
Abstract
This is a case report of a 26-year-old male who sustained a Segond fracture in the context of an acute anterior cruciate ligament (ACL) rupture incurred while downhill skiing. Further work-up revealed that the Segond fracture consisted of two distinct fragments with separate soft tissue attachments, including the capsule-osseous layer of the iliotibial band and the short arm of the biceps femoris. Imaging showed interval healing of the Segond fracture between initial presentation and the performance of arthroscopic ACL reconstruction approximately 4 months later. As intraoperative evaluation demonstrated that anatomic ACL reconstruction restored translational and rotatory knee stability, surgical repair of the Segond fracture, or the anterolateral complex of the knee more broadly, was not required. Maintenance of translational and rotatory knee stability was confirmed at serial post-operative appointments up through final follow-up.
Level of evidence Level V.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The Segond fracture has a lengthy history, first being described in 1879 by Dr. Paul Segond as a capsular avulsion injury following forced rotation of the knee [16]. In 1891 Mouret described the Segond fracture instead as an iliotibial band (ITB) injury following similar rotational maneuvers [15]. While the Segond fracture has long been recognized as pathognomonic of an anterior cruciate ligament (ACL) injury, its anatomy, as well as its functional and prognostic relevance, are topics of ongoing research and debate. With parallel interest in better elucidating the structure and function of the anterolateral complex (ALC) on the knee, several more recent studies have investigated the soft tissue attachments to the Segond fragment [10, 14, 17]. Recent studies investigating anterolateral injuries in the setting of ACL tears have reported rates of Segond fracture in up to 5% of cases [12]. In reviewing magnetic resonance imaging (MRI) of 146 knees with concomitant ACL tears and Segond fractures, Flores et al. found the bony fragment attached to the meniscotibial component of the mid-third lateral capsular ligament (mt-MTLCL, synonymous with anterolateral ligament, ALL) in 86 cases (58.9%), the posterior fibers of the ITB (pf-ITB) in 8 cases (5.5%), and both the mt-MTLCL and pf-ITB in 52 cases (35.6%) [6]. A study of 36 patients with combined ACL tear and Segond fracture found 34 of 36 cases (94.4%) in which the bony fragment was attached to both the anterolateral capsule and ITB [17]. More recently, Helito et al. studied MRIs of 48 patients with a combined ACL and Segond injury, finding that the bony fragment was attached to the ALL in all cases (100%) and to the ITB in 25 cases (52.1%), with concurrent ITB attachment corresponding to larger fragment size [10]. At present, the International Anterolateral Complex (ALC) Consensus Group concludes that, “A number of structures attach to the area of the Segond fracture including the capsule-osseous layer of the iliotibial band, the ALL and the anterior arm of the short head of biceps, and hence it is not clear which is responsible for this lesion” [8].
While anatomic studies have shown co-localization of the anterior arm of the short head of the biceps with the region of the proximal anterolateral tibia from which the Segond fragment most commonly derives, we are unaware of any clinical study demonstrating this soft tissue attachment to a bona fide Segond fragment. For instance, De Maeseneer et al. evaluated MRIs of 13 knees with concomitant ACL tears and Segond fractures finding the bony fragment attached to the ITB and ALL in 11 and 10 cases, respectively, but never attached to the anterior arm of the biceps tendon [13]. Furthermore, the Segond fracture has heretofore been most commonly reported as a single bony fragment to which one or several soft tissue structures attach. To our knowledge, this is the first description of a two-fragment Segond fracture with soft tissue attachments to the capsule-osseous layer of the ITB and the short head of the biceps femoris. Given the variation in reported Segond fracture anatomy, observing two separate bony fragments with unique soft tissue attachments in one patient highlights that there may not be one “correct” anatomic description, but rather the anatomy may depend on a variety of factors such as mechanism of injury, bony morphology, and anatomical variation, among others. Moreover, this demonstrates that both Segond and Mouret accurately described the soft tissue attachments of the Segond fracture over 100 years ago.
Case report
A 26-year-old male with no prior injury or surgical history sustained a non-contact twisting left knee injury while downhill skiing. The patient felt an initial pop when turning and attempted to squat to break his fall. With increasing knee flexion, he felt a distinct second painful pop on the outside of his left knee. At an outside emergency room, the knee was reported to be moderately swollen and painful to palpation over the medial and anterolateral joint line but had no evidence of unstable fracture. The patient was given a knee immobilizer and crutches and instructed to follow-up with an orthopaedist.
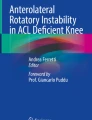
At presentation in the clinic two weeks later, further examination revealed range of motion from 20 to 80° (contralateral knee: -5° [hyperextension] to 148°), a Lachman test grade 2, Grade 2 + valgus laxity at 20° flexion, and an indeterminate pivot shift test due to guarding. KT-1000 arthrometer (Genourob, Laval, France) with 134 N (30 lbs) anterior tibia translational force revealed 4 mm side-to-side difference with guarding on the affected knee. Plain radiography revealed a Segond fracture (Fig. 1). MRI showed an ACL tear, Segond fracture, medial meniscus tear and grade 3 medial collateral ligament (MCL) injury (Fig. 2). Computed tomography (CT) and high-resolution ultrasound (US) further revealed that the Segond fracture consisted of two fragments (Fig. 3a, b). Using US to trace the soft tissue attachments proximally, the anterior fragment was found to be attached to the capsule-osseous layer of the ITB, while the posterior fragment was attached to the short head of the biceps femoris (Fig. 3c). Further assessment with CT 3D reconstruction showed that the anterior fragment measured 7.2 mm (anterior–posterior, AP) × 9.2 mm (proximal–distal, PD) and was 9.6 mm posterior to Gerdy’s tubercle, while the posterior fragment measured 15.3 mm (AP) × 4.8 mm (PD) and was 21.6 mm posterior to Gerdy’s tubercle (Figs. 3d, e).

Plain radiographs of left knee following acute injury. a AP, b lateral, and c sunrise views of left knee after acute ACL rupture, grade 3 MCL rupture, and medial meniscus tear. Yellow arrow highlights Segond fracture, pathognomonic for ACL rupture

MRI of left knee following acute injury. a Sagittal T2 fat-suppressed sequence demonstrating acute ACL rupture. b T2 fat-suppressed and c T1 MRI in coronal plane demonstrating Segond fracture, highlighted by yellow arrow. Increased signal intensity in proximal MCL and medial meniscus consistent with acute injury, better visualized in other sections (not included)

Segond fracture with two independent fragments. a Axial CT and b corresponding high-resolution US demonstrating two-fragment Segond fracture. c Dissection of fresh-frozen cadaveric specimen demonstrating corresponding anatomical structures including avulsion site (yellow arrow) of capsule-osseous layer (COL) of ITB (*) and avulsion site (blue arrow) of short arm of biceps femoris ( +). d, e CT 3D reconstruction of left knee demonstrating two independent fragments with corresponding soft tissue attachments (yellow arrow, COL of ITB; blue arrow, BF). BF biceps femoris, ITB iliotibial band, COL capsule-osseous layer of ITB
The patient opted to undergo 4 months of conservative treatment to finish an internship. Afterwards, repeat US demonstrated osseous integration of both fragments of the Segond fracture (Fig. 4a, b). The patient then elected to undergo arthroscopic anatomic ACL reconstruction after signing informed consent.

Healed Segond fracture and no anterolateral capsular damage 4 months after injury. a US of two-fragment Segond fracture acutely following injury, compared to b US of Segond fracture site 4 months following injury demonstrated interval healing (yellow arrows). c Intraoperative photograph of anterolateral capsule absent any hemorrhage/damage suggesting persistent capsular compromise. ANT anterior, BF biceps femoris, COL capsule-osseous layer of ITB, POST posterior
Examination under anesthesia revealed a grade 2 Lachman test, grade 2 pivot shift test, and 3–5 mm side-to-side difference in translation on anterior drawer. Varus and valgus stress tests at 0 and 20° knee flexion were stable, with resolution of previously noted valgus laxity. Arthroscopic examination showed no overt pathology of the anterolateral capsule (Fig. 4c), an intact anteromedial (AM) but incompetent posterolateral (PL) bundle of the ACL, and a longitudinal tear in the medial meniscus. The medial meniscal tear was repaired with a single all-inside suture. Anatomic PL bundle augmentation with a 9-mm quadriceps tendon autograft with a bone block was performed according to the anatomic ACL reconstruction scoring checklist [3]. The graft was fixed using an extra-cortical button (Endobutton, Smith & Nephew) on the femoral side and a PEEK interference screw (Biosure PK, Smith & Nephew) on the tibial side. Immediate post-operative examination revealed a grade 1 (normal) Lachman test and a negative pivot shift test.
The patient was discharged on the same day with a hinged knee brace locked in extension. One month post-operatively, quadriceps strength was diminished from baseline but improving. Full extension equal to the contralateral side was obtained at 2 months, at which time a negative pivot shift was also confirmed. Knee flexion equal to the contralateral side was achieved by 4 months. Post-operative follow-up was uncomplicated. The patient was most recently seen at 1 year and 10 months post-operative follow-up, at which time there was a grade 1 Lachman, negative pivot shift, 0 mm side-to-side difference in anterior tibial translation on KT-1000 measurement, and full and equal ROM compared to the contralateral knee.
Discussion
To our knowledge, this is the first description of a two-segment Segond fracture with distinct soft tissue attachments to the capsule-osseous layer of the ITB and the short head of the biceps femoris. While it has been recognized that multiple structures attach in the region of the Segond fracture, their respective involvement in the Segond fracture is uncertain [8, 15, 16]. Although several recent studies have reported combined attachment of the anterolateral capsule and ITB to the Segond fragment [1, 6, 10], clinical studies confirming attachment of the anterior arm of the biceps tendon have been largely absent [13]. The two-fragment Segond fracture in this case report supports the variability of soft tissues attached to the avulsed bone [1, 10, 13, 17]. The findings substantiate the fact that Segond fractures occur due to forces transmitted through multiple structures rather than the anterolateral ligament or anterolateral capsule alone. While Segond fractures with two fragments have been previously described [4, 9], these studies lacked the detailed imaging modalities utilized in this case report to clearly elucidate the identity of the soft tissue attachments.
It was beyond the scope of this case report to elucidate the mechanism of the Segond fracture, but it does offer a plausible hypothesis. The patient detailed in this case report described two distinct “popping” sensations. First was with mild knee flexion and presumed valgus, internal tibial rotation, and anterior tibial translation while skiing. The second was with additional knee flexion when trying to brace his fall. This mechanism closely mirrors a case report of an American football player who experienced sequential “popping” sensations with moderate then deep knee flexion, thereafter found to have concomitant ACL rupture and Segond fracture [1]. This “double injury” hypothesis has been further supported by two patients seen at our clinic who presented with isolated ACL ruptures, and then presented with additional Segond fractures after twisting injuries in deep flexion months later. While a cadaveric model in which a non-contact twisting mechanism reproducibly caused ACL rupture was recently described, Segond fractures have not yet been reproducibly replicated in vitro [2]. Nevertheless, a comprehensive pictorial and video essay of an anterolateral knee dissection showed that maximal tension of the combined Segond fracture soft tissue attachments occurred with deeper (~ 90º) knee flexion and internal tibia rotation, supporting the plausibility of the proposed injury mechanism (Fig. 5) [11].

Schematic of the proposed mechanism of ACL rupture and Segond fracture. a Beginning with the knee in anatomic alignment near full extension, b the ACL most commonly ruptures with approximately 20–30º knee flexion with combined anterior tibial translation (ATT), internal tibia rotation (IR), and valgus stress. c The Segond fragment is proposed to fracture with further knee flexion and internal tibia rotation. ITB iliotibial band, TT tibial tubercle, ATT anterior tibial translation, IR internal tibial rotation
Regarding the Segond fracture’s role in knee stability, Melugin et al. compared patients with isolated ACL tears to those with combined Segond fractures and ACL tears and found that those with a combined injury had significantly more pre-operative instability [14]. However, other studies have not found a Segond fracture to predict a higher grade of pivot shift, Lachman test, or anterior drawer when compared to an isolated ACL tear [5, 7, 19]. Investigations of the clinical outcomes following Segond fracture, which may influence the consideration for operative treatment, have found similar rates of graft failure, residual pivot shift, and activity levels when comparing patients who underwent ACL reconstruction with or without concomitant Segond fracture [14, 18, 19]. In the present case report, the patient demonstrated interval healing of the Segond fracture at 4 months, and individualized, anatomic ACL reconstruction without lateral augmentation was sufficient to restore knee stability. Taken together, these findings suggest that additional treatment of a Segond fracture may be unnecessary, although prospective randomized control trials to more definitively address this have not yet been performed.
Conclusion
This case report demonstrates that forces transmitted simultaneously through the capsule-osseous layer of the ITB and the short head of the biceps femoris are sufficient to produce a two-fragment Segond fracture, which may occur sequentially following ACL rupture. Both historical descriptions by Segond and Mouret may have, therefore, been accurate. While potential mechanisms of such injuries warrant further study, rotatory knee stability is multifactorial and many Segond fractures may be managed with conservative treatment.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- ALL:
-
Anterolateral ligament
- CT:
-
Computed tomography
- ITB:
-
Iliotibial band
- MCL:
-
Medial collateral ligament
- MRI:
-
Magnetic resonance imaging
- Mt-LCL:
-
Mid-third lateral capsular ligament
- US:
-
Ultrasound
References
Albers M, Shaikh H, Herbst E, Onishi K, Nagai K, Musahl V, Fu FH (2018) The iliotibial band and anterolateral capsule have a combined attachment to the Segond fracture. Knee Surg Sports Traumatol Arthrosc 26:1305–1310
Bates NA, Schilaty ND, Nagelli CV, Krych AJ, Hewett TE (2018) Validation of noncontact anterior cruciate ligament tears produced by a mechanical impact simulator against the clinical presentation of injury. Am J Sports Med 46(9):2113–2121
Diermeier T, Rothrauff BB, Engebretsen L, Lynch AD, Ayeni OR, Paterno MV et al, The Panther Symposium ACL Treatment Consensus Group (2020) Treatment after anterior cruciate ligament injury: Panther symposium ACL treatment consensus group. Knee Surg Sports Traumatol Arthrosc 28(8):2390–2402
Dietz GW, Wilcox DM, Montgomery JB (1986) Segond tibial condyle fracture: lateral capsular ligament avulsion. Radiology 159:467–469
Ferretti A, Monaco E, Fabbri M, Maestri B, De Carli A (2017) Prevalence and classification of injuries of anterolateral complex in acute anterior cruciate ligament tears. Arthroscopy 33:147–154
Flores DV, Smitaman E, Huang BK, Resnick DL (2016) Segond fracture: an MR evaluation of 146 patients with emphasis on the avulsed bone fragment and what attaches to it. Skeletal Radiol 45:1635–1647
Gaunder CL, Bastrom T, Pennock AT (2017) Segond fractures are not a risk factor for anterior cruciate ligament reconstruction failure. Am J Sports Med 45(14):3210–3215
Getgood A, Brown C, Lording T, Amis A, Claes S, Geeslin A, Musahl V, ALC Consensus Group (2019) The anterolateral complex of the knee: results from the International ALC Consensus Group Meeting. Knee Surg Sports Traumatol Arthrosc 27:166–176
Goldman AB, Pavlov H, Rubenstein D (1988) The Segond fracture of the proximal tibia: a small avulsion that reflects major ligamentous damage. Am J Roentgenol 151:1163–1167
Helito PVP, Bartholomeeusen S, Claes S, Bordalo-Rodrigues M, Helito CP (2020) Magnetic resonance imaging evaluation of the anterolateral ligament and the iliotibial band in acute anterior cruciate ligament injuries associated with Segond fractures. Arthroscopy 36(6):1679–1686
Herbst E, Albers M, Burnham JM, Fu FH, Musahl V (2017) The anterolateral complex of the knee. Orthop J Sport Med. https://doi.org/10.1177/2325967117730805
Lee DW, Lee JH, Kim JN, Moon SG, Kim NR, Kim DH, Kim JG (2018) Evaluation of anterolateral ligament injuries and concomitant lesions on magnetic resonance imaging after acute anterior cruciate ligament rupture. Arthroscopy 34(8):2398–2406
De Maeseneer M, Boulet C, Willekens I, Lenchik L, De Mey J, Cattrysse E, Shahabpour M (2015) Segond fracture: involvement of the iliotibial band, anterolateral ligament, and anterior arm of the biceps femoris in knee trauma. Skeletal Radiol 44:413–421
Melugin HP, Johnson NR, Wu IT, Levy BA, Stuart MJ, Krych AJ (2018) Is treatment of Segond fracture necessary with combined anterior cruciate ligament reconstruction? Am J Sports Med 46:832–838
Mouret J (1892) Considérations sur l’anatomie du genou et étude des luxations des cartilages semi-lunaires. Coulet, Montpellier
Segond P (1879) Recherches cliniques et expérimentales sur les épanchements sanguins du genou par entorse. Progres Med 7:297–299, 319–321, 340–341
Shaikh H, Herbst E, Rahnemai-Azar AA, Bottene Villa Albers M, Naendrup J-H, Musahl V, Irrgang JJ, Fu FH (2017) The Segond fracture is an avulsion of the anterolateral complex. Am J Sports Med 45:2247–2252
Slagstad I, Parkar AP, Strand T, Inderhaug E (2020) Incidence and prognostic significance of the segond fracture in patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med 48(5):1063–1068
Yoon KH, Kim JS, Park SY, Park SE (2018) The influence of Segond fracture on outcomes after anterior cruciate ligament reconstruction. Arthroscopy 34:1900–1906
Funding
No funding was utilized for this study.
Author information
Authors and Affiliations
Contributions
KB, BR, and KN were involved with drafting and revising the manuscript, as well as creation of the figures. KN assisted with creation of the 3D-CT model. KO acquired the ultrasound images. KO and FF were involved with design, clinical analysis, and revision of the manuscript. FF was involved in the surgical management of the patient. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no conflicts of interest.
Ethical approval
The study was approved by the Institutional Review Board at the University of Pittsburgh (STUDY1903019).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Byrne, K.J., Rothrauff, B.B., Nagai, K. et al. Two-fragment Segond fracture validates historical descriptions of independent soft tissue attachments. Knee Surg Sports Traumatol Arthrosc 30, 71–77 (2022). https://doi.org/10.1007/s00167-021-06515-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06515-w