
Abstract
Purpose
The objective of this study was to determine the reasons for complaints and describe the judicial means upstream of France's courts following arthroscopy.
Methods
This is a retrospective observational study including all compensation records related to arthroscopic surgery, collected from the two leading French insurance organizations: MACSF and Branchet companies, from 2014 to 2018. Three medical experts performed the protocol and analysis.
Results
Finally, 247 procedures were included. The most common motives were: the appearance or persistence of pain (43.7%), postoperative infection (29.1%), technical errors (10.5%), nerve damage (5.7%), arterial lesions (2.8%), side errors (2.4%). Knee arthroscopies were more at risk of legal action for infection (p = 0.0006), and for disappointing results or persistent pain (p = 0.001). The first recourse was the conciliation and compensation commission (CCI) in 136 cases (55.1%), the civil court (TGI) in 88 cases (35.6%) and amicable settlement in 23 cases (9.3%). The mean time between surgery and the complaint was 32.8 ± 25.7 months, and was shorter in the case of an amicable procedure (p < 0.001). The lawsuit's mean duration was 15.6 ± 11.2 months, but longer in case of civil proceedings (p < 0.0001). The experts found no negligence in 81.8% of cases (n = 202). Infections were the leading cause of recourse to the conciliation and compensation commission (p < 0.0001), while technical errors were the main reason for complaints settled in an amicable procedure (p = 0.035). It was found more proven negligence in case of amicable procedures (p < 0.0001). The mean amount of compensation was 60,968.45€. No significant difference could be found regarding the median values of compensation between the reason of complaint. The amount of compensation was higher in civil court proceedings than in any others (p = 0.02).
Conclusion
The main reasons for arthroscopy litigation in France are reported in this study, specifying how they are managed upstream of possible legal proceedings. The knee is the main joint involved. Patient information, close follow-up associated with early and appropriate management of complications are the main ways to reduce complaints.
Level of evidence
IV.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The number of arthroscopic procedures is continually increasing. This increasing activity is concomitant with changes in the perception of the doctor–patient relationship. Society rejects the notion of risk and the occurrence of unsatisfactory results, which can result in patient mistrust of their surgeon [30, 31]. Very often banalized and considered by many patients as a minor surgical procedure (small scars, local anaesthesia, ambulatory stay…), arthroscopy is nonetheless a challenging procedure with a risk of complications [26]. Combined with the fact that most procedures are for functional reasons, this makes arthroscopy a particularly litigation-risk specialization [28].
Whatever the type of procedure, orthopaedic surgeons are particularly at risk of legal proceedings worldwide [17], as well as in France [23, 27]. Despite an overall increase in the number of proceedings, there was no impact on the number of complaints except those for non-specified dissatisfaction [22]. As a result of rapid technical advances [4], patients' demand for quality of information and functional outcomes increases significantly in Europe [12]. The main reasons for litigation reported in the literature concerning arthroscopy are infection, medical complications, lack of functional improvement or technical error [8, 20]. Recently, Pioger et al. [25] analyzed two French national databases and reported that the leading causes of lawsuits after arthroscopy in France were: infections (43%), musculoskeletal complications (25%) and lack of information (18%).
Nevertheless, online databases have only limited data (demographics, type of procedure performed, history…) [28], and have not proven to be exhaustive [25]. Moreover, these databases do not consider other recourse besides legal ones (insurance settlements, amicable recourse, conciliation procedures), which can provide an out-of-court solution in up to 90% of medical litigation cases [18].
The first objective was to evaluate the reasons for complaints following arthroscopy in France's private practice. The secondary objective was to determine whether there was a difference in the demographics and the motives for complaints between amicable recourse, conciliation procedures and civil legal court proceedings. The hypothesis was that the most often joint involved was the knee.
Materials and method
This study was registered in the National Committee of Computer Science and Liberties register (CNIL No. 2221312 version 0); data review was conducted following the 1964 Declaration of Helsinki and the Methodology's ethical standards of Reference MR-003 [24].
Study protocol and eligibility criteria
This retrospective observational study included all compensation records related to arthroscopic surgery, collected from the two leading French insurance organizations: MACSF (Mutuelle d'Assurances du Corps de Santé Français) and Branchet companies, from January 2014 to December 2018. The search for records in the insurers' databases was carried out using CCAM codes (Common Classification of Medical Acts). This corresponds to the official French nomenclature designed to identify the technical gestures practiced by doctors. Initially, two operators carried out an exhaustive collection, blind to each other, of CCAM codes relating to an arthroscopic procedure. All records reporting one of the selected CCAM codes related to arthroscopic procedures of the following joints were included: knee, shoulder, elbow, wrist, hip and ankle. Records involving open surgeries associated with the arthroscopy, not concluded as of January 1, 2019, or claims directed to another health care professional than an orthopaedic surgeon were excluded. Three medical legal experts performed the protocol and analysis of the results.
Data collection
Each file was taken from each insurance company's database by a medical expert, then anonymized before evaluation by a unique observer. According to a reading grid established in advance by three investigators, data collection followed a standardized collection protocol and was carried out between January 2019 and June 2019. Each file's data were classified into four categories: patient, surgeon, surgery, or complaint data. The patient's data were: date of birth, gender, profession, medical history, socio-economic level according to the ESeG (European Socio-economic Groups) nomenclature [10]. The data concerning the surgeon were: status, and type of practice (private or public). The surgery data were: joint, side, degree of urgency (scheduled or unscheduled surgery), particular context (professional disease or work accident), surgical indication. The data concerning the complaint were: the interval between surgery and complaint, type of complaint, reason, expert opinion, final decision, amount of indemnity and the total duration of the procedure.
Reason of claim and of legal procedure
In France, when a patient feels that he has been the victim of prejudice, there are several ways to claim compensation. The choice of reparation depends on the type and context of the injury. The patient can thus file a procedure before a conciliation and compensation commission (CCI), or otherwise before the administrative (public practice) or civil (private practice) courts. The CCI assesses whether the injury is related to a fault committed by the practitioner or the institution, or whether it is a therapeutic hazard. In the case of a proven fault, the practitioner's insurance company must offer compensation in proportion to the injury's severity. In the event of a therapeutic hazard, the patient may be covered by a specific public solidarity fund managed by the Office National d'Indemnisation des Accidents Medicaux (ONIAM). Finally, the patient may contact the surgeon directly to ask for amicable compensation for damages, without going through any organization.
Statistical analysis
Two-tailed Fisher’s exact test for categorical data was used to analyze the association between variables. The Kruskal–Wallis H test for independent groups was used to compare the samples' median values, and a Dunn’s multiple comparison test was performed by following. The alpha risk was set to 0.05. The number of necessary subjects was estimated under the assumption that the proportion of knee arthroscopy legal action would be 65% and 50% for the reference and study outcome, respectively. With a type 1 risk of 5% and a type 2 risk of 80%, a bilateral test and a dropout rate estimated at 10%, it was determined that 95 patients would be required for this study. Statistical analysis was performed with the online application EasyMedStat (version3.0.1).
Results
Case selection and claimant description
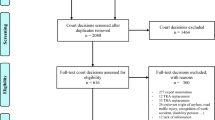
A total of 373 files were found in the databases by CCAM code search, 325 files at Branchet company and 48 at MACSF. Of these, 126 files (33.8%) were excluded, because they involved open surgery (Fig. 1). Of the 247 files included, there were 139 men (56.3%) for 108 women (43.7%). The majority had no previous medical history (n = 153, 61.9%). The most represented socio-economic class was class 4, including small entrepreneurs, shopkeepers, and artisans (n = 48, 19.4%). There were 45 work accidents (18.2%) and 5 professional diseases (2%). The demographic and professional data are summarized in Table 1.

Flowchart representing the data selection process
Surgical procedure description
Among the 247 cases, 237 surgeries were performed in private practice (96%) and 10 in hospitals (4%). Practitioners in public structures were involved if they had made an error that could engage their responsibility or perform a private activity. Eight were emergency procedures (3.2%), and 239 were scheduled surgeries (96.7%). Indications and joints included are summarized in Table 2.
Reason of claim description
There were multiple reasons for complaint in 74 cases (30%). The most common motives were: the appearance or persistence of pain (43.7%), and postoperative infection (29.1%). The reasons for negligence in performing the procedure were: technical errors (10.5%), nerve damage (5.7%), arterial lesions (2.8%), and side errors (2.4%). Nerve lesions were related to a tourniquet that was swollen too long or badly positioned in 71.4% of cases (10/14). Among the other etiologies identified, a lesion of the brachial plexus by stretching was found during shoulder arthroscopy. Of the seven vascular lesions, four were popliteal arteries, two subclavian arteries and one anterior tibial artery. All litigation cases are summarized in Fig. 2. The reasons for postoperative infections (n = 72) are more frequent after knee arthroscopy (n = 62) than another joint arthroscopy (n = 9 for shoulders, n = 1 for ankle and neither for elbow, wrist and hip) (p = 0.0006). There were more reasons for residual pain in the knees (n = 58/163, p = 0.001). There were no other significant differences in the distribution of different motives.

Distribution of reasons for complaint after arthroscopy according to the operated joint
Legal procedure description
The first recourse was the conciliation and compensation commission (CCI) in 136 cases (55.1%), the civil court (TGI) in 88 cases (35.6%) and amicable settlement in 23 cases (9.3%). The time between surgery and the complaint was 32.8 ± 25.7 months and was shorter in the case of an amicable procedure (16.8 ± 11.5 months; p < 0.001). The lawsuit's mean duration was 15.6 ± 11.2 months, but longer in case of civil proceedings (19.5 ± 10.1 months; p < 0.0001). The experts found no negligence by the surgeon involved in 81.8% of the cases (n = 202). At the end of the procedure, 81% of the surgeons or structures were dismissed (n = 200), and 15% were condemned (n = 37). In 4% of cases (n = 10), the final judgment was not available. In five cases of amicable settlement procedures (21.8%), no agreement was reached. In 46 conciliation and compensation commission cases (33.8%), no solution was found either by disagreement or because the court was not competent to make a decision. In 32.6% of these cases (n = 15/46), the plaintiff submitted a complaint to the civil court. Infections were the leading cause of recourse to the conciliation and compensation commission (p < 0.0001), while technical errors were the main reason for complaints settled in an amicable procedure (p = 0.035). The other causes of complaint were equally distributed among the three procedural types (Table 3). It was found more proven negligence in case of amicable procedures (p < 0.0001).
Indemnity payment
The mean amount of compensation was 60,968.45€ (range from 400 to 911,889.62). No significant difference could be found regarding the median values of compensation between the reason of complaint. The compensation was higher in the case of civil court proceedings than any others (p = 0.02).
Discussion
This study shows that the knee is the main joint involved in legal action after arthroscopy in France. The most common reasons for complaint are postoperative pain, infection, and then equally technical errors, stiffness or blockages, and poor doctor–patient relations (including lack of information and insufficient follow-up). It confirms the results of the literature on all these points [6, 25].
This large number of legal proceedings after knee arthroscopy should be moderated. It corresponds to the joint most frequently operated by arthroscopic surgery in France. It has been assessed that about 157,563 knee arthroscopies are performed per year in France [11], compared with other joints: 56,358 shoulders [16], 3030 wrists [16], 1211 ankles [16], and 528 hip arthroscopies [9]. Thus, it may be estimated that the annual rate of legal proceedings following knee and shoulder arthroscopies in France is 0.02%, compared with 0.05% for wrists, 0.08% for hips, and 0.1% for ankles.
This series mainly includes arthroscopic cases performed during a private activity. Only ten cases concern practitioners involved either through their private practice within the hospital or for a fault involving their responsibility. Pioger et al. [25] compared procedures in France after arthroscopy between public and private activities. The main complaints occurring in the public hospital were for infection (29.3%) and technical error (13.8%), as opposed to complaints related to the private activity being mainly infection (50%), and lack of information (24.6%). Our series confirms this large number of complaints about infection and lack of information in the context of private activity.
However, the persistence of pain (43.7%) was the leading cause of complaint in our series. An entity called musculoskeletal complications including stiffness, chronic pain, and unsatisfactory results, was reported by Pioger et al. with a rate of 25%, corresponding to their second cause of complaint [25]. If all these factors are added together in our series, a rate of 59% of the grounds for complaint is found, all joints combined. Those differences could be explained by the fact that Pioger et al. relied exclusively on national databases reporting data from administrative (public activity) and civil (private activity) courts [25]. In our series, 65.7% (71/108) of complaints about pain persistence were related to conciliation or amicable procedure, without recourse to a court procedure.
Infection is also a significant cause of complaints after arthroscopy, especially in the knee. It is the leading cause of arthroscopic complaints worldwide [6], as in France, with an estimated proportion of 43.3% (78/180) [25]. Despite being also one of the leading causes of arthroplasty litigation [3, 22, 27] or traumatology [3], Marmor et al. have shown a higher proportion of arthroscopy complaints than arthroplasty for this motive using the same protocol as ours [21]. Shah et al. reported a 15% lower rate in the United States [28]. This series estimates this number at 29.1% (72/247). A possible explanation for this result could be that two-thirds of conciliations are resolved at the end, and that only 1/3 of the remaining ones will lead to legal proceedings. This could lead to an over-representation of severe cases such as infections in civil courts. Whatever the difference in frequency, it is important to highlight two points. The first is the importance of adequately trained in diagnosing and managing acute infection when it occurs. In France, establishments are liable for damage resulting from infection, unless they can prove a therapeutic hazard. To meet this criterion, the absence of negligence in the prevention, early diagnosis, and appropriate management of the complication must be proved by the surgeon and the health care facilities. In our series, only three cases (4.2%) of infection were considered to be at fault during the conciliation procedure: a sterilization error, preoperative antibiotic therapy not noted in the surgical checklist and improper medical management. The other cases were transmitted either to the ONIAM in the case of a therapeutic hazard, or to the civil court when the conciliation authority would define itself as not competent. Based on the same database as ours, Senard et al. reported that up to 76% error in applying guidelines was found in prosthetic joint infections; 44% delay in diagnosis, 18% medical and antibiotic management error, and 13% surgical management mistake [27]. The second point is to properly inform the patients about this risk, which must be personalized according to their medical and surgical history and the type of surgery.
Information and the doctor–patient relationship is the leading cause of avoidable complaints [1, 2, 23]. In France, it can be found in up to 25% of litigation cases [23, 25]. In this series, a lower estimation of 7.7% of the cases is reported. It could be first explained by the inclusion of patients from the conciliation commission. Another possible explanation lies in the difference in the analysis period between our series and that of Pioger et al. and Mouton et al., respectively, over the period 1994–2020 [25], and 2000–2010 [23]. Since the law of March 4, 2002, in France [19], the practitioner must obtain the patient's free and informed consent for the acts performed and that he has the right to be informed about his state of health. Since this date, he must provide proof that the patient has been notified and understood the information. This is the main difficulty since the patient's attention decreases during the medical meeting when the practitioner mentions the risks of complications or failure [5]. The repeatability of consultations, the documentation provided, and traceability are the best evidence against possible negligence in patient information or follow-up [1, 2, 15]. These practices are now established in daily routine. However, at the time of these studies, this practice was not systematic and included cases in the early years following the application of this law. Therefore, our result could be encouraging and would show an improvement in practices on this subject, even if there is still improvement to be made.
On the other hand, the second avoidable cause of litigation, the wrong side, was found in a way comparable to that of Pioger et al. [25] but over a much shorter period in our series. In all cases, the surgeon entered the operating theatre with a patient who had already been draped by the paramedical teams, without checking his consultation report. All the patients who were victims of a side error had recourse to an amicable settlement.
In this study, the mean indemnity was 60,968.45€, similar to those reported in southern European countries in general orthopaedics [3] or arthroscopy [25, 29]. These amounts are nevertheless much lower than those received in Anglo–Saxon countries for litigation following arthroscopy [28] and also in joint replacement surgery [7, 22]. To our knowledge, there is no comparison in France between the compensation awarded after arthroscopic and open surgery. Concerning recent American data, the compensation awarded after arthroscopic surgery is generally lower than that for total joint arthroplasty (respectively $1,013,494 and $1,929,822) [7, 28].
Arthroscopic procedures are less at risk of condemnation (15%), in contrast, to open surgeries such as total joint replacement. Indeed, a 41.8% conviction rate after knee replacement surgery in France over an 8-year study period was reported by Gibon et al., using the same methodology as ours [13]. Our condemnation rate after litigation following arthroscopy is lower than that reported by Shah et al. in the United States (26%) [28], but especially compared to the estimation of Pioger et al. in France (67.8%) [25]. Ours is probably underestimated by the absence of inclusion of files containing appeal court records, representing 39.3% of civil court cases [25]. Nevertheless, the 67.8% assessment suggested by Pioger et al. [25] does not take into account the cases rejected (81%) during conciliation procedures. Indeed, only one out of three of the dismissed cases or not concluded will lead to legal proceedings in this series. Thus, cases arising in civil and administrative courts could be more severe and, therefore, more likely to result in a verdict against the surgeon or the health care institution.
However, several limitations may be reported. Its first limitation could be related to its retrospective character. Second, is the lack of inclusion of cases in administrative and civil courts of appeal. In our series, an appeal procedure corresponds to nearly one-third of the civil court's claims. In addition, although more information is provided by the insurance company files than the French anonymous databases, they cannot be considered exhaustive. This is because we could not gain access to the Société Hospitalière d'Assurance Mutuelle (SHAM), a leading insurance company for public hospitals and practitioners. Our study, therefore, allows us to highlight exclusively private activity. Thus, the public sector is particularly at risk of complications due to patients' more fragile conditions in one hand and arthroscopy's learning curve when it is performed by residents or young surgeons in training in the other hand [14, 26]. Finally, the 5-year duration of the study could be a limitation, whereas other studies cover more than 20 years [25]. Despite this point, we report the most extensive series of arthroscopy litigation in France. Another strength of our study is that it complements Pioger’s et al. [25] results by reporting the causes of litigation in France upstream of legal proceedings and their outcome.
This study describes the causes of complaints and the results of legal proceedings after arthroscopy in France. It confirms the importance of providing patients with precise and personalized information, while ensuring close postoperative monitoring to be able to manage any possible complications at an early stage. This information must be taken into account to reduce the number of complaints and complications considered as faulty.
Conclusion
The main reasons for litigation related to arthroscopy in France are reported in this study, specifying how they are managed upstream of possible legal proceedings. The knee is the main joint involved. Patient information, close follow-up associated with early and appropriate management of complications are the main ways to reduce the number of complaints.
References
Attarian DE, Vail TP (2005) Medicolegal aspects of hip and knee arthroplasty. Clin Orthop Relat Res 433:72–76
Adamson TE, Tschann JM, Gullion DS, Oppenberg AA (1989) Physician communication skills and malpractice claims. A complex relationship. West J Med 150:356–360
Agout C, Rosset P, Druon J, Brilhault J, Favard L (2018) Epidemiology of malpractice claims in the orthopedic and trauma surgery department of a French teaching hospital: a 10-year retrospective study. Orthop Traumatol Surg Res 104:11–15
Benson M, Boehler N, Szendroi M, Zagra L, Puget J (2014) Ethical standards for orthopaedic surgeons. Bone Jt J 96:1130–1132
Bhutta ZA (2004) Beyond informed consent. Bull World Health Organ 82:771–777
Bokshan SL, Ruttiman R, Eltorai AEM, DePasse JM, Daniels AH, Owens BD (2017) Factors associated with physician loss in anterior cruciate ligament reconstruction malpractice lawsuits. Orthop J Sports Med 5(11):2325967117738957
Bokshan SL, Ruttiman RJ, DePasse JM, Eltorai AEM, Rubin LE, Palumbo MA, Daniels AH (2017) Reported litigation associated with primary hip and knee arthroplasty. J Arthroplasty 32:3573-3577.e1
Cancienne JM, Brockmeier SF, Carson EW, Werner BC (2018) Risk factors for infection after shoulder arthroscopy in a large medicare population. Am J Sports Med 46:809–814
Disegni E, Martinot P, Dartus J, Migaud H, Putman S, May O, Girard J, Chazard E (2021) Hip arthroscopy in France: an epidemiological study of postoperative care and outcomes involving 3699 patients. Orthop Traumatol Surg Res 107(1):102767
European Socio economic Groups—Nomenclature socio-économique européenne—F2016/04-Insee http://www.insee.fr/fr/statistiques/2022135. 19 Feb 2016
Erivan R, Tardieu A, Villatte G, Ollivier M, Jacquet C, Descamps S, Boisgard S (2020) Knee surgery trends and projections in France from 2008 to 2070. Orthop Traumatol Surg Res 106(5):893–902
Ferrara SD, Baccino E, Bajanowski T, Boscolo-Berto R, Castellano M, De Angel R, Pauliukevičius A, Ricci P, Vanezis P, Vieira DN, Viel G, Villanueva E, EALM Working Group on Medical Malpractice (2013) Malpractice and medical liability. European Guidelines on Methods of Ascertainment and Criteria of Evaluation. Int J Legal Med 127:545–557
Gibon E, Farman T, Marmor S (2015) Knee arthroplasty and lawsuits: the experience in France. Knee Surg Sports Traumatol Arthrosc 23:3723–3728
Gil JA, Waryasz GR, Owens BD, Daniels AH (2016) Variability of arthroscopy case volume in orthopaedic surgery residency. Arthroscopy 32:892–897
Gould MT, Langworthy MJ, Santore R, Provencher MT (2003) An analysis of orthopaedic liability in the acute care setting. Clin Orthop Relat Res 407:59–66
HAS (Haute Autorité de Santé), Rapport sur la pertinence de l’arthroscopie dans les autres localisations www.has-sante.fr. 04 Jun 2014
Jena AB, Seabury S, Lakdawalla D, Chandra A (2011) Malpractice risk according to physician specialty. N Engl J Med 365:629–636
Kluge R, Koob R (2001) Expert assessment of medical malpractice. Orthopade 30:117–120
Loi no. 2002–303 du 4 mars 2002 relative aux droits des malades et à la qualité du système de santé—Légifrance (legifrance.gouv.fr)
Lubowitz JH, Brand JC, Rossi MJ (2018) Malpractice litigation after arthroscopy. Arthrosc J Arthrosc Relat Surg 34:2009
Marmor S, Farman T, Lortat-Jacob A (2009) Joint infection after knee arthroscopy: medicolegal aspects. Orthop Traumatol Surg Res 95:278–283
McWilliams AB, Douglas SL, Redmond AC, Grainger AJ, O’Connor PJ, Stewart TD, Stone MH (2013) Litigation after hip and knee replacement in the National Health Service. Bone Jt J 95B:122–126
Mouton J, Gauthé R, Ould-Slimane M, Bertiaux S, Putman S, Dujardin F (2018) Litigation in orthopedic surgery: what can we do to prevent it? Systematic analysis of 126 legal actions involving four university hospitals in France. Orthop Traumatol Surg Res 104:5–9
No authors listed. Loi no. 2002–303 du 4 mars 2002 relative aux droits des malades et à la qualité du système de santé. http://www.legifrance.gouv.fr. 01 Jul 2016
Pioger C, Jacquet C, Abitan A, Odri GA, Ollivier M, Sonnery-Cottet B, Boisrenoult P, Pujol N (2020) Litigation in arthroscopic surgery: a 20-year analysis of legal actions in France. Knee Surg Sports Traumatol Arthrosc. https://doi.org/10.1007/s00167-020-06182-3
Salzler MJ, Lin A, Miller CD, Herold S, Irrgang JJ, Harner CD (2014) Complications after arthroscopic knee surgery. Am J Sports Med 42:292–296
Senard O, Houselstein T, Crémieux AC (2019) Reasons for litigation in arthroplasty infections and lessons learned. J Bone Jt Surg Am 101:1806–1811
Shah KN, Eltorai AEM, Perera S, Durand WM, Shantharam G, Owens BD, Daniels AH (2018) Medical malpractice litigation following arthroscopic surgery. Arthroscopy 34:2236–2244
Tarantino U, Giai Via A, Macrì E, Eramo A, Marino V, Marsella LT (2013) Professional liability in orthopaedics and traumatology in Italy. Clin Orthop Relat Res 471:3349–3355
Truog RD (2012) Patients and doctors—evolution of a relationship. N Engl J Med 366(7):581–585
Tabibian BE, Kuhn EN, Davis MC, Pritchard PR (2017) Patient expectations and preferences in the spinal surgery clinic. World Neurosurg 106:595–601
Acknowledgements
The authors thank the attorney at law Anne-Elisabeth Leduc (Paris Bar) for her contribution.
Funding
No benefits in any form have been received or will be received related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Contributions
GR participated in the data interpretation, and article writing. TK participated in the study design and data acquisition. FZ and DO participated in the study design and article review. TL participated in data interpretation and article review. NC and FS participated in the study design, data acquisition and article review. Three authors (NC, FS, DO) reviewed the article with legal expert oversight. Each author has given final approval of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
GR, TK, FZ, NC, FS, TL and DO have nothing to disclose.
Ethical approval
No ethical approval was need for this study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Rougereau, G., Kavakelis, T., Sailhan, F. et al. Postoperative pain and infection are the most frequent reasons for legal action after knee arthroscopy: a 5-year review based on two private insurance French companies after arthroscopy. Knee Surg Sports Traumatol Arthrosc 29, 3551–3559 (2021). https://doi.org/10.1007/s00167-021-06586-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06586-9