
Abstract
Purpose
To evaluate the relationship between posterior tibial slope (PTS), posterior condylar offset (PCO), femoral sagittal angle (FSA) on clinical outcomes, and propose optimal sagittal plane alignments for unicompartmental knee arthroplasty (UKA).
Methods
Prospectively collected data of 265 medial UKA was analysed. PTS, PCO, FSA were measured on preoperative and postoperative lateral radiographs. Clinical assessment was done at 6-month, 2-year and 10-year using Oxford Knee Score, Knee Society Knee and Function scores, Short Form-36, range of motion (ROM), fulfilment of satisfaction and expectations. Implant survivorship was noted at mean 15-year. Kendall rank correlation test evaluated correlations of sagittal parameters against clinical outcomes. Multivariable linear regression evaluated predictors of postoperative ROM. Effect plots and interaction plots were used to identify angles with the best outcomes. (p < 0.05) was the threshold for statistical significance.
Results
There were significant correlations between PTS, PCO and FSA. Younger age, lower BMI, implant type, greater preoperative flexion, steeper PTS and preservation of PCO were significant predictors of greater postoperative flexion. There were significant interaction effects between PTS and PCO. Effect plots demonstrate a PTS between 2° to 8° and restoration of PCO within 1.5 mm of native values are optimal for better postoperative flexion. Interaction plot reveals that it is preferable to reduce PCO by 1.0 mm when PTS is 2° and restore PCO at 0 mm when PTS is 8°.
Conclusion
UKA surgeons and future studies should be mindful of the relationship between PTS, PCO and FSA, and avoid considering them in isolation. When deciding on the method of balancing component gaps in UKA, surgeons should rely on the PTS. Decrease the posterior condylar cut when PTS is steep, and increase the posterior condylar cut when PTS is shallow. The acceptable range for PTS is between 2° to 8° and PCO should be restored to 1.5 mm of native values.
Level of evidence
II.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Postoperative range of motion (ROM) is an important outcome parameter following knee arthroplasty [22, 28, 42]. This is especially so for Asian populations, that tend to require deep knee flexion in their daily activities, such as kneeling during prayers [22, 29].
Posterior tibial slope (PTS), posterior condylar offset (PCO) and femoral sagittal angle (FSA) are surgically modifiable determinants of postoperative ROM after unicompartmental knee arthroplasty (UKA) [8, 9, 11, 32]. A steeper PTS can facilitate greater flexion [16] but could result in tighter extension gaps [40]. Greater flexion in FSA can also facilitate greater knee flexion [8], but increases contact stress in the unreplaced compartment [32]. Component positioning in the sagittal plane is vital to prevent early failure in UKA [2, 32].
However, the optimal sagittal positioning remains controversial, partly because previous studies have evaluated PTS, PCO and FSA in isolation [8, 16, 32, 40]. This study aimed to propose the optimal alignment for sagittal plane parameters in UKA by accounting for PTS, PCO and FSA alignments concurrently. We hypothesize that there is an optimal range for sagittal plane parameters that can maximize postoperative ROM.
Methods and materials
Patients
This study was approved by a Centralized Institutional Review Board (CIRB 2020/2157) and performed in accordance to the amended ethical standards laid out in the World Medical Association Declaration of Helsinki [47]. Prospectively collected data of patients who underwent primary fixed-bearing UKA at a single institution from 2004 to 2007 was reviewed. A total of 392 UKAs were performed during this period. After excluding those whose radiographs went missing when patient records went digital and PROMs of less than 2-year follow-up, 265 UKAs with complete follow up from pre operation to 10-year were available for analysis (68%). The 265 UKAs belonged to 213 patients. 52 patients had bilateral UKAs, while 161 patients had unilateral UKAs. The mean age of patients was 61.0 ± 7.6 years old, mean body mass index was 27.2 ± 4.4 kg/m2, and 75% were females (Table 1). On latest review at mean 15-years, 19 knees have been revised. Reasons for revision included: aseptic loosening of tibial component (n = 1), progression of OA (n = 13), polyethylene failure (n = 3), subsidence of tibial tray (n = 2). Two types of implants were used in this study, the Preservation (DePuy Synthes, Leeds, UK) (n = 59) and the Miller-Galante (Zimmer Biomet, Warsaw, IN) (n = 206) UKAs. Both prostheses had a similar round-on-flat geometry. Failure rates by implants were at 8% for the Preservation (n = 5/59) and 7% for the Miller-Galante (n = 14/206). Only a minority of revisions occurred before the 10-year mark (n = 4), giving an overall 10-year survivorship of 98%. The final survivorship of mean 15-year (range 13–17 years) was 93%.
Surgical technique
All UKAs were consecutively done by the two senior authors who are fellowship-trained arthroplasty surgeons. The indication for surgery was based on the Kozinn and Scott criteria [20] and all surgeries were indicated for unicompartmental noninflammatory primary OA of the knee with intact cruciate ligaments. The surgical technique was performed in accordance with the respective manufacturer’s surgical instrumentation guide using conventional instruments. An abbreviated medial approach without patellar eversion was performed.
Clinical evaluation
The patients included in this study had few medical comorbidities at index operation, which was translated into the Charlson Comorbidity Index (CCI) scores [34] (Table 1). A variety of patient-reported outcome measures (PROMs) were used to assess all patients routinely in the clinic at 6-month, 2-year and 10-year follow-up. Knee function was assessed using the: adapted Oxford Knee Score (OKS) scoring system [30]; Knee Society knee (KSKS) and function (KSFS) scores [15], Short Form-36 (SF-36) [17, 23] health survey which was transformed into physical (PCS) and mental (MCS) component scores [43] (Table 2). Fulfilment of patients’ expectations and satisfaction after surgery was done with a 6-point scale using similar questions to Bourne et al. [6]. ROM was assessed using a two-arm goniometer with the patient in a supine position. All clinical assessment was performed by physiotherapists who were not involved in this study. The electronic records of all patients were reviewed in July 2020 to determine if and when they had undergone revision, giving a mean duration of follow-up of 15 years.
Radiological evaluation
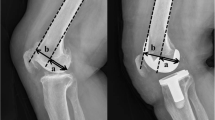
Preoperative and postoperative lateral radiograph of all 265 knee joints were used for radiological evaluation. Radiographs measurements were performed using the Picture Archiving and Communication Systems (PACS: Carestream Health, Rochester, New York, USA). Measurements were recorded to a precision of 0.1 mm and 1°. Measurements were performed using a similar method to previous authors [12, 18, 40], where PTS is the acute angle between the tibial plateau in the sagittal view, and the line perpendicular to the tibial mechanical axis (Figs. 1and 2); PCO is the perpendicular distance of the posterior-most aspect of the femoral condyle from a projection of the posterior femoral line (Figs. 1and 2); FSA is the acute angle between the cut surface of the posterior femoral condyle and the anatomical axis of the femur (Fig. 3a, b).

Preoperative lateral radiograph showing measurement of posterior condylar offset (PCO) and posterior tibial slope (PTS)

Postoperative lateral radiograph showing measurements of posterior condylar offset (PCO) and posterior tibial slope (PTS)

Postoperative lateral radiograph showing the measurement of the femoral sagittal angle (FSA) on a Preservation and b Miller-Galante implants
Radiographs were evaluated consecutively by two blinded independent assessors who were not involved in the surgical procedure. Evaluation was performed by both assessors independently, in December 2019. Subsequently, the evaluation was repeated by both assessors after 6 months. The test–retest reliability was assessed using intraclass correlation coefficient (ICC). Using a two-way random-effects model, the ICC value was 0.98 (95% CI 0.97–0.99, p < 0.05). An ICC > 0.9 represents excellent reliability, which suggests that measurement of sagittal plane parameters meticulously performed using this method, can achieve excellent reliability and reproducibility.
Statistical analysis
All statistical analysis was done using RStudio (RStudio: Integrated Development for R. Rstudio, Inc., Boston, MA). A p value of < 0.05 was used as the threshold for statistical significance. Sample size calculation was performed with power at 0.8 and a significance level at 0.05. To detect 1º of change, with a standard deviation of 3º, the minimum sample size was 142. Descriptive statistics included count, mean, standard deviation and proportions. Kendall’s ranked correlation test was used to evaluate the correlation between sagittal plane parameters with various clinical outcomes. Multivariable regression analysis was performed to elucidate the significant predictors of postoperative ROM. Multivariable regression models also explored potential interaction effects between PTS, PCO and FSA. Regression models adjusted for potential confounders of outcomes, such as age [21], body mass index (BMI) [5, 13, 25, 35, 48], CCI, operated side, different implant designs, coronal and limb alignments, and preoperative ROM [16]. Subsequently, adjusted outputs from the multivariable regression models were channelled into constructing effect plots and interaction plots, to isolate the individual effect of variables on postoperative ROM and propose recommendations accordingly. Loess lines, which are locally weighted smooth polynomial regression lines set to a default span of 0.5, were utilised to better capture non-linear trends in the data and reduce any skewing effect from outliers.
Results
Correlations
PTS, PCO and FSA are significantly correlated with each other (Table 3). A steeper PTS and larger PCO was correlated with greater flexion. Greater flexion of the FSA was correlated with greater FFD. A larger PCO and greater flexion of the FSA was correlated with better PROMs (Table 3).
Predictors
There were significant two-way interaction effects between PTS and PCO (Table 4). Younger age, lower BMI and greater preoperative flexion are significant predictors of better postoperative flexion (Tables 4, 5and 6). The only significant predictor of FFD was preoperative FFD (Tables 4, 5and 6).
Sagittal plane alignment
A PTS between 2° to 8° is optimal for better postoperative flexion (Fig. 4). Restoration of PCO within 1.5 mm from preoperative values is optimal for better postoperative flexion (Fig. 5). At shallow PTS of 2°, it is preferable to reduce PCO by 1.0 mm, whereas at steeper PTS of 8°, it is preferable to restore PCO at 0 mm (Fig. 6).

Effect plot showing the adjusted influence of posterior tibial slope (PTS) on knee flexion at 6-month

Effect plot showing the adjusted influence of change in posterior condylar offset (∆PCO) on knee flexion at 6-month

Interaction plot showing the effect of posterior tibial slope (PTS) on knee flexion at 6-month, for different values of change in posterior condylar offset (∆PCO)
Discussion
The first important finding of this study was the interaction effect between PTS and PCO. This interaction means that there are differential effects of PTS depending on different sizes of PCO, and vice versa. This finding was consistent with a previous study by Han et al. which found an interaction effect between PTS and PCO in total knee arthroplasty (TKA) [12]. Even though knee kinematics between UKA and TKA differ significantly, this finding seems to be similar for both. This is crucial because surgeons need to balance the component gaps yet be mindful that the resultant size of the posterior condyle on different tibial plateau inclination may influence the femoral roll-back mechanism [46]. A mismatch between the PTS and PCO may lead to excessive translation during weight-bearing activities [14, 46], and exacerbate stress on the native knee structures [37, 38].
The second important finding of this study was that PTS between 2° to 8° is optimal in maximising knee flexion. This finding was consistent with previous studies that have made similar recommendations [1, 37, 39]. In addition, the study by Small et al. demonstrated that contact strain in the posterior compartment increased by 80% (p = 0.00) when PTS was increased from 5° to 10°, suggesting that 10° PTS is not advisable [38]. The study by Weber et al. in a cohort of fixed-bearing UKA, also found that there was a significant reduction in wear rate from 10.4 mg/million cycles to 3.22 mg/million cycles when PTS was increased from 0° to 8° [45]. These findings are consistent with the recommendation regarding optimal PTS angles within 2°–8°.
The third important finding of this study was that restoration of PCO to within 1.5 mm of its preoperative value was ideal in maximising knee flexion. Restoration of PCO has been described to be an important predictor of better functional outcomes after TKA [27], but this has not yet been described in UKA. Restoration of PCO is likely to be crucial due to two reasons. Firstly, UKA may be primarily thought of as a resurfacing procedure [3, 44], restoration of PCO is more likely to maintain the complex kinematics of the native knee. Secondly, given the interactive effects between PTS and PCO detailed above, preserving the patient’s native PCO will likely avoid unnecessary counter-productive effects when coupled with PTS. Surgeons just have to be mindful not to cut PCO > 1.5 mm when balancing the component gaps.
In terms of survivorship, PTS, PCO and FSA were not associated with failures in this study. This finding was consistent with previous studies [7, 10], although some authors have reported PTS to be a crucial factor in UKA survivorship [26, 33]. The mechanism for this is because extremes of PTS has been shown to be a risk factor for bearing dislocation [36], although this is still contested [19, 24]. However, this study is unable to corroborate if a steeper PTS might predispose patients to a higher risk of bearing dislocation as it did not include any mobile-bearing UKA. Park et al. also described that excessive flexion of FSA may contribute to the progression of lateral compartment OA due to higher contact stresses [32]. However, none of the patients with revision for the progression of OA in this study had extreme FSA positioning, which suggests that it may not be a clinically significant mechanism for failure.
Given that there has been significant improvement in implant design since 2007, the effects of these parameters may be different with newer generations of UKA implants that have a different geometry and hence biomechanics. A limitation of this study was the use of short radiographs for radiological evaluation, which has slightly lesser precision compared to long film radiographs. Although short radiographs have been described to be an acceptable alternative to long film radiographs in assessing component positioning [41]. Another limitation was the use of 2-dimensional films, therefore tilt, rotation or non-strict lateral views could influence radiological measurements. It would be useful for future studies with access to 3-dimensional imaging to corroborate the findings from this study. Despite this limitation, this study has various strengths. Firstly, it has a long duration of follow-up. Secondly, this study utilized a myriad of different yardsticks and survivorship in assessing patients. Thirdly, this study used a string of rigorous statistical approaches that adjusted for various covariates and interactions, to accurately capture the effect of each factor free from the influence of other confounders.
Clinically, UKA surgeons should aim to cut PTS between 2° to 8° and restore PCO to within 1.5 mm of its preoperative value. Since PTS is often augmented depending on the condition of the cruciate ligaments, surgeons should prioritize increasing the posterior condylar cut when PTS is shallow, and decrease the posterior condylar cut when PTS is steep. Moreover, these targets would be useful to guide planning in robotic surgery given the extremely precise cuts involved [4, 31].
Conclusion
UKA surgeons and future studies should be mindful of the relationship between PTS, PCO and FSA, and avoid considering them in isolation. When deciding on the method of balancing component gaps in UKA, surgeons should rely on the PTS. Decrease the posterior condylar cut when PTS is steep, and increase the posterior condylar cut when PTS is shallow. The acceptable range for PTS is between 2° to 8° and PCO should be restored to 1.5 mm of native values.
References
Adulkasem N, Rojanasthien S, Siripocaratana N, Limmahakhun S (2019) Posterior tibial slope modification in osteoarthritis knees with different ACL conditions: cadaveric study of fixed-bearing UKA. J Orthop Surg (Hong Kong) 27:2309499019836286
Aleto TJ, Berend ME, Ritter MA, Faris PM, Meneghini RM (2008) Early failure of unicompartmental knee arthroplasty leading to revision. J Arthroplasty 23:159–163
Andriacchi TP, Galante JO, Fermier RW (1982) The influence of total knee-replacement design on walking and stair-climbing. J Bone Joint Surg Am 64:1328–1335
Bell SW, Anthony I, Jones B, MacLean A, Rowe P, Blyth M (2016) Improved accuracy of component positioning with robotic-assisted unicompartmental knee arthroplasty: data from a prospective, randomized controlled study. J Bone Joint Surg Am 98:627–635
Berend KR, Lombardi AV Jr, Mallory TH, Adams JB, Groseth KL (2005) Early failure of minimally invasive unicompartmental knee arthroplasty is associated with obesity. Clin Orthop Relat Res 440:60–66
Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KD (2010) Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res 468:57–63
Bruni D, Gagliardi M, Akkawi I, Raspugli GF, Bignozzi S, Marko T et al (2016) Good survivorship of all-polyethylene tibial component UKA at long-term follow-up. Knee Surg Sports Traumatol Arthrosc 24:182–187
Cho KY, Kim KI, Song SJ, Kim KJ (2018) Intentionally increased flexion angle of the femoral component in mobile bearing unicompartmental knee arthroplasty. Knee Surg Relat Res 30:23–27
Cinotti G, Sessa P, Ripani FR, Postacchini R, Masciangelo R, Giannicola G (2012) Correlation between posterior offset of femoral condyles and sagittal slope of the tibial plateau. J Anat 221:452–458
Flury A, Hasler J, Dimitriou D, Antoniadis A, Finsterwald M, Helmy N (2019) Midterm clinical and radiographic outcomes of 115 consecutive patient-specific unicompartmental knee arthroplasties. Knee 26:889–896
Gaudiani MA, Nwachukwu BU, Baviskar JV, Sharma M, Ranawat AS (2017) Optimization of sagittal and coronal planes with robotic-assisted unicompartmental knee arthroplasty. Knee 24:837–843
Han HS, Kang SB (2018) Interactive effect of femoral posterior condylar offset and tibial posterior slope on knee flexion in posterior cruciate ligament-substituting total knee arthroplasty. Knee 25:335–340
Harbourne AD, Sanchez-Santos MT, Arden NK, Filbay SR (2019) Predictors of return to desired activity 12 months following unicompartmental and total knee arthroplasty. Acta Orthop 90:74–80
Horsager K, Kaptein BL, Rømer L, Jørgensen PB, Stilling M (2017) Dynamic RSA for the evaluation of inducible micromotion of Oxford UKA during step-up and step-down motion. Acta Orthop 88:275–281
Insall JN, Dorr LD, Scott RD, Scott WN (1989) Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res 248:13–14
Inui H, Taketomi S, Yamagami R, Kawaguchi K, Nakazato K, Tanaka S (2020) Necessary factors to achieve deep flexion for Asian populations after Oxford unicompartmental knee arthroplasty. J Knee Surg 33:294–300
Jiang L, Chen JY, Chong HC, Chia SL, Lo NN, Yeo SJ (2016) Early outcomes of unicompartmental knee arthroplasty in patients with preoperative genu recurvatum of non-neurological origin. J Arthroplasty 31:1204–1207
Kaya Bicer E, Servien E, Lustig S, Demey G, Ait Si Selmi T, Neyret P (2010) Sagittal flexion angle of the femoral component in unicompartmental knee arthroplasty: is it same for both medial and lateral UKAs? Knee Surg Sports Traumatol Arthrosc 18:928–933
Kazarian GS, Barrack TN, Okafor L, Barrack RL, Nunley RM, Lawrie CM (2020) High prevalence of radiographic outliers and revisions with unicompartmental knee arthroplasty. J Bone Joint Surg Am 102:1151–1159
Kozinn SC, Scott R (1989) Unicondylar knee arthroplasty. J Bone Joint Surg Am 71:145–150
Kuipers BM, Kollen BJ, Bots PC, Burger BJ, van Raay JJ, Tulp NJ et al (2010) Factors associated with reduced early survival in the Oxford phase III medial unicompartment knee replacement. Knee 17:48–52
Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T (2002) Maximizing flexion after total knee arthroplasty: the need and the pitfalls. J Arthroplasty 17:59–62
Lee M, Huang Y, Chong HC, Ning Y, Lo NN, Yeo SJ (2016) Predicting satisfaction for unicompartmental knee arthroplasty patients in an Asian population. J Arthroplasty 31:1706–1710
Lee SY, Bae JH, Kim JG, Jang KM, Shon WY, Kim KW et al (2014) The influence of surgical factors on dislocation of the meniscal bearing after Oxford medial unicompartmental knee replacement: a case-control study. Bone Joint J 96 b:914–922
Liow MH, Goh GS, Tay DK, Chia SL, Lo NN, Yeo SJ (2016) Obesity and the absence of trochlear dysplasia increase the risk of revision in patellofemoral arthroplasty. Knee 23:331–337
Lo Presti M, Raspugli GF, Reale D, Iacono F, Zaffagnini S, Filardo G et al (2019) Early failure in medial unicondylar arthroplasty: radiographic analysis on the importance of joint line restoration. J Knee Surg 32:860–865
Malviya A, Lingard EA, Weir DJ, Deehan DJ (2009) Predicting range of movement after knee replacement: the importance of posterior condylar offset and tibial slope. Knee Surg Sports Traumatol Arthrosc 17:491–498
Miner AL, Lingard EA, Wright EA, Sledge CB, Katz JN (2003) Knee range of motion after total knee arthroplasty: how important is this as an outcome measure? J Arthroplasty 18:286–294
Mulholland SJ, Wyss UP (2001) Activities of daily living in non-Western cultures: range of motion requirements for hip and knee joint implants. Int J Rehabil Res 24:191–198
Murray DW, Fitzpatrick R, Rogers K, Pandit H, Beard DJ, Carr AJ et al (2007) The use of the Oxford hip and knee scores. J Bone Joint Surg Br 89:1010–1014
Park KK, Han CD, Yang IH, Lee WS, Han JH, Kwon HM (2019) Robot-assisted unicompartmental knee arthroplasty can reduce radiologic outliers compared to conventional techniques. PLoS ONE 14:e0225941
Park KK, Koh YG, Park KM, Park JH, Kang KT (2019) Biomechanical effect with respect to the sagittal positioning of the femoral component in unicompartmental knee arthroplasty. Biomed Mater Eng 30:171–182
Polat AE, Polat B, Gürpinar T, Peker B, Tüzüner T (2020) Factors affecting the functional outcome of oxford phase 3 unicompartmental knee arthroplasty. Acta Ortop Bras 28:78–83
Quan H, Li B, Couris CM, Fushimi K, Graham P, Hider P et al (2011) Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol 173:676–682
Ritter MA, Harty LD, Davis KE, Meding JB, Berend ME (2003) Predicting range of motion after total knee arthroplasty. Clustering, log-linear regression, and regression tree analysis. J Bone Joint Surg Am 85:1278–1285
Robinson BJ, Rees JL, Price AJ, Beard DJ, Murray DW, McLardy Smith P et al (2002) Dislocation of the bearing of the Oxford lateral unicompartmental arthroplasty. A radiological assessment. J Bone Joint Surg Br 84:653–657
Sekiguchi K, Nakamura S, Kuriyama S, Nishitani K, Ito H, Tanaka Y et al (2019) Effect of tibial component alignment on knee kinematics and ligament tension in medial unicompartmental knee arthroplasty. Bone Joint Res 8:126–135
Small SR, Berend ME, Rogge RD, Archer DB, Kingman AL, Ritter MA (2013) Tibial loading after UKA: evaluation of tibial slope, resection depth, medial shift and component rotation. J Arthroplasty 28:179–183
Suzuki T, Ryu K, Kojima K, Oikawa H, Saito S, Nagaoka M (2019) The effect of posterior tibial slope on joint gap and range of knee motion in mobile-bearing unicompartmental knee arthroplasty. J Arthroplasty 34:2909–2913
Takayama K, Matsumoto T, Muratsu H, Ishida K, Araki D, Matsushita T et al (2016) The influence of posterior tibial slope changes on joint gap and range of motion in unicompartmental knee arthroplasty. Knee 23:517–522
Tammachote N, Kriengburapha N, Chaiwuttisak A, Kanitnate S, Boontanapibul K (2018) Is Regular knee radiograph reliable enough to assess the knee prosthesis position? J Arthroplasty 33:3038–3042
Ueo T, Kihara Y, Ikeda N, Kawai J, Nakamura K, Hirokawa S (2011) Deep flexion-oriented bisurface-type knee joint and its tibial rotation that attributes its high performance of flexion. J Arthroplasty 26:476–482
Ware JE Jr, Kosinski M, Bayliss MS, McHorney CA, Rogers WH, Raczek A (1995) Comparison of methods for the scoring and statistical analysis of SF-36 health profile and summary measures: summary of results from the Medical Outcomes Study. Med Care 33:As264-279
Weale AE, Halabi OA, Jones PW, White SH (2001) Perceptions of outcomes after unicompartmental and total knee replacements. Clin Orthop Relat Res. https://doi.org/10.1097/00003086-200101000-00021143-153
Weber P, Schröder C, Schwiesau J, Utzschneider S, Steinbrück A, Pietschmann MF et al (2015) Increase in the tibial slope reduces wear after medial unicompartmental fixed-bearing arthroplasty of the knee. Biomed Res Int 2015:736826
Weber P, Woiczinski M, Steinbrück A, Schmidutz F, Niethammer T, Schröder C et al (2018) Increase in the tibial slope in unicondylar knee replacement: analysis of the effect on the kinematics and ligaments in a weight-bearing finite element model. Biomed Res Int 2018:8743604
World Medical Association (2013) World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 310:2191–2194
Xu S, Lim WJ, Chen JY, Lo NN, Chia SL, Tay DKJ et al (2019) The influence of obesity on clinical outcomes of fixed-bearing unicompartmental knee arthroplasty: a ten-year follow-up study. Bone Joint J 101-b:213–220
Funding
There is no funding source.
Author information
Authors and Affiliations
Contributions
YZK (Medical Student): Conceptualization, Methodology, Validation, Statistical Analysis, Data Collection, Writing—Original Draft, Writing—Review and Editing. MHLL (Orthopaedic Surgeon): Conceptualization, Methodology, Writing—Original Draft, Writing—Review and Editing, Supervision. ML (Orthopaedic Surgeon): Validation. JYC (Orthopaedic Surgeon): Supervision. NNL (Orthopaedic Surgeon): Surgeon, Supervision. SJY (Orthopaedic Surgeon): Surgeon, Supervision.
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Ethical approval
Yes.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Khow, Y.Z., Liow, M.H.L., Lee, M. et al. Posterior condylar offset and posterior tibial slope targets to optimize knee flexion after unicompartmental knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 30, 822–831 (2022). https://doi.org/10.1007/s00167-021-06453-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-021-06453-7