
Abstract
Purpose
The aim of this study was to compare femoral tunnel enlargement after anterior cruciate ligament (ACL) reconstruction surgery using hamstring autograft tendons fixed by bioabsorbable femoral trans-tunnel pins with that in patients in which the graft was fixed with extracortical fixation.
Methods
Forty-three patients were randomly selected from our database and included in the study. Femoral tunnel diameter was measured by computed tomography in 20 patients who underwent ACL reconstruction via anteromedial portal technique using autologous quadruple hamstrings, fixed with two bioabsorbable trans-tunnel pins, RigidFix, on the femoral side and compared with 23 patients in whom extracortical fixation, EndoButton CL, was used. The diameter of the femoral tunnel was measured at a distance of 5 mm from the tunnel entrance and at the largest diameter along the tunnel axis. Data were compared with the diameter of the drill used during surgery. Clinical evaluation was performed using the Lysholm score, IKDC subjective score and anterior knee laxity measurements.
Results
Femoral tunnel enlargement 5 mm from the entrance and at the largest diameter was greater in the RigidFix group than the EndoButton group. There were no significant differences between the two groups regarding age, gender, post-operative Lysholm score, IKDC subjective score or knee laxity measurements.
Conclusion
The present study showed greater enlargement of the femoral bone tunnel when a bioabsorbable trans-tunnel pin system was used with the medial portal technique when compared to extracortical fixation. These findings confirm that femoral tunnel widening should be considered when RigidFix was used in ACL reconstruction by anteromedial portal technique.
Level of evidence
III.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The intra-articular reconstruction of the anterior cruciate ligament (ACL) is a well-established surgical procedure for treatment of anterior instability of the knee [2]. Ligament reconstruction with hamstrings is a technique with advantages such as preservation of the extensor mechanism, a lower rate of patellofemoral symptoms when compared to patellar grafts and the minimization of flexion contractures [9, 10, 16, 18, 20]. With the increasing number of ACL reconstructions being performed, surgeons should consider the potential complications of this technique, which can be preoperative, intra-operative or post-operative. Among the post-operative complications, the most frequent are the recurrence of instability, pain, limitation of motion, patellofemoral complications and bone tunnel enlargement [4, 8].
Bone tunnel enlargement is a common complication observed up to 1 year after ACL reconstruction with hamstrings [1, 11–36]. Some studies have suggested that bone tunnel widening stabilizes by 6 months after surgery [11–15]. The aetiology of such enlargement remains unknown. Several explanations, based on possible mechanical and biological factors, have been postulated. Among the mechanical factors are the unwanted mobility of the graft within the tunnel, the non-anatomical location of the tunnels and accelerated post-operative rehabilitation [1]. Inflammatory reactions in response to the presence of biological material inside the bone tunnel may also be associated with enlargement [15].
Although bone tunnel widening is a frequent complication seen in ACL reconstructions using hamstrings, it remains unclear whether the enlargement of bone tunnels is correlated with poor clinical results [11–37]. The main impact of bone tunnel widening is on patients requiring revision surgery. A large bone tunnel may hinder the revision surgery, and bone grafting in a staged procedure may be required [13].
Regarding fixation methods, the RigidFix system (Mitek, Norwood, MA) consists of two bioabsorbable trans-tunnel pins of polylactic acid used to fix the graft into the femoral tunnel. One of the two pins in the RigidFix system is positioned close to the intra-articular opening of the tunnel, which theoretically could decrease the mobility of the graft in the bone tunnel [14, 18]. On the other hand, extracortical fixation using EndoButton CL (Smith & Nephew, Andover, MA) is a very popular method of fixation due to its stability [5]. The extracortical fixation allows for greater movement of the graft within the bone tunnel [19].
This study aimed to compare femoral tunnel enlargement in ACL reconstruction using hamstring autograft tendons fixed by two bioabsorbable trans-tunnel pins with that in patients in which the graft was fixed with extracortical fixation. The hypothesis was that less enlargement of the femoral tunnel occurs when bioabsorbable trans-tunnel pins are used compared with extracortical fixation.
Materials and methods
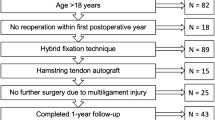
Forty-three patients were randomly selected from our database and included in the study. For selection process, the authors identified in the IOT Hospital of Trauma database a total of 63 patients who met the inclusion criteria of the study. Thirty-three patients underwent ACL reconstruction using EndoButton CL (EndoButton group) and 30 using RigidFix (RigidFix group) for femoral fixation. In each group, all subjects were numbered and sorted according to the date of surgery in descending order of follow-up (1–33, 1–30). A random sequence was created using a random sequence generator (www.random.org). The first 20 and 23 subjects from each randomized list were evaluated.
Femoral tunnel diameter was measured in 20 patients who underwent ACL reconstruction via anteromedial portal technique using autologous quadruple hamstrings, fixed with RigidFix (Mitek, Norwood, MA) on the femoral side, RigidFix group, and compared with 23 patients in who extracortical fixation, EndoButton CL (Smith & Nephew, Andover, MA), was used. On the tibial side, all grafts were fixed with a bioabsorbable interference screw. The median of the follow-up time was 12 months (range 12–18) in the RigidFix group and 13 months (range 12–20) in the EndoButton group. There were 21 men and 2 women in the EndoButton group with a median of age 40 years (range 16–57), while the RigidFix group included 18 men and 2 women with a median of age 29 years (range 16–48). Surgeries took place between 2010 and 2012, and the same team of surgeons operated on all patients at a referral and teaching hospital.
The femoral tunnel diameters were measured using computed tomography (CT) images in patients with at least 1 year after surgery. Two independent radiologists recorded the measurements, considering the diameter of the femoral tunnel at 5 mm inside the entrance and the greatest diameter along the longitudinal axis of the femoral tunnel (Figs. 1, 2). Tunnel enlargement was defined decreasing the data obtained with the diameter of the drill used to create the femoral tunnel during surgery. By measuring the diameter of the tunnel at a distance of 5 mm from the entrance, errors in measuring the diameter of the tunnel due to obliquity of entrance, on the medial side of the femoral condyle, are eliminated. All examinations were performed using the same equipment (64-channel multislice computed tomography model Toshiba Aquilion TSX-101A). Multislice CT allows an assessment of the tunnels in a reliable manner without the amplification commonly found on radiographs [12] and thus the measurement of the three-dimensional bone tunnel with precise definition of the axis. The accuracy of the method used is 0.1 mm. Intra- and interobserver reproducibility of measurements was assessed by interclass coefficients.

Measurements of femoral tunnel diameter, using multislice CT images for cortical fixation (EndoButton) group

Measurements of femoral tunnel diameter, using Multislice CT images cortical for RigidFix group
Clinical evaluation of the outcome was conducted using the Lysholm score, the International Knee Documentation Committee (IKDC) subjective score and an objective measurement of knee laxity using a Rolimeter (Aircast, Florida, USA).
There were no significant differences between the two groups regarding gender, post-operative Lysholm score, IKDC subjective score and knee laxity measurements. Age differed significantly between groups, being the parameter adjusted to groups (Table 1).
The CT scan was performed exclusively for the study. All patients underwent the same protocol of post-operative rehabilitation. The Bioethics’ Committee of the University of Passo Fundo approved the study (#216/2010), and all patients signed an informed consent form.
Surgical technique for ACL reconstruction using EndoButton
The patient is positioned supine with spinal anaesthesia associated with ipsilateral femoral nerve anaesthesia. After routine procedures for surgery being performed, the gracilis and semitendinosus tendons are identified and withdrawn. Krackow sutures using Ethibond 2-0 are performed at the end of the grafts. The tendons are folded to form a quadruple graft. Arthroscopy of the knee joint through the anteromedial and anterolateral portals is performed. A guide wire is introduced via the anteromedial portal placed in the centre of the femoral insertion of the ACL with the knee in 120° of flexion. Via the anteromedial portal and guided by the wire, a femoral tunnel is made measuring 30 mm in length and the same diameter as the proximal tendon graft prepared earlier. The tibial tunnel is made using the tibial guide with 45° of angulation, positioned in the centre of the ACL tibial insertion site. The graft is passed through the tibial and femoral tunnels under arthroscopic guidance. The graft is fixed on the femoral side using EndoButton CL with 15 mm of loop. After that, the knee is positioned in 30° of knee flexion and the graft is fixed on the tibial side using a bioabsorbable interference screw (Fig. 1).
Surgical technique for ACL reconstruction using RigidFix system
Patient positioning, anaesthesia, graft harvesting and their preparation, the tibial and femoral tunnels and tibial fixation are as described above. However, when using RigidFix, the femoral guide is introduced via the anteromedial portal and positioned within the femoral tunnel. Using the guide, two cannulated guides for the introduction of RigidFix are fixed at the lateral condyle through accessory incisions. The graft is passed through bone tunnels under guidance, and graft femoral fixation is performed using the RigidFix system (Fig. 2).
Statistical analysis
Statistical analysis was performed using SPSS version 21.0. Quantitative variables were described using the mean and standard deviation or median and interquartile range. Categorical variables were described using absolute and relative frequencies. To compare means between groups, Student’s t test was applied. In cases of non-normality, the Mann–Whitney test was used. Comparison of proportions was made using the Pearson’s Chi-square test or Fisher’s exact. The level of significance was set at 5 % (p < 0.05). Sample size calculation was based on the difference between two means. With a standard deviation of 2.4 mm, a difference of 2.0 mm to be detected, 5 % significance level, 80 % statistical power and a two-tailed test, the minimum sample size necessary for each group was estimated to be 18. Intra- and interobserver reproducibility of the continuous variables was assessed by intra-class coefficients.
Results
The data of tunnel diameter measurements and enlargement are summarized in Table 2. A significant difference was found between groups in all variables analysed (p < 0.01) The RigidFix group showed the widest femoral tunnel enlargement (Figs. 3, 4).

Proportion of femoral tunnel enlargement at 5 mm from inlet considering cutting-off points

Proportion of femoral tunnel enlargement at largest diameter considering cutting-off points
The intra-class and interclass coefficients were 0.99 and 0.98 for all measurements.
Discussion
The main finding of the present study was that greater enlargement of the femoral tunnel was observed in patients in which RigidFix was used for femoral fixation after hamstring ACL reconstruction via anteromedial portal technique. The exact aetiology of tunnel widening remains unknown. Many mechanical and biological factors have been associated with tunnel enlargement in ACL reconstruction including graft choice, graft fixation methods, improper tunnel placement, cytokine levels in the synovial fluid and accelerated rehabilitation [10–21].
In the present study, the authors compared femoral tunnel widening in a group of patients that underwent ACL reconstruction with hamstrings using RigidFix for femoral fixation with that in patients in whom EndoButton fixation was used. Theoretically, a double bioabsorbable trans-tunnel pin system promotes rigid fixation due to the presence of the second pin near the joint, which may decrease graft motion at the entrance of the tunnel [14, 18]. As a control group, we also analysed and quantified tunnel widening in patients who underwent ACL reconstruction with hamstrings using extracortical fixation. The use of extracortical fixation as the control group was considered because it hypothetically represents the worst scenario for the development of tunnel enlargement as it involves fixation outside the tunnel aperture [37]. Contrary to our hypothesis, the results showed a high incidence of tunnel enlargement on the femur side when RigidFix was used.
The method of graft fixation may be an important factor underlying bone tunnel widening. Some authors have demonstrated that extracortical graft fixation increases the movement of the graft inside the bone tunnel and at the intra-articular aperture (bungee cord effect and windshield wiper effect, respectively) [37]. In a prospective randomized study, Fauno et al. [19] evaluated the incidence of tunnel widening in patients who underwent ACL reconstruction with hamstring grafts using trans-femoral fixation associated with an interference screw in the tibia and compared this to widening in patients in whom cortical fixation in the femoral and tibia was used. The authors concluded that there was a reduction in tunnel enlargement in patients in which fixation was closer to the joint. Iorio et al. [22] performed computed tomography to evaluate bone tunnel enlargement in 25 patients who underwent two-incision arthroscopic ACL reconstruction with a quadruple hamstring autograft using very strong graft fixation close to the joint line. They observed that the rate of tunnel widening seemed to be minimized when anatomical, stiff and strong fixation was combined with a less aggressive rehabilitation program [22]. Ma et al. [26] found no significant difference in bone tunnel enlargement between patients who underwent hamstring ACL reconstruction with aperture graft fixation using a bioabsorbable interference screw compared with patients in whom extracortical fixation was achieved using EndoButton, with the exception of the femoral tunnel in the sagittal plane, in which tunnel expansion was higher in the bioabsorbable screw group. In a recent prospective randomized study comparing femoral tunnel widening evaluated by CT scan in patients who had undergone ACL reconstruction with hamstring grafts, Sabat et al. concluded that femoral tunnel widening was significantly lower in patients that used TransFix (Arthrex, Naples, FL) compared to that in patients in whom EndoButton CL (Smith & Nephew Endoscopy, Andover, MA) was used. In the present study, the RigidFix group showed significantly higher values in all analyses compared with the EndoButton group. Recently, new adjustable-length loop device for lateral cortical fixation became very popular aiming to decrease the elasticity of the system with the graft filling the entire length of the femoral tunnel. However, a controlled laboratory study [6] has shown that the suspensory cortical fixation of the graft using adjustable-length loop devices allowed more cyclic and initial displacement. Therefore, there were no data about tunnel widening when these adjustable-length loop devices were used [6, 30].
Although many studies have examined bone tunnel widening in ACL reconstruction, only a few studies have addressed the enlargement of the femoral tunnel when the RigidFix system was used [3, 7–14]. Arce et al. [3] evaluated the enlargement of the femoral tunnel by radiographs in 66 patients who underwent trans-tibial ACL reconstructions using hamstrings with two bioabsorbable crossed pins (RigidFix, Mitek) or titanium cross pinning (TransFix, Arthrex). They found an enlargement of 62 and 49 % in the 6 months after surgery and 24 and 21 %, respectively, at the end of 1 year post-operatively. The authors concluded that bone tunnel widening appears to be lower when fixation takes place closer to the joint.
Cinar et al. [14] used multislice computed tomography to evaluate the enlargement of the femoral and tibial tunnels in patients after ACL reconstruction using hamstrings fixed with RigidFix or EndoButton and correlated the results with the anatomical and non-anatomical position of the tunnels. They found marked and excessive tunnel enlargement in 77.8 % of patients in the RigidFix group and 88.2 % in the EndoButton group. There was no difference in enlargement according to the positioning of the tunnels, regardless of the fixation method. In our study, the femoral tunnel showed an average increase of 61.9 % compared to the initial tunnel in the RigidFix group and a 26.3 % increase in the EndoButton group. The difference between the two groups was significant. Basad et al. [7] used MRI to compare the enlargement of the femoral tunnel after RigidFix or EndoButton had been used for femoral fixation. Contrary to the results presented, they found no bone tunnel widening associated with any type of fixation.
It is also important to point out that besides the mechanical factors related to fixation devices, chemical and biological factors might contribute to bone tunnel widening. The degradation of absorbable material could create a chemical osmotic effect inside the bone tunnel that could promote widening. A foreign body response, thermal necrosis after drilling and synovial fluid propagation into the bone tunnel could also be additional causes [29, 34]. The present authors suggest that the absorbable material that composes the RigidFix and the soft tissue graft used may contribute to the development of femoral tunnel enlargement.
Some studies have reported a higher rate of bone tunnel enlargement after ACL reconstruction using hamstrings [18, 24, 32, 33, 36] when compared to patellar tendon. Webster et al. [36] published a randomized comparison of tunnel widening among 65 patients who had undergone ACL reconstructions using either a hamstring or bone–patellar tendon–bone autograft with EndoButton fixation on the femoral side and metal interference screw on the tibial side. The authors concluded that tunnel widening was higher in patients that used a hamstring graft.
The strength of this study is that all patients were evaluated by computed tomography images. In a recent study, Marchant et al. [27] concluded that computed tomography is more reliable and superior to radiographs and MRI regarding both tunnel identification and quantification.
This study did not evaluate tibial tunnel widening. A bioabsorbable interference screw was used for tibial fixation in all patients. The diameter of the drill used at the time of surgery does not provide reliable baseline data because when interference screws are used, they may mechanically enlarge the tunnel diameter during the fixation step.
The main limitations of the present study include being a small retrospective cohort, no measurement of the femoral tunnel immediately after surgery and short follow-up. Although both groups of individuals differ in age, there are no studies that clearly link enlargement of the bone tunnels with age. Because of this, the authors do not consider the difference in age as a limitation of the study.
In a recent study, Sabat et al. [31] found no difference between the diameter of the femoral tunnel measured by CT scan 2 weeks post-operatively and the intra-operative drill diameters used. Thus, no excess radiation exposure is justified at the baseline for femoral tunnel evaluation. Likewise, in the present study, there was no need for exposure of a greater number of individuals to radiation. The authors aimed to measure the diameter of the femoral tunnel regardless of the success of the clinical outcomes as the endpoint. The short duration of follow-up and the small number of patients evaluated do not allow conclusions to be made about differences in clinical outcomes. Both groups, in general, showed good clinical outcomes despite the presence of bone tunnel widening.
The findings of the present study confirm that femoral tunnel widening should be considered when RigidFix was used in ACL reconstruction by anteromedial portal technique, and it should be carefully evaluated before revision ACL reconstruction.
Conclusions
The present study showed greater enlargement of the femoral bone tunnel when using a RigidFix for hamstring ACL reconstruction via the anteromedial portal technique when compared to extracortical fixation method. Femoral tunnel enlargement was also greater when compared with the EndoButton fixation method.
References
Achtnich A, Stiepani H, Forkel P, Metzlaff S, Hänninen EL, Petersen W (2013) Tunnel widening after anatomic double-bundle and mid-position single-bundle anterior cruciate ligament reconstruction. Arthroscopy 29(9):1514–1524
Allen MK, Glasoe WM (2000) Metrecom measurement of navicular drops in subjects with anterior cruciate ligament. J Athl Train 35:403–406
Arce G, Lacroze P, Previgliano J, Constanza E, Cañete M (2008) Widening the bony tunnels after anterior cruciate ligament repair. J Bone Joint Surg Br 90((SUPPL II)):281
Arendt E, Dick R (1995) Knee injury patterns among men and women in collegiate basketball and soccer: NCAA data and review of literature. Am J Sports Med 23:694–701
Barrett GR, Papendick L, Miller C (1995) Endobutton button endoscopic fixation technique in anterior cruciate ligament reconstruction. Arthroscopy 11:340–343
Barrow AE, Pilia M, Guda T, Kadrmas WR, Burns TC (2014) Femoral suspension devices for anterior cruciate ligament reconstruction: do adjustable loops lengthen? Am J Sports Med 42(2):343–349
Basad E, Kipper A, Wüsten OA, Sturz H, Ishaque BA (2010) Comparative study after hamstring ACL plasty with RigidFix (pin fixation) and Endobutton (anchor fixation). Z Orthop Unfall 148(3):276–281
Benjaminse A, Gokeler A, Van der Schans CP (2006) Clinical diagnosis of an anterior cruciate ligament rupture: a meta-analysis. J Orthop Sports Phys Ther 36:267–288
Beynnon BD, Johnson RJ, Abate JA, Fleming BC, Nochols CE (2005) Treatment of anterior cruciate ligament injuries. Part I. Am J Sports Med 33:1579–1602
Biau DJ, Toumoux C, Katsahian S, Schranz PJ, Nizard RS (2006) Bone-patellar tendon-bone autograft versus hamstring autograft for reconstruction of anterior cruciate ligament: meta-analysis. BMJ 332:995–1001
Buelow J-U, Siebold R, Ellermann A (2002) A prospective evaluation of tunnel enlargement in ACL reconstruction with hamstrings: extracortical versus anatomical fixation. Knee Surg Sports Traumatol Arthrosc 10:80–85
Chhabra A, Kline AJ, Nilles KM, Harner CD (2006) Tunnel expansion after anterior cruciate ligament reconstruction with autogenous hamstrings: a comparison of the medial portal and transtibial techniques. Arthroscopy 22:1107–1112
Choi NH, Lee JH, Son KM, Victoroff BN (2010) Tibial tunnel widening after anterior cruciate ligament reconstructions with hamstring tendons using Rigidfix femoral fixation and Intrafix tibial fixation. Knee Surg Sports Traumatol Arthrosc 18(1):92–97
Cinar BM, Hersekli MA, Cesur N, Poubargher A, Derincek A (2009) The effects of two different fixation methods on femoral bone tunnel enlargement and clinical results in anterior cruciate ligament reconstruction with hamstring tendon graft. Zhonghua Yi Xue Za Zhi 89(29):2034–2037
Clatworthy MG, Annear P, Buelow JU, Bartlett RJ (1999) Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patellar tendon grafts. Knee Surg Sports Traumatol Arthrosc 7:138–145
Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA (1999) Arthroscopic reconstruction of the anterior cruciate ligament: a comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 27(3):444–454
Dejour H, Deschamps G, Walch G (1984) Resultat du traitement des laxities anterieures chroniques par operation de Kenneth Jones-Lemaire. J Lyon Chir Genou 5:129–140
Ejerhed L, Kartus J, Sernert N, Köhler N, Karlsson J (2003) Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med 31:19–25
Fauno P, Kaalund S (2005) Tunnel widening after hamstring ACL reconstruction is influenced by the type of graft fixation used: a prospective randomized study. Arthroscopy 21(11):1337–1341
Gomes JLE, Marczyk LR (1984) Anterior cruciate reconstruction with a loop or double thickness of semitendinosus tendon. Am J Sports Med 12(3):199–203
Höher J, Möller HD, Fu FH (2008) Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc 6:231–240
Iorio R, Vadalà A, Argento G, Di Sanzo V, Ferretti A (2007) Bone tunnel enlargement after ACL reconstruction using autologous hamstring tendon: a CT study. Int Orthop 31:49–55
Jarvela T, Moisala AS, Paakkala T, Paakkala A (2008) Tunnel enlargement after double-bundle anterior cruciate ligament reconstruction: a prospective, randomized study. Arthroscopy 24(12):1349–1357
Kobayashi M, Nakagawa Y, Suzuki T, Okudaia S, Nakamura T (2006) A retrospective review of bone tunnel enlargement after anterior cruciate ligament reconstruction with hamstring. Arthroscopy 22(10):1093–1099
L´Insalata JC, Klatt B, Fu FH, Harner CD (1997) Tunnel expansion following anterior cruciate ligament reconstruction: a comparison of hamstring and patellar tendon autografts. Knee Surg Sports Traumatol Arthrosc 5:234–238
Ma CB, Francis K, Towers J, Irrgang J, Fu FH, Harner CH (2004) Hamstring anterior cruciate ligament reconstruction: a comparison of bioabsorbable interference screw and endobutton-post fixation. Arthroscopy 20(2):122–128
Marchant MH Jr, Willimon SC, Vinson E, Pietrobon R, Garrett WE, Higgins LD (2010) Comparison of plain radiography, computed tomography, and magnetic resonance imaging in the evaluation of bone tunnel widening after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 18(8):1059–1064
Moisala AS, Jarvela T, Paakkala A, Paakkala T, Kannus P, Järvinen M (2008) Comparison of the bioabsorbable and metal screw fixation after ACL reconstruction with a hamstring autograft in MRI and clinical outcome: a prospective randomized study. Knee Surg Sports Traumatol Arthrosc 16(12):1080–1086
Pereira H, Correlo VM, Silva-Correia J, Oliveira JM, Reis RL, Espregueira-Mendes J (2013) Migration of “bioabsorbable” screws in ACL repair. How much do we know? A systematic review. Knee Surg Sports Traumatol Arthrosc 21(4):986–994
Petre BM, Smith SD, Jansson KS, de Meijer PP, Hackett TR, LaPrade RF, Wijdicks CA (2013) Femoral cortical fixation devices for soft tissue anterior cruciate ligament reconstruction: a comparative biomechanical study. Am J Sports Med 41(2):416–422
Sabat D, Kundu K, Arora S, Kumar V (2011) Tunnel widening after anterior cruciate ligament reconstruction: a prospective randomized computed tomography-based study comparing 2 different femoral fixation methods for hamstring graft. Arthroscopy 27:776–783
Segawa H, Omori G, Tomita S, Koga Y (2001) Bone tunnel enlargement after anterior cruciate ligament reconstruction using hamstring tendons. Knee Surg Sports Traumatol Arthroscopy 9:206–210
Steiner ME, Hecker AT, Brown CH, Hayes WC (1994) Anterior cruciate ligament graft fixation: comparison of hamstring and patellar tendon grafts. Am J Sports Med 22:240–246
Stener S, Ejerhed L, Sernet N, Laxdal G, Rostgard-Christensen Kartus J (2010) A long-term, prospective, randomized study comparing biodegradable and metal interference screw in anterior cruciate ligament reconstruction surgery: radiographic results and clinical outcome. Am J Sports Med 38:1598
To JT, Howell SM, Hull ML (1999) Contributions of femoral fixation methods to the stiffness of ACL replacements at implantation. Arthroscopy 15:379–387
Webster KE, Feller JA, Hameister KA (2001) Bone tunnel enlargement following ACL reconstruction: a randomized comparison of hamstring and patellar tendon grafts with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc 9:86–91
Wilson TC, Kantaras A, Atay A, Johnson DC (2004) Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med 32(2):543–549
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Lopes, O.V., de Freitas Spinelli, L., Leite, L.H.C. et al. Femoral tunnel enlargement after anterior cruciate ligament reconstruction using RigidFix compared with extracortical fixation. Knee Surg Sports Traumatol Arthrosc 25, 1591–1597 (2017). https://doi.org/10.1007/s00167-015-3888-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3888-x