
Abstract
Purpose
The aim of this study was to make a comparison between players in two age groups in an elite male soccer team regarding injury localisation within the muscle–tendon unit, injury size and muscle group in terms of muscle injuries of the lower extremity.
Methods
Cohort study based on data collected from a Swedish elite male soccer team during the seasons 2007–2012. In total, 145 muscle injuries were included. Injury localisation to the tendon or muscle, the size of haematoma and the affected muscle group were assessed using ultrasound. Age comparison was made between younger players (≤23 years) and older players (>23 years).
Results
No difference regarding injury localisation to either the tendon or the muscle, or the size of haematoma between the two age groups was found. However, the older group of players suffered a significantly higher number of injuries to the triceps surae than the younger players (p = 0.012).
Conclusions
In a Swedish team of male soccer players at elite level, there was no difference between players 23 years or younger and players older than 23 years, in terms of injury distribution to muscles or tendons. Players older than 23 years sustained more injuries to triceps surae when compared with players 23 years or younger. The clinical relevance is to pay attention to muscle function of triceps surae in older players and to screen those players who may need an injury prevention programme.
Level of evidence
II.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In Sweden soccer is the sport that attracts the highest number of athletes. Since soccer is characterised as a high-intensity contact sport, it may, unfortunately, result in a broad variety of injuries. Soccer injuries can be subdivided into different types according to the consensus statement of injury definitions and data collection procedures in studies of soccer injuries [9]. The main injury groups according to the consensus statement are fractures and bone stress, joint and ligament injuries, muscle and tendon injuries, contusions, lacerations and skin lesions, injuries to the central/peripheral nervous system and other injuries. Injuries can be further divided into categories of the main groups [9].
In a recent seven-season follow-up study of male professional soccer players, the injury incidence was reported to be eight injuries per 1,000 player hours [6]. The study also reported that 35 % of the injuries were muscle strains, followed by ligament injuries (18 %) and haematoma due to contusions (17 %) [6]. Ninety-two per cent of the muscle injuries occurred in the major muscle groups of the lower extremities, the hamstrings being involved in 37 %, the adductors in 23 %, the quadriceps in 17 % and the calf muscles in 13 % of the cases [7].
Muscle injuries can be classified into four different grades, based on ultrasonography (US) examinations according to the Peetrons classification system [13]. Grade 0 injuries are not visible on US. Grade I injuries correspond to a minimal elongation of the injured muscle, with less than 5 % of the muscle involved. Grade II injuries consist of partial muscle ruptures involving 5–50 % of the muscle volume or cross-sectional diameter. A hypoechoic gap within the muscle fibres is visible with US of grade II injuries. Grade III injuries are complete muscle tears with retraction of the muscle [13].
According to the “consensus statement of injury definitions and data collection procedures in studies of soccer injuries”, the muscle and tendon injury group can be subcategorized into muscle ruptures, tears, strains, cramps, tendon injuries, tendon ruptures, tendinosis and bursitis [9].
In the clinical setting, US is easily accessible and relatively inexpensive, and therefore, often used as the first choice of diagnostic imaging [1, 11]. Diagnostic imaging is often used to verify a muscle injury. However, recently Ekstrand et al. [8] reported that 13 % of hamstring strains in professional soccer players could not be detected with magnetic resonance imaging (MRI). The reason for this is unknown, though. One explanation may be that minor injuries were not detectable with MRI or that some injuries that clinically appeared to be hamstring strains were caused by neural tension or back problems.
Hitherto, only few studies have compared muscle injuries in different age groups. In some studies, it has been suggested that older soccer players are more prone to muscle injuries than younger players [1, 7]. A study on Australian football players reported that players above 23 years of age had an increased injury risk of hamstrings and triceps surae in comparison with players 23 years or younger [11]. However, no difference in relative risk was found for quadriceps strains between the two age groups [12]. Furthermore, it is unclear whether the injury localisation within the muscle–tendon unit differs between age groups. Hitherto, knowledge of the relationship between age and injury localisation within the muscle–tendon unit in soccer players is still lacking.
Since an elite soccer team often consists of players of different ages, it is valuable to find out whether age plays any role as a risk factor for muscle injuries. Therefore, the aim of the present study was to make a comparison between a young and an older age group of elite male soccer players regarding the localisation and the severity of muscle injuries of the lower extremity.
Materials and methods
The present investigation is a cohort study based on prospective data collected from a Swedish elite male soccer team during six seasons (2007–2012). During these years, a total of 178 players were included in the senior squad. US examinations were performed 209 times and out of these, 64 injuries were excluded and 145 muscle injuries of the lower extremity were included in the data analysis. Based on their age, these players were divided into two groups, players ≤23 years and players >23 years. The player’s height, weight and BMI of both age groups are shown in Table 1.
Inclusion/exclusion criteria
Included in this study were all muscle injuries suffered by players from the senior squad of an elite male soccer team during training or match. A muscle injury was defined as a traumatic injury to the muscle leading to inability to fully participate in training or match. To be included an injury also had to be examined with US. In total, 209 US reports were retrieved from the injured player’s medical charts. Re-injures, injuries not affecting the lower extremity and other injuries than muscle injuries were excluded. In addition, muscle injuries referred to another US examination in order to check their degree of healing were also excluded. A re-injury was defined as an injury to a previously injured muscle group within the same year of the first injury. This was in line with the consensus statement on injury definitions in professional soccer [8]. After exclusion, 145 reports of muscle injuries diagnosed with US remained for statistical analysis.
A physiotherapist with more than 20 years experience of being a team physiotherapist for high division football players was responsible for collecting and reporting all injuries.
The injuries were categorised as predominantly affecting the tendon or the muscle according to the US reports. The injuries were also categorised based on which muscle group was injured. The four muscle groups included were the hamstrings, the quadriceps, the hip adductors and the triceps surae. The size of the haematomas and/or oedema was retrieved from the US reports. Using US, cross-sectional length and width as well as the longitudinal length of the haematomas/oedema were compared. Injuries or complaints/pain that could not be seen with US were included in the statistical analysis and given the value 0. The two age groups consisted of players 23 years or younger (n = 38) and players older than 23 years (n = 26). This dividing of age groups in players ≤23 years and players >23 years was chosen based on a previous study of Australian football players [23]. Comparative analyses between the young and the older age groups, regarding injury localisation within the muscle–tendon unit, size of the injury/haematoma and injury distribution were executed.
Ultrasonography
Whenever a player sustained an acute muscle injury during training or match, he was referred to a radiologist for US examination.
The use of US was the method of choice due to the fact that it was more easily accessible and inexpensive when compared with MRI. Fortunately, the US examinations were performed by an experienced radiologist who strengthens that the analyses of the pictures were well performed and thereby comparable to MRI in the acute setting [3]. The intra-examiner variability for US examinations on tendon and muscle dimensions has been documented [5]. For an experienced operator, the intra-class correlation coefficient (ICC) ranged from 0.86 (patellar tendon) to 0.99 (vastus lateralis) [5]. These high ICC values can be considered good and indicate that US performed by an experienced radiologist is sufficiently reliable to use in a study of muscle and tendon injuries.
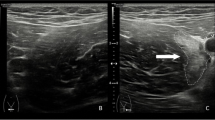
The US imaging was performed using Mylab 70 Xvision ESAOTE (Florence, Italy). The area of maximal tenderness was palpated in order to locate the site of injury. The imaging was executed in two planes transversely related to the muscle fibres and longitudinally in the long axis of the muscles, using a linear high-frequency transducer. When a player suffered a muscle injury, a standardised referral to the radiologist was sent within 1–3 days. The player then underwent diagnostic US within 2–7 days of the injury. All the investigations were performed by the same experienced radiologist, who investigated the cross-sectional length, cross-sectional width and longitudinal length of the haematoma. A haematoma was identified on the basis of the presence of an area of increased echogenicity with or without muscle fibre disruption. The radiologist also examined which muscles were affected and whether the injury primarily affected the muscle or the tendon. A comparison between the contralateral leg and the injured leg was performed.
The present study was approved by the Regional Ethics Committee at Linköping University, Sweden (Dnr 2010/365-31).
Statistical analyses
Included cases in this investigation were injuries to the quadriceps, hamstrings, hip adductors and the triceps surae. A player could have more than one muscle injury, and therefore a dependence variable could be expected between cases. In the analyses, no regard has been taken to this fact, which implies that the significance of the differences between groups can be somewhat overestimated.
Data from all variables were summarised using standard descriptive statistics such as frequency, mean and standard deviation, median and range. The differences between age groups (muscle versus age group) and the analysis of character of the injury (muscle or tendon) and age were analysed with Pearson’s χ2 (Chi-square) method. As the sample size was small for some of the muscle groups, Fisher’s exact test was also used. The analysis of the relationship between the extent of the injury (cross-sectional length, cross-sectional width and longitudinal length) and age was performed for the separate measures. No volume measure was calculated as the coordinates of the size of the injury were not available. The analyses were made by a non-parametric Mann–Whitney U test due to positively skewed distributions when plotting the data in a histogram. The significance level of all analyses was 5 % (two-tailed). The SPSS® version 21.0 (SPSS inc, Chicago, Illinois, USA) software was used for all statistical analyses.
Power analysis
All players during the six seasons were included in the study. A total of 145 injuries were discovered. Age was split into two groups according to the median value, i.e. less or equal to 23 (n = 69) versus above 23 years (n = 76), which leaves a harmonic mean of 72 subjects in each group. The effect size that was possible to detect with a power of 0.80 and a significance level of 0.05 was of almost medium size (0.50) or 0.47 (Cohen 1988). This effect size can be translated to a difference in frequency of injury localisation between the two age groups of 15–25 %, e.g. 10 % in one group and 28 % in the other, depending on the percentages of the groups.

Age-related injury distribution within the MTU, a comparison between soccer players years or younger and soccer players older than 23 years in terms of injuries primarily affecting either the tendons or the muscles. MTU muscle–tendon unit. Asterisk denotes significant difference (p < 0.05, Chi-square test)
Results
The injury incidence during the six seasons (2007–2012) was found to be on an average 14.5 muscle injuries/1,000 h of match play and 3.5 muscle injuries/1,000 h of training. Sixty-four players sustained a total of 145 muscle injuries of the lower extremity (quadriceps, hamstrings, adductors and triceps surae). Out of the 145 injuries, 69 injuries (48 %) occurred in players 23 years or younger and 76 injuries (52 %) in players older than 23 years (Fig. 1). No significant differences of the age groups were found in terms of the number of muscle injuries when it comes to the quadriceps (n.s.), the hamstrings (n.s.) and the adductors (n.s.). For the triceps surae, the players 23 years or younger suffered 8 % of the injuries, and the players older than 23 years suffered 20 % of the injuries (p = 0.012).
There were no significant differences regarding injury localisation within the muscle–tendon unit to either the tendon or muscle, when comparing players 23 years or younger with players older than 23 years. Most injuries occurred in the muscle in both age groups. Injuries to the muscle were found to be 57 % in players ≤23 years and 64 % in players >23 years. Injuries to the tendon were found to be 43 % in players ≤23 years and 36 % in players >23 years. The number of injuries localised in the muscle and tendon is also presented in Fig. 2.

Age and injury, a comparison of muscle injury distribution of the lower extremity between soccer players 23 years or younger and soccer players older than 23 years
No statistically significant group differences were found in terms of haematoma/oedema for any of the three US measured values, cross-sectional length, cross-sectional width and longitudinal length (Table 2; Fig. 3).

Size of haematoma/oedema, a comparison between soccer players 23 years or younger (n = 61) and soccer players older than 23 years (n = 71). The haematoma/oedema was measured in three dimensions represented as cross-sectional length, cross-sectional width and longitudinal length. US ultrasonography, CS cross-sectional, Lt longitudinal
Discussion
The most important finding of the present investigation was that there were no differences between players 23 years or younger and players older than 23 years when it comes to injury localisation within the muscle–tendon unit to either the tendon or the muscle. Furthermore, no difference between age groups was found for the size of the haematoma/oedema determined as cross-sectional length, cross-sectional width and longitudinal length. However, players older than 23 years sustained a higher number of injuries to the triceps surae than the young group of players.
During the six studied seasons, the injury incidence of muscle injuries in soccer players was found to be on an average 14.5 muscle injuries/1,000 h for match play and 3.5 muscle injuries/1,000 h for training. These figures correspond well with those by Ekstrand et al. [7] (4.1 injuries/1,000 h) when it comes to training. However, regarding match play Ekstrand et al. [7] reported an incidence of muscle injuries to be twice as high (27.5 injuries/1,000 h) as those of the present study. It is known that competitive games have a higher injury incidence rate than training sessions [7]. However, a possible explanation for the differences of the size of the injury incidence during match play between the study by Ekstrand et al. [7] and the present study may be due to that their study was carried out during two seasons compared to six seasons in the present investigation. It is not unusual that injury incidence can vary at different seasons, which might depend on a number of factors such as the soccer players of the team at the time, their coaches and training methods, for instance.
No difference was found between players 23 years or younger and players older than 23 years in terms of injury distribution between the large muscle groups of the lower extremity. The older group of players did, however, sustain a significantly higher number of injuries to the triceps surae than the younger players. This finding is consistent with a recent and similar study by Hägglund et al. [10].
However, in contrast to this study, other similar studies have reported an increased risk of hamstring injuries in older players [1, 12]. This inconsistency could be due to differences in the study cohorts. Orchard et al. [12] performed a study on Australian football players, whereas Arnason et al. [1] investigated risk factors in semi-professional soccer players. The semi-professional soccer players might not have had the same resources and knowledge on how to prevent hamstring injuries as the elite players in the present study. The study by Orchard et al. [12] showed a significant difference in relative risk for older players and injuries to both the triceps surae and the hamstring muscles. However, age was not found to be a confounder for the correlation between a previous injury and the risk of sustaining an injury. This is of potential interest and should be taken into account when further analysing the results of the present study. The increased risk of injuries to the triceps surae in the older players may be due to the fact that they had sustained injuries to the triceps surae already before the start of the present study, at least more than 2 months earlier.
When comparing injury localisation within the muscle–tendon unit between the two groups of players, no differences were noted, indicating that elite players irrespective of age are at equal risk of sustaining injuries to the tendons, and/or the muscles. Earlier studies comparing age and injury localisation within the muscle–tendon unit are lacking. Therefore, a direct comparison to other studies is not possible.
In a large study of injury risk factors in the Icelandic first and second league of soccer, the result showed that older players had an increased risk of sustaining injuries in general and hamstring strains in particular [1]. However, in that study, it was not reported whether the strains primarily affected the tendon or the muscle. To the best of our knowledge, the present investigation is the first one studying the relationship between age and injury localisation within the muscle–tendon unit.
In the present study, no difference was found for the size of the haematomas/oedema following injury, when comparing players 23 years or younger and players older than 23 years. We have not found any earlier study investigating the relationship between age and the size of muscle haematoma/oedema. When comparing the present study to other studies investigating the size of muscle injury using US, it should be noted that this study included those injuries that were negative on US in the statistical analysis. This was done since it would lead to a larger and more representative study material. Furthermore, the injuries with haematoma/oedema visible on US and those not visible on US were often similar from a clinical point of view. Because of the inclusion of the injuries that were negative on US the mean cross-sectional length of injury was shorter in the present study than in a study by Connell et al. [3], 5 and 25 mm, respectively. In a study on youth soccer players, a positive relationship was found between increasing age and the time of the rehabilitation after injury [2]. One could speculate that a reason for this finding could be due to that the size of muscle injuries increased with increasing age. The older players in their study (16 years) might have suffered injuries caused by a larger force than the younger players (9–15 years) because of their larger body mass and higher power output. In the present study, the players 23 years or younger and the players older than 23 years were fairly equal in terms of height, body weight and BMI. Moreover, they can be assumed to be fairly equal in strength and power output as well. These similarities and the fact that the two study groups trained and competed together, thus exposing both groups to similar forces, most probably makes the result of the present study realistic and trustworthy.
One of the main strengths of the present investigation is that all US examinations were performed by the same experienced radiologist, thereby eliminating the risk of inter-observer variability. It has been reported that the intra-observer variability is low for an experienced radiologist using US on muscles and tendons [5]. Also, in the acute setting of muscle injuries, US has been found to be as reliable as MRI, if performed by experts [3].
Another strength was the homogenous study cohort with all players coming from the same soccer team and sharing the same coaches and medical staff. However, the conclusions from the study cannot be generalised beyond the scope of the present cohort, in this case male elite soccer players.
The cohort study design was inherently vulnerable to unknown confounding factors. However, in the present study, they were limited by the narrow inclusion of male elite soccer players. Confounding factors might still have affected the results, e.g. previous injuries correlated with age and injury risk.
A study limitation could be that the study sample of 145 injuries might not have been large enough to detect age-related differences due to a type II error. This study can, however, be considered as a pilot study and further studies are needed to make accurate assumptions. Nonetheless, from a clinical point of view, the results are relevant since the study cohort included all players from a Swedish male elite soccer team. This makes it possible for coaches and medical staff in the Swedish elite soccer teams to translate the results of the present study into their teams.
Since many injuries occur at the muscle–tendon unit, it may in some cases be difficult to define whether the muscle or the tendon is injured. This could be another limitation of the present study. However, as the study is not investigating the specific injury incidence of muscle or tendon injuries but rather comparing two subgroups within the same cohort, it is likely that any confounding factor would have affected both subgroups equally much and therefore not affected the results of the comparison.
In the present study, the time from injury to US examination varied between 2 and 7 days, which could be seen as a further limitation. This may lead to inaccurate results, as the haematoma/oedema might have been resorbed more on day 7 than day 2 meaning that those haematomas/oedemas examined shortly after injury are larger than those with a longer period between injury and examination.
To the best of our knowledge, this investigation of muscle injuries in soccer players is the only one evaluating the relationship between age and injury localisation within the muscle–tendon unit. Since the time of healing as well as the treatment may differ, whether the injury is localised in the muscle or the tendon, it is important to be able to determine the site of the injury. Age may also play a role when it comes to tissue healing. Therefore, the clinical relevance of the present study is to pay attention to muscle function of triceps surae in older soccer players. For instance, at the start of the season, the coaches and medical staff can screen those players that due to side-to-side difference in muscle strength may need an injury prevention programme.
Conclusions
In Swedish elite male soccer players, no differences between players 23 years or younger and players older than 23 years were shown in terms of injury localisation within the muscle–tendon unit to muscle or tendon or the size of haematoma/oedema. Muscle injuries of the triceps surae were more commonly found in players older than 23 years when compared with those 23 years or younger.
References
Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R (2004) Risk factors for injuries in football. Am J Sports Med 32(1 Suppl):5S–16S
Cloke D, Moore O, Shah T, Rushton S, Shirley MD, Deehan DJ (2012) Thigh muscle injuries in youth soccer: predictors of recovery. Am J Sports Med 40(2):433–439
Connell DA, Schneider-Kolsky ME, Hoving JL, Malara F, Buchbinder R, Koulouris G, Burke F, Bass C (2004) Longitudinal study comparing sonographic and MRI assessments of acute and healing hamstring injuries. Am J Roentgenol 183(4):975–984
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. Lawrence Erlbaum Ass., Publ, Hillsdale
Dudley-Javoroski S, McMullen T, Borgwardt MR, Peranich LM, Shields RK (2010) Reliability and responsiveness of musculoskeletal ultrasound in subjects with and without spinal cord injury. Ultrasound Med Biol 36(10):1594–1607
Ekstrand J, Hagglund M, Walden M (2011) Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med 39(6):1226–1232
Ekstrand J, Hagglund M, Walden M (2011) Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med 45(7):553–558
Ekstrand J, Healey JC, Walden M, Lee JC, English B, Hägglund M (2012) Hamstring muscle injuries in professional football: the correlation of MRI findings with return to play. Br J Sports Med 46(2):112–117
Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, Hägglund M, McCrory P, Meeuwisse WH (2006) Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Clin J Sport Med 16(2):97–106
Hagglund M, Walden M, Ekstrand J (2013) Risk factors for lower extremity muscle injury in professional soccer: the UEFA Injury Study. Am J Sports Med 41(2):327–335
Megliola A, Eutropi F, Scorzelli A, Gambacorta D, De Marchi A, De Filippo M, Faletti C, Ferrari FS (2006) Ultrasound and magnetic resonance imaging in sports-related muscle injuries. Radiol Med 111(6):836–845
Orchard JW (2001) Intrinsic and extrinsic risk factors for muscle strains in Australian football. Am J Sports Med 29(3):300–303
Peetrons P (2002) Ultrasound of muscles. Eur Radiol 12(1):35–43
Acknowledgments
The Swedish Centre for Sport Research is gratefully acknowledged for financial support.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Svensson, K., Alricsson, M., Karnebäck, G. et al. Muscle injuries of the lower extremity: a comparison between young and old male elite soccer players. Knee Surg Sports Traumatol Arthrosc 24, 2293–2299 (2016). https://doi.org/10.1007/s00167-015-3527-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3527-6