reliable tools for identification of high-risk subjects is expected. Bone mineral density (BMD) measurement by DXA has been shown to be a good predictor for fracture risk in men [6, 7], but cheaper and more available technologies need to be developed.
In this setting, quantitative ultrasound (QUS) bone measurement seems to be able to meet the increasing demand for bone densitometry services. In recent years large prospective studies have demonstrated that QUS measurement can predict osteoporotic fractures in postmenopausal women as well as DXA measurements can [8, 9], but only sparse data are available for men. A few case-controlled studies showed that QUS discriminates between fractured and unfractured men [10, 11] and a prospective study based on a small sample of institutionalized people reported that QUS predicts the risk for fracture in elderly men [12]. Recently, Khaw et al. [13] have reported that QUS of the heel has the same predictive power of hip fracture in men as in women. Despite the limited number of events, this is the first prospective study on the value of QUS measurement in predicting hip fracture in men. Adami et al. [14] have recently showed in a wide population sample that risk factors usually associated with low BMD as measured by DXA are also associated with calcaneal bone stiffness as measured by QUS, and most risk factors usually observed in women are equally able to influence QUS measurement in men. These results have been achieved by a multicenter population-based study named ESOPO (Epidemiological Study On the Prevalence of Osteoporosis). ESOPO recruited a large cohort of randomly selected older community-dwelling women and men representative of the general Italian population.
Based on the same sample, the purpose of this study was to assess whether ultrasonographic measurement of the os calcis is associated with the risk of fracture in elderly men.
Materials and methods
Study population and instruments
In Italy all individuals are registered with a local general practitioner as part of the National Health Service. From these healthcare lists a random selection of 8,742 men aged 60–80 years was made. The relative distribution of selected subjects with respect to age and geographical location closely resembled the general Italian population. These subjects were asked to participate through 1,532 general practitioners involved in the study, and referred to 83 health centers distributed all over Italy equipped with an Achilles apparatus (GE-Lunar, Madison, Wisconsin, USA). As unique selection criteria, the study recruited non-institutionalized, community-dwelling, independently mobile elderly men, without severe cognitive impairment as judged by their primary-care physician. Of the whole sample, 4,981 men (57%) agreed to undergo QUS evaluation, without significant differences among northern, central and southern Italy, but with a relative attendance rate slightly higher for younger men. After correction of the original selected population for compliance rate and exclusion of subjects who were per-protocol deleted because of an incomplete drawing up of the questionnaire, data were collected from 4,832 men (median age 67.4 years). Among these, 3,223 subjects were aged 60–69 years and 1,609 were older than 70 years.
After obtaining informed consent, all subjects completed a self-administered questionnaire described in detail elsewhere [14] and covering lifestyle variables thought to be predictors of bone mass. Information was gathered on the following: smoking habits, consumption of alcohol, physical activity defined as the usual daily time spent outside walking (more than 30 min), calcium intake using as indicator the mean daily consumption of dairy products, and a history of being bedridden for more than 2 months. Finally, subjects were asked about their medical and drug-use history. Detailed information was also retrieved regarding fracture incidence since age 50 years. At the time of QUS measurement, the subjects were interviewed by a physician with regard to circumstances related to fractures. Fractures caused by severe trauma such as a traffic accident or a fall from a height or a staircase as well as all fractures of skull, face, finger, toe and vertebrae were excluded, and only low-trauma fractures (fall from a standing height or less) were considered. All reported hip fractures and 82% of other fractures were verified with the general practitioner by phone. The recruitment and QUS measurements were completed in 4 months, from March to June 2000.
Measurements
At the time of QUS measurement, height (measured by a stationary stadiometer) and weight (measured by a balance scale) were obtained from all subjects. QUS assessments were carried out with the Achilles device. All centers participating in the study were given a new instrument, and all instruments were calibrated and tested centrally before delivery. Before beginning the study, a protocol to standardize the methodology of the measurement was sent to each participating center. All instruments were calibrated daily in accordance with the manufacturer’s recommendations and in each center all measurements were done by the same operator. QUS measurements were performed at the right os calcis. In the case of a previous fracture within the right lower extremity, the contralateral calcaneus was measured. The broadband ultrasound attenuation (BUA) and speed of sound (SOS) were measured. The stiffness index (SI), a composite parameter obtained by a mathematical combination of BUA and SOS, was calculated by the software of the device and expressed as a percentage of young normal values. Compliance with the measurement procedures was regularly checked by ten coordinating centers that provided assistance to the local centers. The coefficients of variation were assessed in each center by a delegate of the coordinating centers and calculated from three cohort members scanned five times on the same day. The mean coefficients of variation were 2.1% for BUA (range, 1.4–2.6%), 0.3% for SOS (0.1–0.5%) and 1.8% for SI (1.2–2.1%).
Statistical analysis
After checking for normality of the distribution (Shapiro-Wilks test), parametric tests were applied to perform comparisons between fractured and unfractured subjects. Student’s t -test for unpaired data was used for continuous variables and chi-square test for categorical variables. To assess the association of QUS parameters with fracture risk, multiple logistic regression analyses were performed. In the first analysis the crude relative risk of hip fracture and all other non-spinal fractures was calculated for a 1 standard deviation decrease in BUA, SOS and SI. We then adjusted for age and other clinical variables that were significantly associated with QUS measures at the level of <0.05, such as weight, calcium intake, current smoking, regular walking outside, and a history of being bedridden. Results are presented as the odds ratios (OR) and 95% confidence intervals (CI) for hip fracture and other non-spinal fractures. SAS statistical software was used for the analyses.
Results
Data on the fracture groups and unfractured subjects are shown in Table 1. Among our sample, 498 men (10.3%) had sustained at least one low-trauma fracture and among these subjects 43 men reported a previous hip fracture. Subjects with previous low-energy fractures referred 552 fractures. Because vertebral fractures were excluded by design, fractures were mainly appendicular. A slightly higher prevalence of fractures of the upper extremity (41.9%) was found with 168 (30.4%) wrist fractures, 29 (5.2%) fractures of the proximal humerus, and 35 (6.3%) other upper extremity fractures. Overall, fractures of the lower extremity were 208 (37.7%). Besides hip fractures (7.8%), 165 fractures (29.9%) concerned the femur, tibia, ankle and foot. Rib fractures were 59 (10.7%), and pelvic and clavicle fractures were 53 (9.6%). Twenty-two men aged 60–69 years reported hip fractures and 254 reported other non-spinal fractures. Among subjects older than 70 years, 21 reported a previous hip fracture and 201 subjects reported other non-spinal fractures.
When compared with unfractured subjects, both men with hip fracture and those with other non-spinal fractures were significantly older (respectively, p <0.05 and p <0.001), whereas, no difference in anthropometric measures was found, and chronic disease prevalence rates did not show any significant difference between groups. By comparison with the unfractured group, a greater prevalence of a history of prolonged bedridden periods (unrelated to fracture) was found both in subjects with a previous hip fracture ( p <0.001) and men with other non-spinal fractures ( p <0.001).
Regarding health practice variables, the prevalence of current smoking was higher in men with non-spinal fractures ( p <0.05), whereas, no difference was found in mean dairy calcium intake and daily intake of alcohol among groups. Significant differences were seen for regular walking outside. Thus, the proportion of men reporting daily walking outside greater than 30 min was higher in unfractured men in comparison with subjects with hip fracture ( p <0.001) and men with other previous non-spinal fractures ( p <0.01). Finally, all QUS parameters showed significantly lower values in both fractured groups ( p <0.001) compared with unfractured subjects.
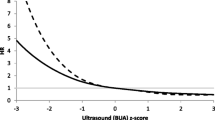
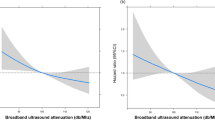
In Table 2 are shown the odds ratios for hip fracture and all non-spinal fractures. After adjustment for age and other clinical variables such as weight, dairy calcium intake, current smoking, regular walking outside, and a history of bedridden periods, a decrease of 1 SD in BUA was associated with an increased risk of hip fracture as great as 2.24 (95% CI 1.61–3.08) and a 38% increase in the risk for other non-spinal fractures (OR=1.38; 95% CI 1.22–1.59). A decrease of 1 SD in calcaneal SI increased the risk of hip fracture by 2.19 (95% CI: 1.56–3.11), and the risk of non-spinal fractures by 1.27 (95% CI: 1.17–1.38). The association between SOS and fracture risk was slightly weaker: each 1 SD decrease was associated with a 71% increase in the risk for hip fracture (OR=1.71; 95% CI 1.18–3.24) and a 14% increase of other non-spinal fractures (OR=1.14; 95% CI 0.96–1.40).
After splitting the sample according to decade, no relevant difference was found in odd ratio values between men younger and older than 70 years (data not shown). Instead, by considering the type of fracture divided into upper or lower extremity fractures, a slightly stronger association of QUS parameters with fractures of the lower extremity was observed: after adjusting for age and other clinical variables, the fracture risk estimates for the lower extremity in comparison with the upper extremity were 2.06 (1.54–2.71) vs 1.51 (1.18–2.04) for BUA; 1.90 (1.42–2.66) vs 1.35 (1.14–1.98) for SI; and 1.52 (1.06–2.04) vs 1.24 (0.92–1.61) for SOS.
Discussion
In this study we found that lower values of QUS parameters are associated with previous hip fracture and other non-spinal fractures among a population of community-dwelling elderly men. These results sustain the value of QUS measurement in assessing the risk of fragility fractures. Unlike most previous cross-sectional studies on male OP assessed by QUS, participants were not selected on the basis of the presence of fractures or already diagnosed as having OP, and they were not institutionalized. We recruited a large sample of unselected population living at home that closely resembles the general Italian male population aged 60–80 years. The two-fold increase in the relative risk of hip fracture for each 1 SD reduction in QUS measures is similar to what has been reported in other QUS case-control studies on males [10, 11] and in prospective studies on older females [8, 9]. The weaker relationship between the reduction in QUS parameters and the risk of other non-spinal fractures as compared with hip fracture is consistent with other studies. It is likely that these fractures are more closely associated with other variables that can independently influence the risk of appendicular fractures such as propensity to fall, frailty, visual acuity and response to falling [15]. In this regard can be viewed the stronger associations observed with fractures of the lower extremity in comparison with fractures of the upper extremity.
Adami et al. [14] have recently reported on the same population of this study that many of the risk factors associated with OP such as age, weight, calcium intake, smoking and physical activity are able to affect SI values assessed by QUS not only in women but also in men. Most of these factors are also associated with fracture risk and this may allow designing a “case finding” strategy, where clinical risk factors in conjunction with QUS measurement could be used to accurately predict the individual risk for fracture.
In agreement with the results of other cross-sectional studies on male OP [11, 16], patients with hip fracture showed higher values of QUS parameters in comparison with female samples with similar age and previous hip fractures [17, 18]. This result could be consistent with similar observations made in studies that examined BMD measured by DXA in fractured men and women. Despite an average higher BMD in fractured men than women [19], retrospective and prospective studies showed that fracture risk increases as BMD decreases in men in the same way as in women and, for any given BMD, the estimates of hip fracture risk are similar between sexes [7, 20]. As for BMD, differences of QUS values between fractured men and women could be related to a different distribution of QUS measures within the population with SD values of QUS parameters that differ between sexes. An alternative hypothesis would be that QUS measurement captures differences in microarchitectural changes between osteoporotic men and women [21, 22] or variables related to bone size or geometry [23].
This study has some strengths and weakness. The sample size and selection criteria with respect to the representativeness of the general population aged 60–80 years probably allow us to generalize these results to the whole Italian male population. The most obvious limitations of the study are related to its cross-sectional nature. Unlike longitudinal studies, cross-sectional data permit only limited interpretation of to what extent QUS measurement really predicts the risk of fracture. For example, it remains uncertain whether the collected QUS data reflect pre-fracture values, since fractures per se may have contributed to changes in bone structure due to immobilization or change in gait. Furthermore, even if this study was based on a large and unselected sample, we cannot exclude that results may be biased from cohort effects or survivor bias.
It has been recently reported in a prospective study that QUS measurement is as effective as DXA scan for assessing fracture risk [13]. Thus QUS bone evaluation for its low cost can be considered a suitable answer to face the expected increasing number of male patients attending OP clinics and seeking advice for prevention or therapy of their bone disease.
In conclusion, this study has provided evidence that QUS measurement is associated with the risk for hip fracture and any non-spinal fractures among a community-dwelling cohort of elderly men. The magnitude of odds ratios and the width of the confidence intervals suggest that the strength of this association is similar in men and postmenopausal women. Consistent with these findings, QUS measurement could be considered a suitable tool for identification of elderly men with a high risk of osteoporotic fractures and candidates for therapeutic intervention.
References
Melton LJ 3rd (1993) Hip fractures: A worldwide problem today and tomorrow. Bone 14:S1–S8
Jones G, Nguyen T, Sambrook PN, Kelly PJ, Gilbert C, Eisman JA (1994) Symptomatic fracture incidence in elderly men and women: the Dubbo Osteoporosis Epidemiology Study (DOES). Osteoporos Int 4:277–282
Seeman E (2001) Unresolved issues in osteoporosis in men. Rev Endocr Metab Disord 2:45–64
Melton LJ 3rd, Thamer M, Ray NF et al (1997) Fracture attributable to osteoporosis: Report from the National Osteoporosis Foundation. J Bone Miner Res 12:16–23
Cooper C, Campion G, Melton LJ 3rd (1992) Hip fracture in the elderly: a world-wide projection. Osteoporos Int 2:285–289
Nyquist F, Gardsell P, Sernbo I, Jeppsson JO, Johnell O (1998) Assessment of sex hormones and bone mineral density in relation to occurrence of fracture in men: a prospective population-based study. Bone 22:147–151
De Laet CE, Van Hout BA, Burger H, Weel AE, Hofman A, Pols HA (1998) Hip fracture prediction in elderly men and women: validation in the Rotterdam study. J Bone Miner Res 10:1587–1593
Hans D, Dargent-Molina P, Schott AM et al (1996) Ultrasonographic heel measurements to predict hip fracture in elderly women: the EPIDOS study. Lancet 348:511–514
Bauer DC, Glüer CC, Cauley JA et al (1997) Broadband ultrasound attenuation predicts fractures strongly and independently of densitometry in older women. Arch Intern Med 157:629–634
Pluskiewicz W, Drozdzowska B (1999) Ultrasound measurements at the calcaneus in men: differences between healthy and fractured persons and the influence of age and anthropometric features on ultrasound parameters. Osteoporos Int 10:47–51
Mulleman D, Legroux-Gerot I, Duquesnoy B, Marchandise X, Delcambre B, Cortet B (2002) Quantitative ultrasound of bone in male osteoporosis. Osteoporos Int 13:388–393
Pluijm SMF, Graafmans WC, Bouter LM, Lips P (1999) Ultrasound measurements for the prediction of osteoporotic fractures in elderly people. Osteoporos Int 9:550–556
Khaw KT, Reeve J, Luben R et al (2004) Prediction of total and hip fracture risk in men and women by quantitative ultrasound of the calcaneus: EPIC-Norfolk prospective population study. Lancet 363:197–202
Adami S, Giannini S, Giorgino R et al (2003) The effect of age, and lifestyle factors on calcaneal quantitative ultrasound: the ESOPO study. Osteoporos Int 14:198–207
Prudham D, Evans JG (1981) Factors associated with falls in the elderly: a community study. Age Ageing 10:141–146
Karlsson MK, Duan Y, Ahlborg H, Obrant KJ, Johnell O, Seeman E (2001) Age, gender, and fragility fractures are associated with differences in quantitative ultrasound independent of bone mineral density. Bone 28:118–122
Turner CH, Peacock M, Timmerman L, Neal JM, Johnston CC (1995) Calcaneal ultrasonic measurements discriminate hip fracture independently of bone mass. Osteoporos Int 5:130–135
Schott AM, Weill-Engerer S, Hans D, Duboeuf F, Delmas PD, Meunier PJ (1995) Ultrasound discriminates patients with hip fracture equally well as dual energy X-ray absorptiometry and independently of bone mineral density. J Bone Miner Res 10:243–249
Orwoll E (2000) Perspective: Assessing bone density in men. J Bone Miner Res 15:1867–1870
Kanis JA, Johnell O, Oden A, Dawson A, De Laet C, Jonsson B (2001) Ten-year probabilities of osteoporotic fractures according to BMD and diagnostic thresholds. Osteoporos Int 12:989–995
Aaron J, Makins N, Sagreiya K (1987) The microanatomy of trabecular bone loss in normal aging men and women. Clin Orthop 215:260–271
Parfitt AM, Mathews CH, Villanueva AR, Kleerekoper M, Frame B, Rao DS (1983) Relationships between surface, volume, and thickness of iliac trabecular bone in aging and in osteoporosis: Implications for the microanatomic and cellular mechanisms of bone loss. J Clin Invest 72:1396–1409
Nicholson PH, Muller R, Lowet G et al (1998) Do quantitative ultrasound measurements reflect structure independently of density in human vertebral cancellous bone? Bone 23:425–431
Acknowledgements
This work was totally funded by an unlimited grant from Procter and Gamble, Rome, Italy
Author information
Authors and Affiliations
Corresponding author
Appendix: Local coordinators of the ESOPO study
Appendix: Local coordinators of the ESOPO study
Antonino Accardi, Marsala (TP); Alberto Angeli, Orbassano (TO); Salvatore Baglio, Roma; Alfonso Baldoncini, Arezzo; Pierluigi Ballardini, Lagosanto (FE); Cataldo Bancheri, Roma; Franco Beghe, Imperia; Luigi Bernini, S. Miniato (PI); Maurizio Bevilacqua, Milano; Gerolamo Bianchi, Arenzano (GE); Giuseppe Bonomi, Palmanova (UD); Massimo Bottai, Sarzana (SP); Giovanni Brogi, Pescia (PT); Giuseppe Candioto, Agrigento; Sergio Candiotto, Dolo (VE); Riccardo Cecchetti, Pontedera (PI), Raffaele Cerqua, S. Felice a Cancello (CE); Sandro Cervelli, Roma; Stefano Coaccioli, Terni; Franco Coin, Dolo (VE); Cataldo Colella, Aversa (CE); Daniele Costi, Parma; Massimo Cravero, Torino; Salvatore D’Auria, Benevento; Giovanni D’Avola, Catania; Nicola De Gennaro, Capua (CE); Lucio Del Forno, Vasto (CH); Arturo D’Elia, Napoli; Ombretta Di Munno, Pisa; Roberto Di Virgilio, Treviso; Filippo Favazzi, Mistretta (ME); Mario Ferraris, Vercelli; Paolo Filipponi, Umbertide (PG); Cristiano Maria Francucci, Ancona; Bruno Frediani, Siena; Giorgio Gandolini, Milano; Romildo Gasparini, Legnago (VR); Romeo Gatti, Viterbo; Salvatore Gatto, Napoli; Ernesto Gemini, Napoli; Tommaso Gismondi, Bari; Stefano Gonnelli, Siena; Siro Grassi, Napoli; Giovanni Iolascon, Napoli; Giancarlo Isaia, Torino; Tommaso Izzo, Nocera Inferiore (SA); Giovanni La Montagna, Napoli; Renato La Forgia, Matera; Giovanni Lapadula, Bari; Gaetano Loiacono, Martina Franca (TA); Pierluigi Lombardi, Castelnuovo (LU); Roberto Lovato, Vicenza; Riccardo Maglitto, Lentini (SR); Fabio Magnani, Vignola (MO); Nazzarena Malavolta, Bologna; Giorgio Mancini, Macerata; Giuseppe Masellis, Carpi (MO); Domenico Maugeri, Catania; Carmelo Micale, Cuggiono (MI); Redento Mora, Pavia; Maurizio Muratore, S. Cesario di Lecce (LE); Rita Occhipinti, Belluno; Geremia Oliva, Frattamaggiore, (NA); Ernesto Palummeri, Genova; Domenica Panzavecchia, Partinico (PA); Salvatore Parello, Canelli (AT); Raffaele Pellerito, Torino; Giovanni Pisanu, Oristano (CA); Domenico Policicchio, Avellino; Marco Pozone, L’Aquila; Giulio Pucci, Spoleto (PG); Stefano Respizzi, Rozzano (MI); Giuseppe Roberti, Chivasso (TO); Maurizio Rossini, Verona; Sergio Rossitto, Piazza Armerina (EN); Luciano Sabadini, Arezzo; Carlo Salvarani, Reggio Emilia; Salvatore Salvini, Anzio (RM); Giuseppe Santeufemia, Iglesias (CA); Ivana Santi, Milano; Leonardo Sartori, Padova; Mario Sfrappini, S. Benedetto del Tronto (AP); Ferdinando Silveri, Jesi (AN); Luigi Sinigaglia, Milano; Michele Soriano, Vibo Valentia; Ruggero Spinazze, Conegliano (TV); Giuseppe Stancati, Cosenza; Giancarlo Tartarelli, Massa; David Topini, Viterbo; Francesco Trotta, Ferrara; Giuseppe Varcasia, Castrovillari (CS); Alfredo Zanatta, Legnago (VR)
Rights and permissions
About this article
Cite this article
Varenna, M., Sinigaglia, L., Adami, S. et al. Association of quantitative heel ultrasound with history of osteoporotic fractures in elderly men: The ESOPO study. Osteoporos Int 16, 1749–1754 (2005). https://doi.org/10.1007/s00198-005-1914-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-005-1914-4