
Abstract
Purpose
Since excessive tibial tuberosity–trochlear groove distance (TT–TG) is one of the major risk factors for patellofemoral instability, TT–TG is an often-used parameter in knee realignment surgery. Up to date, TT–TG is measured and interpreted using absolute values, disregarding the knee size of the individual. It was hypothesized that there is a relation between TT–TG and knee size and body height, respectively.
Methods
Consecutive MRI scans of 120 knee joints were analysed retrospectively. Of these, 60 MRI scans were obtained from patients with trochlear dysplasia and another 60 MRI scans were acquired from patients presenting with a different pathology of the knee joint. TT–TG was measured and TD was classified into low and high grade. Interepicondylar distance as an expression of knee size was measured on transverse MRI slices presenting the maximal distance from the medial to the lateral epicondylus. TT–TG was correlated with interepicondylar distance and body height.
Results
Interepicondylar distance as an expression of knee size correlated highly with body height in the control group with normal trochlea (r = 0.78) as well as in the TD group (r = 0.69). Correlation of TT–TG with interepicondylar distance or body height in the control group as well as in the TD group showed poor values with r < 0.30 (range r = 0.072–0.28).
Conclusion
TT–TG seems associated neither with the size of the individual knee, nor with body height. For this reason, TT–TG has to be considered as very individual parameter in knee realignment surgery.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The tibial tuberosity–trochlear groove distance (TT–TG) is a widely used parameter in the assessment of patellofemoral disorders [6]. Regarding patellofemoral instability (PFI), excessive TT–TG is considered as one of the major risk factors. The TT–TG characterizes the lateralisation of the tibial tuberosity or, in case of trochlear dysplasia (TD), the medialization of the trochlear groove. The relevance of the TT–TG in clinical practice is underlined by the fact that the parameter is used as a decision-making criterion in realignment surgery of the knee [8, 14]. In 1994, Dejour et al. [4] found a markedly increased TT–TG in patients with symptomatic patellar instability, characterized by dislocation of the patella, which comprised a total loss of the contact between the articular surfaces of patella and trochlea. Using axial CT scans, the authors found that a mean TT–TG of 20 millimetres (mm) in patients with a history of PFI was 19.8 ± 1.6 mm, while the TT–TG in the control group was 12.7 ± 3.4 mm.
At present, MRI is considered as an equivalent imaging method. Dejour’s findings were confirmed in 2000 by McNally et al. [9]. The authors detected a TT–TG of more than 20 mm in patients with severe patellofemoral maltracking in MRI imaging. A TT–TG of 20 mm has frequently been used as a cut-off value to direct surgical treatment. Besides this, almost all scientific work concerning the measurement and the interpretation of TT–TG discusses absolute values, disregarding the knee sizes of the individual. However, it appears intuitive to assume smaller thresholds for the TT–TG in smaller knee joints.
It was hypothesized that there is a relation between TT–TG and the size of the knee joint, meaning that small persons with small knees have smaller TT–TG and vice versa for tall persons.
The aim was to establish a non-dimensional ratio between TT–TG and knee size in order to be able to assess the TT–TG depending on the individual knee size, especially in knee joints presenting with TD.
Materials and methods
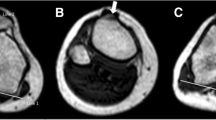
A total of 120 MRI scans of knee joints from patients presented to our hospital were analysed retrospectively. Of these, 60 consecutive MRI scans were obtained from patients with TD [60 patients: 27 males and 33 females; mean age 23 years (17–48 years); 33 scans of left knees and 27 scans of right knees]. All of the patients with TD presented to our hospital suffered from symptomatic PFI (at least one patellofemoral dislocation). There was no severe injury to the trochlear cartilage or major bony contusion of the trochlea leading to the deformation of the trochlear groove. TD was classified into low-grade and high-grade dysplasia, based on the classification system described by Dejour et al. [3]. Therefore, all transversal MRI scans were read together with sagittal plane radiographs of the knee: with the presence of a crossing sign in the sagittal radiograph and a shallow but still concave trochlea in the MRI scan, TD type A was assessed. With additional trochlear spur in the sagittal radiograph and a flat trochlea in the MRI scan, TD type B was assessed. With the presence of a crossing sign and a double-contour sign (hypoplastic medial facet) in the sagittal radiograph and a convexly shaped lateral trochlear facet, TD type C was assessed. With the combination of all above-mentioned characteristics in the radiograph and a clear asymmetry of the height of the facets (“cliff pattern”), TD type D was assessed.
TD Dejour type A and B were defined low grade and Dejour type C and D high grade, respectively (Fig. 1). No patient presenting with TD underwent distal realignment procedures or deepening trochleoplasty prior to MRI.

Assessment of the severity of trochlear dysplasia, using the classification system described by Dejour et al. After synopsis of the axial MRI slice with a true lateral radiograph, the example depicts several features of type D trochlear dysplasia: cliff pattern on the MRI scan (1) combined with the crossing sign (2), supratrochlear spur (3) and double-contour sign (4) on the radiograph
Another 60 consecutive MRI scans were obtained from patients presenting with a different pathology of the knee joint [e.g. lesion of the meniscus, tear of anterior cruciate ligament; 59 patients: 36 males and 23 females; mean 43 years (span 18–68 years), 34 scans of left knees and 26 scans of right knees]. In this subgroup, patients with patellofemoral complaints or anterior knee pain were excluded.
Imaging
MRI was performed with the patient in supine position on a 1.5-T unit (VA17A-Symphony A Tim System, Siemens, Germany). During the MRI scans, the knee joints were fully extended [5, 7]. The scans were obtained in fat-saturated proton density-weighted fast spin-echo imaging sequence under standardized conditions.
For the assessment of TD, the transverse MRI scans were acquired at the most proximal craniocaudal transverse slice on which the cartilage along the entire width of the trochlea was visible.
In all MRI scans, the TT–TG was measured according to the method described by Schoettle et al [12]:
The first transverse slice that depicted a complete attachment of the patellar tendon slightly cranial the tuberositas tibiae was used. In order to determine the mid-point of the patellar tendon insertion, a line was drawn connecting the medial and lateral insertion points. A vertical line was set at its centre. In order to define the deepest point within the trochlear groove, again the first craniocaudal transverse slice that depicted complete cartilaginous trochlea was used. Perpendicular lines to a tangent to the posterior femoral condyles were drawn through the mid-point of the patellar tendon and the cartilaginous trochlear groove, and the TT–TG was determined in millimetres.
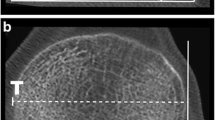
In order to assess the individual size of the knee joint, the interepicondylar distance (IED) was assessed. IED was measured on the transverse MRI slice presenting the maximal distance from the medial to the lateral epicondylus. The distance was expressed in millimetres (Fig. 2).

a Determination of the mid-point of the patellar tendon insertion: the first slice with complete attachment of the patellar tendon cranial to the tuberositas tibiae was used. A line between the most external insertion points was drawn with a vertical line at its center. b For the definition of the deepest point within the trochlear groove the first craniocaudal transverse slice with complete cartilaginous trochlea was used. On the slice with the maximal distance from the medial to the lateral epicondylus IED was measured. c TT–TG was defined as the distance between the mid-point of the patellar tendon to the cartilaginous trochlear groove perpendicular to a tangent to the posterior femoral condyles
All values of TT–TG and IED were acquired by two observers. Both observers were experienced in knee realignment surgery.
The measurements were performed with GE Centricity PACS-IW (General Electric Company, Connecticut, USA). This imaging software allowed measurement accuracy with one decimal.
Body height was obtained from patient charts. IED was correlated with body height to prove the validity of the parameter.
Statistical analysis
Subsequently, TT–TG was related to IED in dividing the values of TT–TG (in mm) by the values of IED (in mm) (TT–TG/IED × 100 %), and results were defined as TT–TG ratio (in %).
For the values of TT–TG and IED, interobserver correlation and intraobserver correlation were calculated using intraclass correlation coefficient (ICC).
Standard error of measurement (SEM) was calculated [SEM = SD × √(1 − r)].
Correlation of TT–TG to IED as well as to body height was expressed using Pearson’s correlation coefficient. In addition, the variation coefficient (relative standard deviation) was determined for TT–TG and TT–TG ratio in order to express the distribution of the values. When p values exceeded 0.05, power analysis was performed using G*Power Version 3.1.9.2. Post hoc power analysis (effect size 0.6; α = 0.05) for the control group (n = 60) and the TD group (n = 60) resulted in 0.89 (1-β err prob). Statistical analysis was performed with SAS statistical software version 9.2 (SAS institute, North Carolina, USA).
The IRB approval was given by the ethical committee of the University of Ulm, ID 305/13b.
Results
The anthropometric data (body height, TT–TG, IED, TT–TG ratio) are provided in Table 1. IED as an expression of knee size correlated highly with body height in the control group with normal trochlea (r = 0.78) as well as in the TD group (r = 0.69).
The values of the readings of IED showed excellent intra- and interobserver correlation in the control group and in TD group (range r = 0.97–0.99; SEM: 0.70–1.03).
For the readings of TT–TG in the control group, interobserver correlation and intraobserver correlation were excellent (r = 0.92; SEM: 1.01 and r = 0.97; SEM: 0.62, respectively).
Regarding the values of TT–TG in the scans with low-grade TD, excellent interobserver correlation (r = 0.93; SEM: 1.01) and intraobserver correlation (r = 0.95; SEM: 0.88) were found. For the scans with high-grade TD, good interobserver correlation (r = 0.84; SEM: 1.06) and good intraobserver correlation (r = 0.84; SEM: 1.06) were found. All above-mentioned intra- and intercorrelation readings were statistically significant (p < 0.05).
Correlation of TT–TG with IED or body height in the control group as well as in the TD group showed values of r < 0.30 (range r = 0.072–0.28) [Fig. 3]. Except the correlation of TT–TG in the TD group with the body height in the TD group (p < 0.05), p values exceeded 0.05 (range p = 0.108–0.583).

a, b Correlation of TT–TG with IED or body height in the control group as well as in the TD was poor (values of r < 0.30)
Variation coefficient for TT–TG ratio was 0.35 in the control group with normal trochlea, 0.29 in low-grade TD and 0.14 in high-grade TD [Table 1].
Discussion
The most important finding in this study was that TT–TG in scans of knee joints with normal and dysplastic trochlea did correlate neither with body height nor with knee size. Initially, the aim of this examination was to establish a so-called non-dimensional TT–TG ratio, describing a TT–TG dependent on individual knee size, especially for knee joints presenting with TD. We hypothesized that TT–TG relates to knee size or body height, meaning that small persons with small knees have smaller TT–TG and vice versa for tall persons. This hypothesis had to be rejected.
In clinical practice, the TT–TG is used as a decision-making support in realignment surgery of the knee [4, 8, 14]. In the current literature, absolute values for pathological TT–TG are still discussed, assuming a threshold at 15 mm or 20 mm, regardless of the size of the knee joint of the individual [4, 8]. In this context, the authors of the present study felt that the TT–TG should be interpreted depending on knee size.
Prior to this, an objective parameter in knee MRI correlating with the individual body height was required. We chose IED as objective parameter as it is measurable reproducibly in transverse MRI slices. In this study, IED correlated highly with body height. This finding allowed the assumption that body height was represented well by IED. Excellent reproducibility of the values of TT–TG and IED was confirmed by intra- and interobserver correlation in normal knees and in the knees with low-grade TD. For the measurement of TT–TG in high-grade TD, we found slightly reduced inter- and intraobserver correlation, owing to the fact that the deepest point in the trochlear groove is difficult to define with a flat or dome-shaped trochlea.
In this study, the mean TT–TG for normal knees averaged 10.4 mm (SD 3.6 mm) and for knees with PFI 15.8 mm (SD 4.6 mm). These values are comparable to the values described in the current literature [1, 2, 10–12, 15].
Contrary to expectations, correlation of TT–TG with knee size (IED) and with body height showed interaction neither in the control group nor in the TD group. These findings indicate that the geometry of the knee joint seems to be too unique to establish a relation of TT–TG to morphometric aspects of the knee, at least in axial plane MRI.
However, we found a decreasing variation coefficient for the values of TT–TG ratio with increasing severity of TD (Table 1). This means that the values of TT–TG normalized to knee size show less spread when TD increases. Looking at it the other way round, TT–TG ratio shows the most variation in knees with normal trochlea.
Balcarek et al. approached this issue with a similar intention. The authors aimed at diminishing the effect of size in the relatively smaller-boned knees of children and adolescents and related to the TT–TG with the total width of the distal femur. They found a difference in their so-called relative TT–TG distance (comparable to the TT–TG ratio in our examination) between the normal group and their study group, but no significant interaction of TT–TG with femur width [1].
Recently, Pennock et al. [11] investigated the relation of TT–TG to body height and femoral width. The authors rose to question whether an absolute value of TT–TG can be applied to all patients, especially when anthropometric measurements vary dramatically. In their patient cohort, patients’ height varied from 139 to 196 cm. Their data showed that TT–TG is associated with patient height, but femoral width did not affect TT–TG measurement.
In this examination, the results were similar: TT–TG ratio for the knee joints without PFI was calculated 12.7 % and for the knee joints with PFI 20.1 %. Balcarek et al. found that TT–TG ratio for the knee joints without and with PFI was 15 and 22 % and Pennock et al. 13.8 and 18.8 %, respectively [1, 11]. The aforementioned authors particularly investigated the values of TT–TG in the young patient. Some of the patients with PFI in the work of Balcarek were younger than 10 years (mean 21.6, SD 7.9 years], and the patients’ age in the work of Pennock averaged 15.4 years (range 10–18 years). Pennock et al. demonstrated that the TT–TG varies modestly as a function of body height. In their cohort, patients’ age ranged from 10 to 18 years and body height from 139 to 196 cm. Due to this relatively wide range of body height, discrimination of small TT–TG in smaller persons to large TT–TG in bigger persons seems to be statistically representable.
In the cohort of this examination, all included patients of the control group and TD group had reached skeletal maturity, and the growth plates around the knee joint were closed. The body height of our patients ranged from 155 to 193 cm. In the control group, patients’ height ranged from 150 to 193 cm. In the present study, patients’ morphometric data (body height, IED) did not significantly correlate with TT–TG.
There are analogous situations in knee surgery, for example, in anterior cruciate ligament (ACL) surgery. Shelbourne and Kerr showed that there was no correlation between body height or weight and femoral notch width. The authors concluded that body size could not be used as a predictor of notch width [13].
Several limitations deserve mention. Our control group was not completely asymptomatic. The MRI scans in these patients were performed because of meniscal tears, rupture of anterior cruciate ligament or cartilage lesion. Furthermore, observers could not be blinded as to whether the MRI scans had been obtained in control patients or in patients with TD, because in the latter group morphologic findings were clearly apparent. Another limitation is the relatively low number of MRI scans with high-grade TD. Thus, statistical power might be affected in this subgroup. In the subgroup of high-grade TD, the measurement of TT–TG was prone to slight imprecision due to the dome-shaped trochlea.
In clinical practice, TT–TG has to be regarded as a distinct parameter, independent of knee size or body height. Irrespective of the presence of TD or its severity, the values of TT–TG seem not related to the size of the knee. In a run-up to a surgical procedure aiming at patellofemoral instability, the size of the knee should not influence the interpretation of TT–TG.
Conclusion
First, interepicondylar distance correlates with body height and so can be used as a proxy for the size of the knee. Second, in patients with mature skeleton and in knee joints with and without TD, TT–TG seems associated neither with the size of the individual knee, nor with body height. For this reason, TT–TG has to be considered as very individual parameter in knee realignment surgery.
References
Balcarek P, Jung K, Frosch KH, Stürmer KM (2011) Value of the tibial tuberosity-trochlear groove distance in patellar instability in the young athlete. Am J Sports Med 39(8):1756–1761
Camp CL, Stuart MJ, Krych AJ, Levy BA, Bond JR, Collins MS, Dahm DL (2013) CT and MRI measurements of tibial tubercle-trochlear groove distances are not equivalent in patients with patellar instability. Am J Sports Med 41(8):1835–1840
Dejour D, Saggin P (2010) The sulcus deepening trochleoplasty—the Lyon’s procedure. Int Orthop 34(2):311–316
Dejour H, Walch G, Nove-Josserand L, Guier CH (1994) Factors of patellar instability: an anatomic radiographic study. Knee Surg Sports Traumatol Arthrosc 2:19–26
Dietrich TJ, Betz M, Pfirrmann CW, Koch PP, Fucentese SF (2014) End-stage extension and its influence on the tibial tuberosity-trochlear groove distance (TTTG) in asymptomatic volunteers. Knee Surg Sports Traumatol Arthrosc 22(1):214–218
Goutallier D, Bernageau J, Lecudonnec B (1978) The measurement of the tibial tuberosity-patella groove distanced technique and results (author’s transl). Rev Chir Orthop Reparatrice Appar Mot 64(5):423–428
Izadpanah K, Weitzel E, Vicari M, Hennig J, Weigel M, Suedkamp NP, Niemeyer P (2014) Influence of knee flexion angle and weight bearing on the tibial-tuberosity-trochlear groove (TTTG) distance for evaluation of patellofemoral alignment. Knee Surg Sports Traumatol Arthrosc 22(11):2655–2661
Koeter S, Diks MJF, Anderson PG, Wymenga AB (2007) A modified tibial tubercle osteotomy for patellar maltracking. J Bone Joint Surg Br 89(2):180–185
McNally EG, Osterle SJ, Pal C (2000) Assessment of patellar maltracking using combined static and dynamic MRI. Eur Radiol 10:1051–1055
Pandit S, Frampton C, Stoddart J, Lynskey T (2001) Magnetic resonance imaging assessment of tibial tuberosity-trochlear groove distance: normal values for males and females. Int Orthop 35(12):1799–1803
Pennock AT, Alam M, Bastrom T (2014) Variation in tibial tubercle-trochlear groove measurement as a function of age, sex, size and patellar instability. Am J Sports Med 42(2):389–393
Schoettle PB, Zanetti M, Seifert B, Pfirrmann CW, Fucentese SF, Romero J (2006) The tibial tuberosity-trochlear groove distance; a comparative study between CT and MRI scanning. Knee 13(1):26–31
Shelbourne KD, Kerr B (2001) The relationship of femoral intercondylar notch width to height, weight and sex in patients with intact anterior cruciate ligaments. Am J Knee Surg 14(2):92–96
Tecklenburg K, Feller JA, Whitehead TS, Webster KE, Elzarka A (2010) Outcome of surgery for recurrent patellar dislocation based on the distance of the tibial tuberosity to the trochlear groove. J Bone Joint Surg Br 92(10):1376–1380
Wittstein JR, Bartlett EC, Easterbrook J, Byrd JC (2006) Magnetic resonance imaging evaluation of patellofemoral malalignment. Arthroscopy 22(6):643–649
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Dornacher, D., Reichel, H. & Kappe, T. Does tibial tuberosity–trochlear groove distance (TT–TG) correlate with knee size or body height?. Knee Surg Sports Traumatol Arthrosc 24, 2861–2867 (2016). https://doi.org/10.1007/s00167-015-3526-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3526-7