
Abstract
Purpose
The purpose of this study was to analyse unique injury data of the national statutory accident insurance for the two highest divisions in German male football (Bundesliga and 2. Bundesliga) over three consecutive seasons regarding inter-season, inter-division and inter-team differences.
Methods
This was a prospective observational open cohort study over the seasons 2014/2015, 2015/2016 and 2016/2017. Every acute injury that was registered by clubs or physicians with the German statutory accident insurance for professional athletes (VBG) as part of occupational accident reporting and that led to time loss and/or to medical attention, was included.
Results
The complete sample consisted of 1449 players. The study covered 2663.5 player seasons with an observed match exposure of 69,058 h and a projected training exposure of 529,136 h. In total, 7493 injuries were included. The overall incidence rate was 12.5 (± 0.28) injuries per 1000 exposure hours, which translated into match and training rates of 47.0 (± 1.62) and 8.02 (± 0.24) injuries per 1000 h, respectively.
Conclusion
Findings of 2.7 injuries per player and season underline the need of effective preventive approaches. Higher injury incidences in seasons after international tournaments suggest an increasing risk of injury with increasing number of matches. However, large differences between the single teams from the same division indicate that a reduction in the injury burden is generally possible. Continuing the presented injury surveillance might be helpful to identify injury trends in the future and to evaluate the effectiveness of preventive approaches under real-life conditions.
Level of evidence
Level II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Although football is related to several health benefits [20, 27], in particular on professional level it is also associated with a high risk of injuries [19, 23]. Up to 101 injuries per 1000 h of match play [1] with an increasing incidence [4] have been reported, particularly for certain injury types [16, 24]. This is proof of the great need for effective injury prevention approaches in professional football. In addition to the classic implementation models such as the “Sequence of Injury Prevention” [36] or the “TRIPP-Framework” [14], a number of papers have been published in the past years describing research frameworks leading to successful implementation of interventions in sport practice [32, 37, 38]. All of the existing implementation models share a common theme that the description of injury epidemiology within the target population is an integral part of the identification of preventive approaches. Considering the importance of the description of injury epidemiology, Fuller et al. [15] published a consensus statement on injury definitions and data collection procedures in studies of football injuries to ensure consistency and to increase inter-study comparability of epidemiologic data. As a result, several excellent epidemiologic publications are available providing helpful data for injury prevention. Having a closer look on current epidemiologic studies from professional male football, we notice that papers either describe tournaments and not regular league play [1, 22, 31, 33], or focus on single teams only and do not consider complete divisions, such as the outstanding UEFA Elite Club Injury Study [9] and others [3, 5, 16, 25, 26, 29, 30, 34]. Yet other studies mainly focus on single injury types or body locations [2, 7, 28, 35]. The current studies that address all injury types from complete professional divisions either do not cover European top leagues [4, 6, 21, 34] or analyse public media information with a high risk of bias [26]. Certainly, to our best knowledge, there is no current publication describing epidemiologic data from one of the Europe’s top leagues, covering complete divisions (complete squads from all clubs) in a longitudinal study design.
In Germany, there is a unique social insurance system including a statutory accident insurance for all employees. For the sector of professional athletes, the responsible statutory accident insurance is the Verwaltungs-Berufsgenossenschaft (VBG). Based on the presented state of the epidemiologic literature and the ensuing possibilities of the German insurance system, the aim of the present study is to perform a complete survey of all acute injuries of the two highest divisions in German male football over three consecutive seasons by analysing the unique data sample of the German statutory accidental insurance VBG. The leading questions we want to answer are whether an ongoing injury surveillance of all acute injuries by statutory insurances (1) is generally beneficial for the description of injury epidemiology, in particular with regard to (2) inter-season time trends, (3) differences between skill levels (divisions) and (4) inter-team differences within the same division. These results might deliver a best practice example for a continuous national injury surveillance and might support the development of future preventive approaches for injuries on professional level.
Materials and methods
This was a prospective observational open cohort study over three consecutive seasons (2014/2015, 2015/2016 and 2016/2017) that evaluated injuries in German professional male football. The study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement [39].
Inclusion criteria and definitions
Teams and participants
All first division [Bundesliga (BL1)] and second division [2. Bundesliga (BL2)] football players who competed in at least one competitive match for the respective 18 BL1 and 18 BL2 clubs during the 2014/2015, 2015/2016 and 2016/2017 seasons were included in this study. Each season extended from 1 July until 30 June of the subsequent year, resulting in a complete observation period from 1 July 2014 until 30 June 2017 (36 months).
In general, all participants were statistically considered to be one person. Players who played in both the first and second divisions during one season due to a club change were included in both collectives for comparisons between the divisions within one season (e.g. incidence rate 2014/2015 BL1 vs. BL2). Player seasons were calculated as the number of included players per season. Players who joined or left a team during the winter break only counted for a half player season on the respective team. If a player was part of a German first or second division team over the whole observation period and competed in at least one competitive match per season, this one person accounted for three player seasons.
Injuries
The present study followed the injury definition of the consensus statement on injury definitions and data collection procedures in football [15]. We included every acute injury of the included participants that was registered by clubs or physicians with the VBG as part of the occupational accident reporting that led to the player’s short-term disability (time loss) and/or to medical treatment costs (medical attention). Pain or chronic injury that was not of a post-traumatic nature as well as illnesses or mental impairments was not considered. Players who had an existing injury at the start of the observation period were not excluded from the study, but their existing injuries were not included as part of the study.
Recurrent injuries were defined as an injury of the same type and the specific muscle or ligament at the same site as an index injury that occurred after a player’s return to full participation from the index injury. A recurrent injury occurring within 2 months of a player’s return to full participation was referred to as an “early recurrence”, one occurring 2–12 months after a player’s return to full participation as a “late recurrence” and one occurring more than 12 months after a player’s return to full participation as a “delayed recurrence”. Injuries such as contusions, lacerations, concussions and sequelae resulting from the index injury were not recorded as recurrences, but always set as an index injury [15]. As we had no pre-study period injury data available, all first injuries that occurred during the observation time were set as an index injury.
Injury event
Since we had no comprehensive data of all test and friendly matches available, only injuries that occurred during competitive matches (official league play, national cup matches, international cup matches) were classified as match injuries. Identified injuries from friendly and test matches were classified as training injuries.
Data collection
Players’ baseline information
The personal data (name, date of birth, club, playing position) of all included participants were provided by the German Football League [“Deutsche Fußball Liga” (DFL)] and matched with open access data from the websites www.kicker.de and www.transfermarkt.de. The pseudonymised injury data were retrieved from the VBG database about 3 to 4 months after the close of the respective season as of 15 September. Thus, the duration or expected duration of time loss was also examined as of the data retrieval date of 15 September. It therefore must be noted that this is merely an excerpt of the total aforementioned cut-off date for the analyses. This approach enables a longitudinal comparison of the three seasons.
Match and training exposures
The match exposure was calculated by the number of competitive matches per included team multiplied with 11 (regular number of players per team on the pitch) and the duration of the match in hours (1.5 h or 2.0 h, respectively, for matches with extra time).
For calculation of the overall training exposure, five teams from the cohort could have been acquired to report exact training exposure in minutes of every single player. In that way, a total of ten complete team seasons out of the observation period were collected. These ten team seasons covered eight BL1 and two BL2 team seasons. Five of the BL1 team seasons represented teams that participated in international championships (UEFA Champions League, UEFA Europa League). Based on these data, the training exposure of the complete cohort and observational period was projected. For projection of the training exposure in BL1, the mean exposure of the BL1 internationally competing team seasons was multiplied by the number of teams that competed internationally in the respective season, and added to the mean exposure of the non-internationally competing FB1 team seasons multiplied by the number of the remaining FB1 teams. For BL2, the mean of the reported BL2 team seasons was multiplied by 18 (number of teams).
Since all personal data of the participants were available via open access, and the injury data were provided strictly pseudonymised by the VBG, the ethical committee of the Ruhr-Universität Bochum, Faculty of Sports Science, declared no ethical objections to this study design.
Statistical analysis
All statistical analyses were performed using IBM SPSS statistical software (version 25). Incidence rates were calculated as the number of injuries per 1000 h of exposure time with a corresponding 95% confidence interval (95% CI). Recurrent injuries are presented as total numbers and proportions (% of total number of injuries) and incidence per 1000 h (h) with a corresponding 95% CI. Burden is reported as the total number of days lost to injuries. Following the consensus statement of Fuller et al. [15], for the several injured body locations, total numbers and proportions (% of total number of injuries), the respective burden as mean (m) and standard deviation (SD) as well as the median and range of time loss are presented. In addition, total numbers and proportions (% of total number of injuries) grouped according to their severity are presented: slight (0 days); minimal (1–3 days); mild (4–7 days); moderate (8–28 days); and severe (> 28 days). Group comparisons with not given 95% CI, such as comparison of playing positions and affected body locations, were performed with the Chi-squared test or Fisher’s exact test.
For inter-team comparison of the injury burden of the single teams within the same division, slight and minimal injuries were excluded. The reason for this exclusion was that only injuries leading to at least 4 days of absence are mandated to be reported as part of the occupational accident reporting. Thus, the number and distribution of slight and minimal injuries may be biased by different reporting behaviours. To regard different demands, we additionally set the burden of the single clubs in relation to the number of competitive matches. Thus, inter-team comparisons were calculated using the following formula: “Cumulative injury burden resulting from reportable injuries (≥ 4 days) per team-season/number of competitive matches per team-season”.
The significance level for this study was set to p < 0.05.
Results
The complete sample consisted of 1449 players. In total, the study covered 2663.5 player seasons with an observed match exposure time over three consecutive seasons of 69,058 h of match play and a projected training exposure of 529,136 h. Within this period, 1275 players (88.0%) were injured at least once. On average, every included player sustained 2.7 injuries per season and consequently was not able to perform in match and training on 28 days.
Injuries and incidence rates
A total of 7493 injuries were registered and included in this study. Of these, 3247 (43.3%) occurred during match play and the remaining 4246 (56.7%) during training. 4033 injuries (53.8%) led to time loss. The overall incidence rate was 12.5 (± 0.28) injuries per 1000 h of exposure; this was 47.0 (± 1.62) injuries and 8.02 (± 0.24) injuries per 1000 h of match play and training, respectively. While the overall incidence rate and the training incidence rate was significantly higher in BL1 compared with BL2 teams, the match incidence rate in BL2 teams was significantly higher than in BL1 teams, as shown in Table 1. We also found significantly higher overall incidence rates in the first (2014/2015) and third observed seasons (2016/2017) compared with the second season (2015/2016) (Table 1).
Injury burden
The total burden equalled 77,761 days of absence, which equalled a total time loss of 213 years from the two divisions after three seasons (Table 1). More than one-fourth (27.3%) of the injuries were classified as moderate or severe injuries and led to at least 8 days of absence each. Particularly injuries of the knee led to long periods of absence up to 544 days (22.5; SD ± 55.0), followed by injuries of the shoulder (12.8; SD ± 23.4), the thigh (10.5; SD ± 19.7) and the ankle (10.1; SD ± 23.5) (Table 2).
Recurrent injuries
The overall rate of recurrent injuries was 7.1% (n = 532). Most recurrent injuries (47.7%; n = 254) occurred between 2 and 12 months after a player’s return to full participation (late recurrence), as shown in Table 3. Almost half of all recurrent injuries (48.1%; n = 256) were thigh injuries, particularly muscle injuries of the hamstrings and the adductors, followed by injuries of the ankle (24.6%; n = 131) and the knee (14.8%; n = 79). The resulting burden of these 466 recurrent injuries that affected the thigh, knee and ankle represented 6.2% of the total injuries, and led to 7355 absence days (9.5% of the total burden). BL1 and BL2 did not differ notably considering the distribution of recurrent injuries.
Injured body locations
Of all analysed injuries, 78.0% were of the lower extremities. The thigh (23.6%), knee (15.2%) and ankle (12.8%) were most commonly affected, as shown in Table 2. Comparison of the injury distribution on the single body locations between seasons, divisions and single teams showed no considerable differences. However, the distribution of the body regions was notably influenced by the playing position of the injured player. While head injuries were overrepresented in goalkeepers (GK) and defenders (DF), midfielders (MF) had significantly fewer head injuries. In addition, GK were overrepresented in upper limb injuries such as of the shoulder, elbow, forearm, wrist and hand/finger, but under-represented in thigh, lower leg, ankle and foot injuries. Furthermore, MF were overrepresented in ankle injuries (p < 0.001).
League and team differences
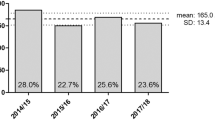
The number of competitive matches per team and season ranged from 35 to 56 in BL1 and from 35 to 40 in BL2. Figures 1 and 2 present the number of days lost to reportable injuries (> 4 days of time loss) in relation to the number of competitive matches per team and season. The mean for all BL1 teams ranged from 17.3 to 19.0 days of absence per competitive match over the three observed seasons with individual rates ranging from 4.7 to 33.4 (2014/2015), 9.1 to 34.7 (2015/2016) and 3.5 to 44.6 (2016/2017) (Fig. 1). For BL2 teams (Fig. 2), the mean burden ranged from 16.1 to 19.0 days of absence per competitive match, with individual rates ranging from 2.6 to 37.7 (2014/2015), 6.1 to 40.7 (2015/2016) and 4.9 to 30.3 (2015/2016).

Ranges of days lost to reportable injuries (time loss ≥ 4 days) in relation to the number of competitive matches over three consecutive seasons in BL1 from low (1) to high (18) (the respective ranks from 1 to 18 in ascending order do not necessarily reflect the same pseudonymised team over the three observed seasons)

Ranges of days lost to reportable injuries (time loss ≥ 4 days) in relation to the number of competitive matches over three consecutive seasons in BL2 from low (1) to high (18) (the respective ranks from 1 to 18 in ascending order do not necessarily reflect the same pseudonymised team over the three observed seasons)
Discussion
The main findings of the study were that (1) overall injury incidences differ significantly between the three observed seasons; (2) incidence rates differ significantly in comparison of the two divisions; and (3) injury burden of the single teams within one division differs considerably in all three observed seasons.
The main importance of preventive approaches for lower limb injuries, in particular for injuries of the thigh, the knee and the ankle [4, 16, 19, 23], can be underlined by the findings of their study. In German professional male football, these three body locations are affected in every other injury (51.6%) and are responsible for 75.8% of the overall injury burden. Furthermore, recurrence injuries of these three body locations account for at least 9.5% of the total burden—despite the possible resulting subsequent injuries. Although the effectiveness of existing injury prevention training programmes is presented in a large amount of evidence under a wide variety of circumstances, settings and populations, for both overall injury rate and particular injury types, including hamstring muscle injuries, ACL ruptures and ankle sprains [13], the injury burden is still high in professional football [9, 18, 40] and has not decreased much during the past 15 years [8, 12].
An explanation for the identified higher incidence rates of the first and third observed season compared with the second one might be that the international tournaments, FIFA World Cup 2014 and UEFA Euro 2016, occurred prior to both seasons. It has been demonstrated by Ekstrand et al. [11] that teams with no or shortened winter breaks showed higher injury rates than teams with winter breaks. The same reasoning of a shortened time for regeneration and pre-season preparation in combination with a higher number of matches for single players might be reasonable for our finding. As a consequence, programme design, load monitoring and regeneration management seem to be topics of high relevance to reduce injury burden—particularly in seasons after international tournaments.
In the comparison of the two observed divisions, we found higher overall and training incidence rates in BL1 compared with BL2, but higher match incidence rates in BL2 compared with BL1. They conclude that the higher overall incidence rates in BL1 can be explained by the higher intensity and a greater number of matches, and as a consequence, more travel and less time for regeneration. However, a more rugged and less technique-orientated playing style at lower performance levels might be reason for the higher match injury incidences in BL2.
Foremost, it should be mentioned that the injury burden in relation to the number of competitive matches of the single teams within one division over the three seasons differed considerably by a factor of 3.8–12.6 in BL1 and 6.1–14.5 in BL2. These wide ranges indicate that a reduction in the injury burden seems generally possible—even under the circumstances of professional football. We consider that the large variations in injury burden demonstrate that some teams and coaching staffs are better than others concerning their (medical and sports scientific) player support in terms of individual internal and external player load management [17], the implementation of evidence-based injury prevention programmes into daily training routine [12], and their communication and leadership style [10].
There were some limitations to the current study. (1) We had no pre-study injury history available. As a result, the number of recurrent injuries was likely higher than stated in this study. At the same time, this is the explanation for why recurrent injury rates increased over the study period. (2) Classification of the injury event (match, training) was performed by matching the date of injury with the match schedule of the single teams. We suggested that any injury that occurred on the date of a competitive match of the respective club did occur during the match and consequently was defined as a match injury. However, there is a possibility that the injury occurred during the warm-up or other activities besides the competitive match, and thus, this may bias the match-to-training injury ratio. (3) As stated in the methods section, training exposures were projected by the reporting of single teams, since we had no comprehensive training exposure data available. Real training exposure might deviate and consequently bias the stated training injury incidence. In addition, also for the calculation of match exposure as stated in the methods, a risk of bias cannot be excluded. (4) Likewise, as already pointed out in the methods, only injuries leading to at least 4 days of absence are mandated to be reported as part of the occupational accident reporting. As a result, the number of slight and minimal injuries and their distribution across divisions, seasons and body locations may be biased. Exceptions to this risk of bias were comparison of single teams from the same division, in which we focused on mandatory reportable injuries only.
The main strengths of this study were the large long-term prospective data set of professional football, covering all players from all teams, and use of the same data collection procedures and definitions across seasons. To the best of our knowledge, there is no other current complete survey over three consecutive seasons from one of the Europe’s top leagues.
Conclusion
This study presents results of a new national injury surveillance, analysing epidemiologic data of German professional male football from the responsible German statutory accident insurance. The findings of 2.7 injuries per player and season underline the need of effective preventive approaches on professional level, in particular for injuries of the thigh, the knee and the ankle. Significantly higher incidence rates in seasons after international tournaments (FIFA World Cup 2014 and UEFA Euro 2016) suggest a correlation between the number of competitive matches (and resulting shortened breaks) and risk of injury. Thus, programme design, load monitoring and regeneration management seem to be further topics of high relevance to reduce injuries. However, big differences concerning the injury burden in relation to the respective number of competitive matches between the single teams from one division indicate that a reduction in the injury burden is generally possible—even under the given circumstances of professional football. Continuing the presented injury surveillance might be beneficial for the identification of injury trends in the future and evaluation of the effectiveness of preventive approaches under real-life conditions.
References
Almutawa M, Scott M, George KP et al (2014) The incidence and nature of injuries sustained on grass and 3rd generation artificial turf. Phys Ther Sport 15(1):47–52
Beaudouin F, aus der Fünten K, Tross T et al (2017) Head injuries in professional male football (soccer) over 13 years. Br J Sports Med. https://doi.org/10.1136/bjsports-2016-097217
Benito del Pozo L, Ayán Pérez C, Revuelta Benzanilla G et al (2014) Influence of the soccer players’ professional status on the frequency and severity of injuries. Apunts. Medicina de l’Esport 49(181):20–24
Bjørneboe J, Bahr R, Andersen TE (2012) Gradual increase in the risk of match injury in Norwegian male professional football. Scand J Med Sci Sports 24(1):189–196
Carling C, McCall A, Le Gall F et al (2015) The impact of in-season national team soccer play on injury and player availability in a professional club. J Sports Sci 33(17):1751–1757
Eirale C, Tol JL, Farooq A et al (2013) Low injury rate strongly correlates with team success in Qatari professional football. Br J Sports Med 47(12):807–808
Eirale C, Tol JL, Targett S et al (2015) Concussion surveillance. Clin J Sport Med 25(1):73–74
Ekstrand J, Hagglund M, Kristenson K et al (2013) Fewer ligament injuries but no preventive effect on muscle injuries and severe injuries. Br J Sports Med 47(12):732–737
Ekstrand J, Hagglund M, Walden M (2011) Injury incidence and injury patterns in professional football. Br J Sports Med 45(7):553–558
Ekstrand J, Lundqvist D, Lagerbäck L et al (2018) Is there a correlation between coaches’ leadership styles and injuries in elite football teams? A study of 36 elite teams in 17 countries. Br J Sports Med 52(8):527–531
Ekstrand J, Spreco A, Davison M (2018) Elite football teams that do not have a winter break lose on average 303 player-days more per season to injuries than those teams that do. Br J Sports Med. https://doi.org/10.1136/bjsports-2018-099506
Ekstrand J, Walden M, Hagglund M (2016) Hamstring injuries have increased by 4% annually in men’s professional football, since 2001. Br J Sports Med 50(12):731–737
Faude O, Rommers N, Rössler R (2018) Exercise-based injury prevention in football. Ger J Exerc Sport Res 48(2):157–168
Finch C (2006) A new framework for research leading to sports injury prevention. J Sci Med Sport 9(1–2):3–9 (discussion 10)
Fuller CW, Ekstrand J, Junge A et al (2006) Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Br J Sports Med 40(3):193–201
aus der Fünten K, Faude O, Lensch J et al (2014) Injury characteristics in the German professional male soccer leagues after a shortened winter break. J Athl Train 49(6):786–793
Gabbett TJ (2016) The training—injury prevention paradox. Br J Sports Med 50(5):273
Hägglund M, Waldén M, Magnusson H et al (2013) Injuries affect team performance negatively in professional football. Br J Sports Med 47(12):738–742
Hagglund M, Walden M, Ekstrand J (2016) Injury recurrence is lower at the highest professional football level than at national and amateur levels. Br J Sports Med 50(12):751–758
Hammami A, Chamari K, Slimani M et al (2016) Effects of recreational soccer on physical fitness and health indices in sedentary healthy and unhealthy subjects. Biol Sport 33(2):127–137
Haxhiu B, Murtezani A, Zahiti B et al (2015) Risk factors for injuries in professional football players. Folia Med (Plovdiv) 57(2):138–143
Junge A, Dvorak J (2015) Football injuries during the 2014 FIFA World Cup. Br J Sports Med 49(9):599–602
Klein C, Henke T, Platen P (2018) Injuries in football (soccer)—a systematic review of epidemiology and aetiological aspects. Ger J Exerc Sport Res 48(3):309–322
Krutsch W, Zeman F, Zellner J et al (2016) Increase in ACL and PCL injuries after implementation of a new professional football league. Knee Surg Sports Traumatol Arthrosc 24(7):2271–2279
Larruskain J, Lekue JA, Diaz N et al (2018) A comparison of injuries in elite male and female football players. Scand J Med Sci Sports 28(1):237–245
Leventer L, Eek F, Hofstetter S et al (2016) Injury patterns among elite football players. Int J Sports Med 37(11):898–908
Milanović Z, Pantelić S, Kostić R et al (2015) Soccer vs. running training effects in young adult men. Biol Sport 32(4):301–305
Mosler AB, Weir A, Eirale C et al (2018) Epidemiology of time loss groin injuries in a men’s professional football league. Br J Sports Med 52(5):292–297
Noya Salces J, Gomez-Carmona PM, Moliner-Urdiales D et al (2014) An examination of injuries in Spanish Professional Soccer League. J Sports Med Phys Fitness 54(6):765–771
Noya Salces J, Gomez-Carmona PM, Gracia-Marco L et al (2014) Epidemiology of injuries in first division Spanish football. J Sports Sci 32(13):1263–1270
Nuhu A, Kutz M (2016) Descriptive epidemiology of soccer injury during elite international competition in Africa. Int J Athl Ther Train. 22(2):21–28
Padua DA, Frank B, Donaldson A et al (2014) Seven steps for developing and implementing a preventive training program. Clin in Sports Med 33(4):615–632
Pangrazio O, Forriol F (2016) Epidemiology of soccer players traumatic injuries during the 2015 America Cup. Muscles Ligaments Tendons J 6(1):124–130
Stubbe JH, van Beijsterveldt A-MMC, van der Knaap S et al (2015) Injuries in professional male soccer players in the Netherlands. J Athl Train 50(2):211–216
Svensson K, Alricsson M, Karneback G et al (2016) Muscle injuries of the lower extremity. Knee Surg Sports Traumatol Arthrosc 24(7):2293–2299
van Mechelen W, Hlobil H, Kemper HC (1992) Incidence, severity, aetiology and prevention of sports injuries. A review of concepts. Sports Med 14(2):82–99
van Tiggelen D, Wickes S, Stevens V et al (2008) Effective prevention of sports injuries. Br J Sports Med 42(8):648–652
Verhagen E, Voogt N, Bruinsma A et al (2014) A knowledge transfer scheme to bridge the gap between science and practice. Br J Sports Med 48(8):698
von Elm E, Altman DG, Egger M et al (2014) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Int J Surg 12(12):1495–1499
Waldén M, Hägglund M, Magnusson H et al (2016) ACL injuries in men’s professional football. Br J Sports Med 50(12):744
Acknowledgements
The authors wish to thank all the participating clubs including coaches, players and medical staff. Data analyst Katja Burkhardt is acknowledged for aggregating and pseudonymising the injury data from the VBG data warehouse.
Funding
This study received no funding to compete.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no competing interests.
Ethical approval
The ethical committee of the Ruhr-Universität Bochum, Bochum, Germany, Faculty of Sports Science, declared no ethical objections to this study design.
Research involving human and animal participants
This article does not contain any studies with human participants or animals performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Klein, C., Luig, P., Henke, T. et al. Injury burden differs considerably between single teams from German professional male football (soccer): surveillance of three consecutive seasons. Knee Surg Sports Traumatol Arthrosc 28, 1656–1664 (2020). https://doi.org/10.1007/s00167-019-05623-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05623-y