
Abstract
Introduction and hypothesis
Some patients with hip osteoarthritis report that urinary incontinence (UI) is improved following total hip arthroplasty (THA). However, the type and severity of UI remain unclear. In this study, we hypothesize that both stress urinary incontinence (SUI) and urge urinary incontinence (UUI) are improved after THA. We assess the characteristics of UI and discuss the anatomical factors related to UI and THA for improved treatment outcome.
Methods
Fifty patients with UI who underwent direct anterior-approach THA were evaluated. Type of UI was assessed using four questionnaires: Core Lower Urinary Tract Symptom Score (CLSS), Urogenital Distress Inventory Short Form (UDI-6), International Prostate Symptom Score (IPSS), and Overactive Bladder Symptom Score (OABSS). Uroflowmetry and postvoid residual urine were measured using ultrasound technology. Hip-joint function was evaluated using Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) and range of motion (ROM).
Results
Of the 50 patients, 21 had SUI, 16 had mixed urinary incontinence (MUI), and eight had urgency urinary incontinence (UUI). In total, 36 patients were better than improved (72 %). The rate of cured and improved was 76 % for SUI, 100 % MUI, and 50 % UUI. The improvement of ROM was more significant in cured or improved patients than in stable or worse patients.
Conclusions
Improvement in mild UI may be an added benefit for those undergoing THA for hip-joint disorders. These data suggest that for patients with hip-joint disorder, hip-joint treatment could prove to also be a useful treatment for UI.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Urinary incontinence (UI) and overactive bladder (OAB) are stressful conditions common throughout the world [1]. The symptoms are not related to mortality; however, they can cause considerable impairment in various aspects of daily life and greatly reduce the quality of life (QOL) [2]. With the global increase in life expectancy, UI and OAB are increasingly important diseases that require treatment.
Japan has been a super-aged society for 10 years, and these conditions are on the increase. According to results of an epidemiological study, the prevalence of OAB in men and women >40 years is 12.4 % (8.1 million) and tends to increase with age [3]. Hip osteoarthritis is a common condition that many people develop during middle age or older. It is an important cause of pain and physical disability. In Japan, in the majority of patients with secondary osteoarthritis, it is primarily due to congenital dislocation or acetabular dysplasia. The prevalence of hip osteoarthritis is particularly high among middle-aged and elderly women [4–6]. Numerous treatment options are available to help relieve pain and improve mobility, and to help this condition, total hip arthroplasty (THA) is one of the most successful procedures in the orthopedic field [7]. Some patients report that their symptoms of UI have decreased following THA. In our institution, Tamaki et al. [8] found that the mean International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) score in patients with UI before surgery improved by 64 % at 3 months after THA. However, details on type or severity of UI were not discussed.
In this study, we hypothesized that both stress (SUI) and urge (UUI) urinary incontinence could be improved with the recovery of hip-joint function. We prospectively evaluated the clinical outcomes of THA and symptoms of UI before and after THA. We used several questionnaires to evaluate type and severity of UI. We also discuss the anatomical basis of the relationship between UI and THA.
Methods
Patient background
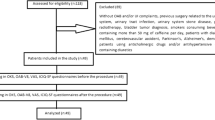
From September 2012 to March 2014, 1025 female patients underwent THA in our institution. The study population consisted of 83 of them who were examined by a urologist (KO), during this period. The details of the patients who came to the clinic on the day of the urologist’s presence was not purposely different from those who came on other days; therefore, the 83 patients were thought to be chosen randomly from the total 1025 patients. Patients with UI were defined as those who answered I have had an episode of UI and whose presurgery scores (for items SUI and UUI) in the core lower urinary tract symptom score (CLSS) exceeded 1. Whereas those who answered I have not had an episode of UI and whose scores in the CLSS were 0 prior to surgery, were defined as patients without UI. Of the 83 patients, 56 were diagnosed with UI, and of them, 50 could participate in all postsurgery assessments; one patient refused postsurgery assessment. There was partial loss of data for five. Thus, 50 patients with UI were evaluated.
Characteristics of the 50 patients are listed in Table 1. Average participant age was 62.9 ± 8.5 years, duration of arthrosis condition 8.1 ± 9.4 years, height 153.8 ± 5.8 cm, weight 53.7 ± 11.2 kg, body mass index (BMI) 22.7 ± 4.2 kg/m2, parity 1.74 ± 0.9, and birth weight 3081 ± 328 g. Simultaneous bilateral THA was performed in 15 of these patients. During the research period, no patient received medication for or surgical treatment for UI.
Surgical procedure
The direct anterior approach was used in all hips, with the patients in the supine position on a standard surgical table [9]. Postoperative rehabilitation was started on the first day. Both active- and passive-motion exercises of the involved joint and full weight bearing were allowed for all patients on the first day. To prevent early postoperative dislocation, deep flexion with internal rotation and hyperextension with external rotation of the hip joint were prohibited for 3 weeks after the surgery. After that time, no precautions were taken in order to avoid postoperative dislocation.
Questionnaire
We asked patients to complete the CLSS [10], Urogenital Distress Inventory Short Form (UDI-6) [11], International Prostate Symptom Score (IPSS) [12, 13], and Overactive Bladder Symptom Score (OABSS) [14] before surgery. Patients with UI before surgery were asked to again complete the same questionnaires at 3 days and 3 months after surgery. Individuals whose scores for items SUI and UUI in the CLSS were 0 at 3 months after surgery were defined as cured. Individuals whose scores improved by >1 were defined as improved. Individuals whose scores did not change were defined as stable. Patients whose scores worsened by at least 1 were defined as worse.
Uroflometry and residual urine
We also performed uroflowmetry (LIFE-TECH, MicrofloII) and measured postvoid residual (PVR) using ultrasound technology (Bladder Scan BVI 6100). These examinations were performed before and at 3 days and 3 months after surgery.
Evaluation of hip joint function: WOMAC and ROM
Hip function was evaluated using the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) [15]. The maximum WOMAC score is 96 points and is the sum of separate scores for pain (20 points), stiffness (8 points), and physical function (68 points). Range of motion (ROM) refers to the amount of movement that a particular joint or body part can move as measured in degrees. Common joint movements include flexion, extension, abduction, adduction, external rotation, and internal rotation.
Statistical analyses
Statistical processing was performed using the Excel application (Microsoft Office 2013. Student’s paired or unpaired t test was applied to evaluate differences, and the level of statistical significance applied was p < 0.05.
Ethical approval
The study was carried out with the approval of the Board of Ethics of Funabashi Orthopedic Hospital (No. 2012020).
Results
Questionnaires: CLSS, UDI-6, IPSS, OABSS
CLSS: Urgency significantly improved from 0.98 ± 0.89 before THA to 0.44 ± 0.57 at 3 days afer (p < 0.01) and 0.52 ± 0.73 at 3 months after(p < 0.01) (Fig. 1). Urge urinary incontinence (UUI) significantly improved from 0.64 ± 0.63 before to 0.36 ± 0.59 at 3 days (p < 0.05) and 0.28 ± 0.6 at 3 months (p < 0.01) after. Stress urinary incontinence (SUI) significantly improved from 0.98 ± 0.62 before to 0.36 ± 0.52 at 3 days (p < 0.01) and 0.28 ± 0.53 at 3 months (p < 0.01) after. QOL score significantly improved from 3.52 ± 1.5 before to 2.58 ± 1.77 at 3 days (p < 0.01) and 2.14 ± 1.37 at 3 months (p < 0.01) after. According to CLSS score, before THA, UI severity was relatively mild. Concerning UUI, 24 patients answered rarely and four patients answered sometimes; no patient answered often. Concerning SUI, 31 patients answered rarely and 11 answered sometimes; no patient answered often.

Questionnaires before and after total hip arthroplasty (THA): CLSS Core Lower Urinary Tract Symptom Score, UDI-6 Urogenital Distress Inventory Short Form, IPSS International Prostate Symptom Score, OABSS Overactive Bladder Symptom Score
UDI-6: Frequency improved from 19.3 ± 24.3 before THA to 12.7 ± 23.1 at 3 days after and significantly improved to 10.0 ± 21.5 at 3 months after (p < 0.05) (Fig. 1). UUI improved from 20.6 ± 26.8 before to 14.0 ± 24.3 at 3 days and significantly improved to 8.0 ± 18.5 at 3 months (p < 0.01) after. SUI improved from 20.6 ± 22.2 before to 12.7 ± 20.1 at 3 days and significantly improved to 8.0 ± 15.9 at 3 months (p < 0.01) after. Small leakage significantly improved from 26.0 ± 22.6 before to 16.7 ± 22.6 (p < 0.05) at 3 days and 10.7 ± 22.6 at 3 months (p < 0.01) after. No significant difference was observed in difficulty and pain before and after THA.
IPSS: Incomplete emptying improved from 0.56 ± 0.91 before THA to 0.28 ± 0.57 at 3 days and significantly improved to 0.22 ± 0.55 at 3 months (p < 0.05) after (Fig. 1). Frequency significantly improved from 1.78 ± 1.45 before to 1.16 ± 1.18 at 3 days (p < 0.05) and improved to 1.36 ± 1.27 at 3 months after THA. Urgency improved from 1.36 ± 1.48 before to 0.96 ± 1.28 at 3 days and significantly improved to 0.62 ± 1.01 at 3 months (p < 0.05) after. QOL score significantly improved from 3.46 ± 1.55 before to 2.48 ± 1.71 at 3 days (p < 0.01) and 2.12 ± 1.42 at 3 months (p < 0.01) after
OABSS: Urgency significantly improved from 1.46 ± 1.47 before THA to 0.82 ± 1.16 at 3 days after (p°
< 0.05) and 0.84 ± 1.18 at 3 months after (p < 0.05) (Fig. 1). UUI improved from 0.88 ± 1.13 before to 0.62 ± 1.03 at 3 days after and significantly improved to 0.42 ± 0.97 at 3 months after (p < 0.05).
Improvement of UI evaluated by CLSS
For the 50 patients in this study, according to the CLSS, 22 had SUI, 18 had MUI, and ten had UUI. In total, 37 patients were better than improved (74 %) and 13 worse than stable (26 %). The rate of improvement was different among UI types: In the 22 patients who had SUI before THA, 14 were cured, two were improved, five were stable, and one had de novo UUI after; of the 18 who had MUI before THA, 12 were cured, five were improved, and one was stable; in the ten who had UUI before THA, four were cured, four were stable, one was worse, and one was de novo SUI after THA. The rate of cured and improved was 73 % in SUI, 94 % in MUI, and 40 % in UUI.
Uroflometry and residual urine
Voided volume (VV) was significantly decreased from 173.9 ± 140 ml before THA to 118.5 ± 91.2 ml at 3 daysafter, but it returned to 183.8 ± 131.7 ml at 3 months (Fig. 2). Postvoid residual urine volume (PVR) was 5.5 ± 20.4 ml before THA, 6.5 ± 21.7 ml at 3 days after, and 5.8 ± 27.1 ml at 3 months after. All the values were within the normal range. In uroflowmetry, maximum flow rate (Qmax) was 19.6 ± 13.1 ml/s before THA, 18.0 ± 13.1 ml/s at 3 days after, and 21.4 ± 12.7 ml/s at 3 months after No significant difference was observed in Qmax before and after THA.

Uroflometry and residual urine before and after total hip arthroplasty (THA). VV voided volume, PVR postvoid residual, Q max maximum flow rate
Evaluation of hip-joint function
According to WOMAC, pain significantly improved from 9.15 ± 4.4 before THA to 1.85 ± 1.91 at 3 months after (p < 0.01). Stiffness significantly improved from 3.63 ± 1.8 before to 1.53 ± 1.36 at 3 months after (p < 0.01). Physical Function significantly improved from 29.9 ± 14.5 before to 7.39 ± 6.14 at 3 months after (p < 0.01). Total score significantly improved from 44.4 ± 20 before to 11.1 ± 8.5 at 3 months after (p < 0.01).When assessing ROM, flexion significantly improved from 79.0 ± 22.8 before THA to 98.6 ± 14.6 at 3 months after (p < 0.01) (Table 2). Extension significantly improved from 7.2 ± 7.9 before to 10.5 ± 5.5 at 3 months after (p < 0.05). Abduction significantly improved from 15.5 ± 8.6 before to 21.3 ± 8.3 at 3 months after (p < 0.01). Internal rotation significantly improved from 15.8 ± 12.7 before to 30.3 ± 10.1 at 3 months after (p < 0.01) (Table 2).
Correlation between improvement of UI and hip function
Improvement in ROM was compared between cured or improved and stable or worse patients (Fig. 3). No significant difference was observed either before or after THA between these groups However, there were some differences in improvement of ROM. Flexion, extension, abduction, and internal rotation were significantly improved at 3 months after THA in cured or improved patients. Flexion significantly improved from 78.4 ± 22.3 before to 98.8 ± 14.7 at 3 months after (p < 0.01). Extension was significantly improved from 6.5 ± 8.1 before to 11.1 ± 5.9 at 3 months after (p < 0.05). Abduction was significantly improved from 15.1 ± 8.0 before to 21.9 ± 7.6 at 3 months after (p < 0.01). Internal rotation was significantly improved from 14.6 ± 13.6 before to 30.0 ± 10.4 at 3 months after (p < 0.01). In the stable or worse group, only internal rotation was significantly improved—from 20.2 ± 13.4 before to 31.4 ± 7.8 at 3 months after (p < 0.05).

Improvement in the range of motion (ROM) before and after total hip arthroplasty (THA)
Difference between unilateral and bilateral arthroplasty was compared. Preoperational IPSS total score was more severe in the bilateral group; however, the difference concerning UI improvement was negligible.
Discussion
Morbidity associated with UI
Kikuchi et al. [16] showed that a high physical activity level was independently related to a lower self-reported prevalence of UI in a community-dwelling elderly population aged >70 years. The prevalence rate of UI before THA was 33 % reported by Tamaki et al. [8] and 28.9 % reported by Baba et al. [17]. In our study, CLSS revealed that 67 % (56/83) of patients were diagnosed with UI. In the previous studies, an orthopedic surgeon diagnosed UI, whereas in this study, a urologist diagnosed UI. This could be one reason for the differences.
Concerning the type of UI in Japanese women: SUI is reported to be more common than UUI [18]. In addition, the prevalence rate for UUI of one or more times in 1 week was 16 % and SUI of one or more times in 1 week was 19 % in Japanese women aged 40 years or older. In our study, 47 % had SUI, 18 % had UUI, and 35 % had MUI. This prevalence is similar to a former study that was not restricted to patients with osteoarthritis of the hip: 49 % SUI, 11 % UUI, and 36 % MUI in the EPINCONT study in Norway [19].
Among these questionnaires, CLSS was the most representative for evaluating the frequency of UI. On the other hand, UDI-6 was the most useful for evaluating patient concerns. As questions concerning SUI and UUI were independently asked in these two questionnaires, the severity of symptoms could be evaluated clearly.
Correlation among UI types
In this study, improvement was observed in SUI, MUI, and UUI. The rate of cured and improved was highest in MUI. This could be related to the severity of UI among types. In MUI patients, UI score before THA was milder than in other patient groups. SUI score was 1.27 ± 0.44 in the SUI group but 1.17 ± 0.38 in MUI group. UUI score was 1.30 ± 0.48 in UUI group, and1.06 ± 0.24 in MUI group. Although there was no significant difference, these differences did have some influence on improvement.
Immediate improvement of UI
The direct anterior approach was used in all hips. Postoperative rehabilitation was begun on the first day. Both active and passive motion exercises of the involved joint and full weight-bearing were allowed for all patients on the first day. Improvement of urinary continence was already observed at 3 days after the operation. Following this surgery, patients are in the phase of gait training, so they still have some difficulty walking. This means the improvement in urinary continence function is not directly explained by walking stability.
Relationship between pelvic muscles and hip joint
The obturator internus, gemelli, and quadratus femoris muscles are rotator muscles surrounding the hip joint. In addition to their morphology, their innervation pattern shows that they work together as a single muscle mass [20]. Many researchers have reported that the iliococcygeus muscle arises from the arcus tendinous levatoris ani situated on the obturator fascia [21–27]. The pubococcygeus is a lateral compressor of various visceral canals that cross the pelvic floor [28]. The puborectalis part reduces the anteroposterior dimension of the anourogenital hiatus. The iliococcygeus and, to a lesser extent, the less muscular ischiococcygeus, together with the puborectalis, contribute to anorectal and UI.
There is a special relationship between the medial portion of the levator ani muscle (pubococcygeus portion), the arcus tendinous fasciae pelvis, and the suburethral layer of the endopelvic fascia in the region of the proximal urethra, which facilitates contraction of the levator ani muscles to control the position of the vesical neck [29]. According to Kim et al. [30], the medial portion of the pubovisceral muscle origin has a relatively direct connection to the bone adjacent to the inner surface of the obturator internus muscle. The lateral portion of the pubovisceral muscle pubic origin attaches to the levator arch that runs from the pubic bone to the ischial spine at the site where the pubovisceral muscle joins the iliococcygeal muscle.
The muscles around the hip joint, including the obturator internus muscle, are less mobile in patients with hip osteoarthritis. Tension in these muscles seems to decrease due to the loss of the hip’s range of motion. Following THA, these muscles can become tense due to muscle strengthening and improvement of the hip’s range of motion. Based on anatomical studies, the levator ani and obturator internus have been shown to have a close relationship. However, the functional relationship between these muscles is unclear. The present findings showed that the improvement of hip-joint function correlated with the improvement of urinary continence function. Thus, improvement of the obturator internus correlated with function of the levator ani. We therefore hypothesize that a loose pelvic floor could be improved by THA.
Pelvic floor muscle training
Pelvic floor muscle training (PFMT) is one of the most reliable exercises for improving UI [31]. Kim et al. [32] reported that 44.1 % of the patients achieved cure of urine leakage with 3 months of exercise. In addition, Bo et al. reported improvement with 6 months of PFMT [33] in 92 % of their patients.
THA is performed to improve hip-joint function and recovery of levator ani function that is connected to the obturator internus. In both PFMT and THA, neither the urethra nor bladder is surgically treated, but these procedures are thought to have an indirect effect on UI via pelvic floor muscles. In this study, 64 % of patients achieved cure of urine leakage after THA, even though the operation did not directly approach the urethra. This ratio is comparable with a few months of exercise.
Correlation between improvement of UI and hip function
ROM of the hip joint was significantly improved after THA; in particular, this improvement was significant in internal rotation. As mentioned above regarding morphology of the muscles surrounding the hip, the hip joint is connected to the pelvic floor muscles by the internal obturator muscle. We previously hypothesized a relationship between improvement of hip ROM and pelvic floor function [34]. In that study, we compared the improvement of ROM between patients who experienced improved UI (group A) and those who did not (group B). The scores for flexion, extension, and abduction were significantly improved in group A.
Owing to the THA, internal obturator muscle tension is recovered. The origins of both the levator ani muscle and endopelvic fascia are thought to shift cranially. This can explain the improvement of incontinence 3 days after the operation, even before recovery of muscular strength. In addition to attachment recovery, muscular strength is increased after 3 months of rehabilitation. This enhances the improvement of urinary UI.
Baba et al. [17] compared UI improvement between posterior and anterior approaches of THA. In the posterior approach, resection of the posterior structures, including the obturator internus tendon, is required. In contrast, in the anterior approach, damage to the muscle is reduced. In patients after the posterior approach, UI became worse, whereas in patients after the anterior approach, UI improved. This indicates the importance of muscles around the hip joint regarding UI.
Limitations
There were some limitations to this study. First, in the majority of the patients in Japan, secondary osteoarthritis is primarily due to congenital or acetabular dysplasia. This situation could be a reason for the difference in results compared with studies of other countries. Second, the long-term result remains unclear, because the follow-up period was only 3 months. Third, we did not compare anterior and posterior THA approaches. Finally, a point of this study was that the examination was performed by a urologist; however the urologist could only examine 83 of the total 1025 patients.
Conclusion
In this study, improved hip function contributed to the improvement of all types of UI. These results suggest a relationship between pelvic floor function and hip-joint function and thereby explain hip-dysfunction-related UI.
References
Irwin DE, Milsom I, Hunskaar S, Reilly K, Kopp Z, Herschorn S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50:1306–15. doi:10.1016/j.eururo.2006.09.019.
Coyne KS, Zhou Z, Thompson C, Versi E. The impact on health-related quality of life of stress, urge and mixed urinary incontinence. BJU Int. 2003;92:731–5. doi:10.1046/j.1464-410X.2003.04463.x.
Homma Y, Yamaguchi O, Imidafenacin Study Group. A randomized, double-blind, placebo- and propiverine-controlled trial of the novel antimuscarinic agent imidafenacin in Japanese patients with overactive bladder. Int J Urol. 2009;16:499–506. doi:10.1111/j.1442-2042.2009.02286.x.
Nakamura S, Ninomiya S, Nakamura T. Primary osteoarthritis of the hip joint in Japan. Clin Orthop Relat Res. 1989;24:190–6.
Yoshimura N, Campbell L, Hashimoto T, Okayasu T, Wilman C, Coggon D, et al. Acetabular dysplasia and hip osteoarthritis in Britain and Japan. Br J Rheumatol. 1998;37:1193–7.
Inoue K, Wicart P, Kawasaki T, Huang J, Ushiyama T, Hukuda S, et al. Prevalence of hip osteoarthritis and acetabular dysplasia in French and Japanese adults. Rheumatology. 2000;39:745–8.
Laupacis A, Bourne R, Rorabeck C, Feeny D, Wong C, Tugwell P, et al. The effect of elective total hip replacement on health-related quality of life. J Bone Joint Surg Am. 1993;75:1619–26.
Tamaki T, Oinuma K, Shiratsuchi H, Akita K, Iida S. Hip dysfunction-related urinary incontinence: A prospective analysis of 189 female patients undergoing total hip arthroplasty. Int J Urol. 2014;21:729–31. doi:10.1111/iju.12404.
Oinuma K, Eingartner C, Saito Y, Shiratsuchi H. Total hip arthroplasty by a minimally invasive, direct anterior approach. Oper Orthop Traumatol. 2007;19:310–26.
Homma Y, Yoshida M, Yamanishi T, et al. Core lower urinary tract symptom score (CLSS) questionnaire: A reliable tool in the overall assessment of lower urinary tract symptoms. Int J Urol. 2008;15:816–20.
Uebersax JS, Wyman JF, Shumaker SA, McClish DK, Fantl JA. Short forms to assess life quality and symptom distress for urinary incontinence in women: the Incontinence Impact Questionnaire and the Urogenital Distress Inventory. Continence Program for Women Research Group. Neurourol Urodyn. 1995;14:131–9.
Barry MJ, Fowler Jr FJ, O’Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992;148:1549–57. discussion 1564.
Okamura K, Nojiri Y, Osuga Y, Tange C. Psychometric analysis of international prostate symptom score for female lower urinary tract symptoms. Urology. 2009;73:1199–202. doi:10.1016/j.urology.2009.01.054.
Homma Y, Gotoh M. Symptom severity and patient perceptions in overactive bladder: how are they related? BJU Int. 2009;104:968–72. doi:10.1111/j.1464-410X.2009.08498.x.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes following total hip and knee arthroplasty in osteoarthritis. J Orthop Rheumatol. 1988;1:95–108.
Kikuchi A, Niu K, Ikeda Y, Hozawa A, Nakagawa H, Guo H, et al. Association between physical activity and urinary incontinence in a community-based elderly population aged 70 years and over. Eur Urol. 2007;52:868–74.
Baba T, Homma Y, Takazawa N, Kobayashi H, Matsumoto M, Aritomi K, et al. Is urinary incontinence the hidden secret complications after total hip arthroplasty? Eur J Orthop Surg Traumatol. 2014;24:1455–60. doi:10.1007/s00590-014-1413-4.
Homma Y, Yamaguchi O, Hayashi K; Neurogenic Bladder Society Committee. Epidemiologic survey of lower urinary tract symptoms in Japan. Urology. 2006;68:560–4.
Hannestad YS, Rortveit G, Sandvik H, Hunskaar S; Norwegian EPINCONT Study. A community-based epidemiological survey of female urinary incontinence: the Norwegian EPINCONT Study. Epidemiology of Incontinence in the County of Nord-Trøndelag J Clin Epidemiol. 2000;53:1150–7.
Aung HH, Sakamoto H, Akita K, Sato T. Anatomical study of the obturator internus, gemelli and quadratus femoris muscles with special reference to their innervation. Anat Rec. 2001;263:41–52.
Thompson P. On the arrangement of the fasciae of the pelvis and their relationship to the levator ani. J Anat Physiol. 1901;35:127–50.
Derry DE. Pelvic muscles and fasciae. J Anat Physiol. 1907;10:107–11.
Smith GE. Studies in the anatomy of the pelvis, with special reference to the fasciae and visceral supports. J Anat Physiol. 1908;42:198–218.
Smith WC. The levator ani muscle; its structure in man, and its comparative relationships. Anat Rec. 1923;26:175–203.
Courtney H. Anatomy of the pelvic diaphragm and anorectal musculature as related to sphincter preservation in anorectal surgery. Am J Surg. 1950;79:155–73.
Lawson JO. Pelvic Anatomy. I. Pelvic floor muscles. Ann R Coll Surg Engl. 1974;54:244–52.
Frohlich B, Hotzinger H, Fritsch H. Tomographical anatomy of the pelvis, pelvic floor, and related structures. Clin Anat. 1997;19:223–30.
Standring S. True pelvis, pelvic floor and perineum. In: Mundy AR (ed) Gray’s anatomy, 39th ed. Elsevier Churchill Livingstone, 2005. pp.1357–1371.
DeLancey JO. Structural support of the urethra as it relates to stress urinary incontinence: the hammock hypothesis. Am J Obstet Gynecol. 1994;170:1713–20. discussion 1720–1723.
Kim J, Betschart C, Ramanah R, Ashton-Miller JA, DeLancey JO. Anatomy of the pubovisceral muscle origin: Macroscopic and microscopic findings within the injury zone. Neurourol Urodyn. 2015;34:774–80. doi:10.1002/nau.22649.
Bø K, Herbert RD. There is not yet strong evidence that exercise regimens other than pelvic floor muscle training can reduce stress urinary incontinence in women: a systematic review. J Physiother. 2013;59:159–68. doi:10.1016/S1836-9553(13)70180-2.
Kim H, Yoshida H, Suzuki T. The effects of multidimensional exercise treatment on community-dwelling elderly Japanese women with stress, urge, and mixed urinary incontinence: a randomized controlled trial. Int J Nurs Stud. 2011;48:1165–72. doi:10.1016/j.ijnurstu.2011.02.016.
Bø K, Talseth T, Holme I. Single blind, randomised controlled trial of pelvic floor exercises, electrical stimulation, vaginal cones, and no treatment in management of genuine stress incontinence in women. BMJ. 1999;318(7182):487–93.
Sugano N, Noble PC, Kamaric E, Salama JK, Ochi T, Tullos HS. The morphology of the femur in developmental dysplasia of the hip. J Bone Joint Surg Br. 1998;80:711–9.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflicts of interest
None.
Additional information
This work has been presented at prior conferences The 38th Annual Meeting of International Urogynecological Association, Dublin, Ireland, 29 May 2013; and the 40th Annual Meeting of the Japanese Hip Society, Hiroshima, Japan, 30 November 2013
Rights and permissions
About this article

Cite this article
Okumura, K., Yamaguchi, K., Tamaki, T. et al. Prospective analyses of female urinary incontinence symptoms following total hip arthroplasty. Int Urogynecol J 28, 561–568 (2017). https://doi.org/10.1007/s00192-016-3138-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-016-3138-x