
Abstract
The KT-1000 is widely accepted as a tool for the instrumented measurement of the antero-posterior (AP) tibial translation. The aim of this study is to compare the data obtained with the KT-1000 in ACL deficient knees with the data obtained using a navigation system during “in vivo” ACL reconstruction procedures and to validate the accuracy of the KT-1000. An ACL reconstruction was performed using computer aided surgical navigation (Orthopilot, B-Braun, Aesculap, Tuttlingen, Germany) in 30 patients. AP laxity measurements were obtained for all patients using KT-1000 arthrometer (in a conscious state and under general anaesthesia) and during surgery using the navigation system, always at 30° of knee flexion. The mean AP translation was 14 ± 4 and 15.6 ± 3.8 mm using the KT-1000 in conscious and under general anaesthesia, respectively (P = 0.02) and 16.1 ± 3.7 mm using navigation. Measurements obtained with the KT-1000 under general anaesthesia were no different from those obtained “in vivo” with the navigation system (P = 0.37). In conclusion this study validates the accuracy of the KT-1000 to exactly calculate AP translation of the tibia, in comparison with the more accurate measurements obtained using a navigation system.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
To address objective knee laxity, instrumented testing devices that promote standard load application and provide instrumented translation measurements have been developed, such as the KT-1000 arthrometer (MedMetric Corp, San Diego, CA) [7, 29]. This device provides antero-posterior (AP) displacement measurements by monitoring the relative motion between two sensor pads, one in contact with the patella and the other in contact with the tibial tubercle. Several studies indicated that patients with ACL deficient knees display significantly greater anterior laxity as measured with the KT-1000 arthrometer in the injured knee when compared to the normal knee [2, 6, 7, 30, 31]. These differences have been consistent whether the patients tested were conscious or unconscious [16]. Today the KT-1000 arthrometer is widely used as a valid measurement tool in clinical situations; however, we know of no studies that have evaluated the accuracy of this device using known displacements.
Recently, computer assisted navigation systems have been developed to make surgery more reproductive and assist the surgeon with ligamentous knee reconstruction and arthroplasty surgery [1, 3, 5, 8, 15, 17, 26]. For knee ligament surgery the navigation systems were initially designed to facilitate placements of the tunnels in ACL reconstruction [8, 9, 12, 19, 25, 26, 28]. Recent advances include the ability to perform navigated knee stability examinations, representing an intriguing addition to the surgeon diagnostic armamentarium. [8, 10, 24, 26]. The advantage of these systems is the ability to precisely quantify 6 degrees of freedom (DoF) kinematics of the knee during standard clinical testing in the operative setting.
The aim of this study is to compare the measurements of AP translation in ACL deficient knees, recorded with the KT-1000, in both a conscious state and under general anaesthesia, and measurements obtained using the navigation system during “in vivo” ACL reconstruction procedures. The hypothesis of the study is that there are no differences between the KT-1000 and navigation to calculate the AP translation of the knee under general anaesthesia.
Methods
The study group consisted of 30 consecutive patients in whom an ACL reconstruction was performed using computer aided surgical navigation (2.0 OrthoPilot ACL navigation system, Orthopilot, B-Braun, Aesculap).
The average age of patients at the time of surgery was 29 years (range 19–39). All patients were male with a history of chronic ACL deficient knee with a mean time interval between injury and surgery of 3 years (range 5 months–6 years).
All patients were evaluated with the KT-1000 arthrometer (MedMetric Corp, San Diego, CA) before surgery in a conscious state and in the operating room under general anaesthesia in an unconscious state.
All ACL reconstruction procedures were performed with the help of a navigation system (2.0 OrthoPilot ACL navigation system, Orthopilot, B-Braun, Aesculap).
The KT-1000 arthrometer was secured to a horizontal platform with its Velcro (VELCRO USA Inc., Manchester, NH) straps to prevent movement of the device. The reference plate was placed under the tibial tubercle pad, and the variable stack of plates was placed under the proximal edge of the patellar pad. Care was taken to ensure that the variable stack contacted the patellar pad at the joint line indicated by the KT-1000 arthrometer. This ensured that the displacements being measured occurred along the intended joint line. The distal tibial contact surface of the KT-1000 arthrometer was elevated so that the proximal tibial pad could rest flat on the reference plate, allowing maximal range of measurement during testing. The difference between the tibial tubercle reference pad and the patellar references pad was set to zero by placing equal stacks of plates (plate position at zero) under the reference pads. The KT-1000 arthrometer was lightly tapped until the indicator settled. The dial was then adjusted to read 0.0 mm.
Displacement was calculated under a manual maximum (MM) load in the injured and in the uninjured knees, always at 30° of knee flexion. All values were expressed in millimetres (mm). The MEDmetric Corporation cites data from Malcom et al. [21, 22] regarding the accuracy and reproducibility of its KT-1000 arthrometer.
Mean and standard deviations for all measurements as well as the side to side (S/S) difference were calculated. The navigation system assists the surgeon to orientate the tunnels and moreover allows the evaluation of the kinematic of the knee, in particular the AP translation of the tibia.
The femoral and tibial transmitters were firmly fixed to the femur and tibia with two K-wires of 2.5 mm of diameter. To enable the computation of the knee, extra-articular landmarks were registered by the system using a straight pointer. Registration of these landmarks is needed to record translation measurements. The extra-articular landmarks included the tibial tuberosity, the anterior edge of the tibia and the medial and lateral points of the tibial plateau. The knee kinematic between 0° and 90° of knee flexion was also registered.
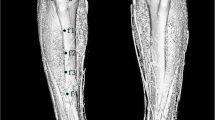
We used the navigation to calculate MM AP tibial translation at 30° of knee flexion (Fig. 1). All values were expressed in millimetres. According to the manufacturer the accuracy of the navigation is estimated to be 0–1 mm. All measurements of KT-1000 and navigation were recorded under a MM force applied by the same Senior Surgeon (A.F.) who performed all surgical procedures to minimise the interobserver variability and who made every effort to apply a similar loading to the knee.

The navigation set-up for AP translation evaluation at 30° of knee flexion
Statistical analysis was performed by statisticians of the Regional Agency of Public Health. All preoperative and intraoperative values of AP displacement of the tibia were recorded in a standard Excel file (Microsoft Office, Microsoft Corporation, USA) and mean and standard deviations were calculated. A 2 (normal knee/ACL disrupted knee) by 2 (conscious/unconscious) by 2 (KT-1000/navigation measurements) analysis of variance (ANOVA) with repeated measures (P < 0.05) was conducted to determine the effect and interactions of those independent variables on the dependent variable of anterior displacement as measured by the KT-1000 arthrometer.
Results
The mean AP displacement of the injured knees, measured by the KT-1000, was 14 ± 4 and 15.6 ± 3.8 mm in a conscious state and under general anaesthesia, respectively.
The mean AP displacement of the uninjured knees, measured by the KT-1000, was 8.5 ± 2.42 and 9 ± 2.32 mm in a conscious state and under general anaesthesia, respectively.
The mean AP displacement, measured by the navigation system under general anaesthesia, was 16.1 ± 3.7 mm. In 15/30 (50%) of cases the value of AP translation calculated by the navigation system was the same as the value calculated with the KT-1000 under general anaesthesia, and in none of the cases was the difference higher than 2 mm.
The mean S/S difference, calculated with the KT-1000 was 8.5 ± 3.1 and 8.5 ± 3.25 mm in a conscious state and under general anaesthesia, respectively. The S/S difference calculated with the KT-1000 in a conscious state was <3 mm in 10% of cases, between 3 and 5 mm in 20% of cases and >5 mm in the other 70% of cases. The S/S difference calculated with the KT-1000 under general anaesthesia was between 3 and 5 mm in 30% of cases and >5 mm in the other 70% of cases.
Values of AP translation calculated with the KT-1000 were significantly higher and different in the injured knee compared to the uninjured knee in both the conscious and unconscious state. Measurements with the KT-1000 under general anaesthesia were significantly higher and different to those obtained in a conscious state (P = 0.02), while they were not different to the measurements obtained “in vivo” with the navigator (P = 0.37).
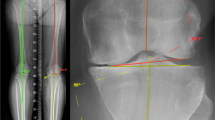
No differences were found in the amount of side to side difference using KT-1000 in a conscious state and under general anaesthesia (P = 0.02). Results are summarised in Fig. 2.

Mean values of AP translation. Statistically significant differences are reported
Discussion
Quantitative systems for the measurements of knee joint laxity have become important additions to the clinical and research practice of orthopaedics [4, 11, 13, 14, 18, 21–23, 32]. Generally four devices, (the Genucom Knee analysis System, the Med Metric KT-1000 Arthrometer, the Stryker Knee Laxity Tester, the Rolimeter) which have been presented in the literature, may be used to clinically assess the amount of knee laxity in an objective manner. These devices can add objective data to the physical examination of the knee. Therefore, the accuracy, reliability and potential sources of measurement errors associated with the use of these devices need to be investigated.
The majority of published reports support the use of ACL laxity measurements obtained from the KT-1000 arthrometer in the diagnosis of ACL disruption [2, 6, 7, 30, 31] because of its accuracy, reproducibility, availability and cost. This device provides AP translation measurement by monitoring the relative motion between two sensors pads in contact with the patella and tibial tubercle [6, 7, 21].
Factors that should be considered in clinical applications of the KT-1000 device include soft tissue compliance, knee positioning and muscle activity. The problem of soft tissue compliance may be minimal, in part because of the subcutaneous position of both the patella and tibia, which are used as contact points with the KT-1000 arthrometer. However, muscle activity is difficult to prevent or to quantify; active quadriceps muscles can decrease posterior translation of the tibia as well as active hamstring muscles which can decrease anterior translation. Muscle contraction can explain why in our study results of AP translation recorded with the KT-1000 are significantly higher under general anaesthesia than in a conscious condition, in agreement with previous similar studies [16]. However, we found no differences in the amount of side to side difference using KT-1000 between the conscious state and under general anaesthesia so we can conclude that the standard KT-1000 evaluation, as well as the Lachman test, should report paired differences rather than individual knee measurements, as is well known.
The KT-1000 measures displacements of the tibial tubercle relative to the patella rather than making direct measurements from the tibia at the joint line, while the knee stability examination, calculated with the navigation system, is highly precise and provides real time quantitative multiplanar data and informative 3D visualisation of knee kinematics [8, 10, 24, 26]. Moreover, using transmitters that are strongly fixed in the bone with 2.5 mm diameter K-wires, if surgical pitfalls are minimised or eliminated and landmarks are accurately registered, the navigation system provides kinematic values with an accuracy of 100%, as precise as that of a robotic sensor system [27]. For this reason surgical navigation was applied to the knee stability examination in this scenario to validate the accuracy of KT-1000 arthrometer.
In our study, values of AP translation under general anaesthesia were not different between KT-1000 and navigation system. These results are in agreement with data from Malcom et al. [21, 22] regarding the accuracy and reproducibility of its KT-1000 arthrometer. They reported that the KT-1000 arthrometer has a mean error of 0.39 + 0.25 mm when compared to measurements made by displacement transducers, and 0.16 ± 0.44 mm (correlation coefficient 0.979) when compared to a system using Steinmann pins. In our study the KT-1000 has been tested for accuracy with a navigation system and has been shown to perform well in comparison.
Studies have also demonstrated that the KT-1000 arthrometer provides reproducible results when appropriate practice and test experience have been achieved by the operator, because one must ensure that the displacing force is directed properly and the device in positioned accurately over the joint line [33]. In fact, significant variation in measurements can occur when the anterior directed force is applied off-center and when the device is not aligned with the joint line [20]. Therefore the KT-1000 arthrometer has a great potential for clinic use, but sources of mistakes in measurement must be minimised.
Although sufficient for a statistical analysis the study is limited by the sample size of ten patients, who accepted undergo the navigation, despite the increased morbidity of the procedure, due to the cortical bone fixation of four pins.
Despite some limitation due to the actual control of the forces used to create the AP translation of the tibia, as manual test were performed, and intra-observer variability cannot be excluded, the reliability of the navigation in evaluating knee kinematic has been previously well documented [10, 24, 27]. Therefore the navigator system allowed us to obtain in vivo the value of AP displacement to be compared with the KT-1000 value in the same condition under general anaesthesia. Moreover in this study group the method used allowed us to obtain the data by using the same patients thus minimising the variation between patients and increasing the statistical power. On the basis of our results the hypothesis that there are no differences between the KT-1000 and the navigation to calculate the AP translation of the knee under general anaesthesia is confirmed.
Although this study validates the accuracy of the KT-1000 to calculate AP translation of the tibia, authors agree with the position of Sherman et al. [30] who stated “instrumented testing devices are not meant to substitute for a thorough history and physical examination, but rather to supplement and substantiate them”.
References
Anderson KC, Buehler KC, Markel DC (2005) Computer-assisted navigation in total knee arthroplasty: comparison with conventional methods. J Arthroplasty 20(6 Suppl 3):132–138
Bach BR, Warron RF, Flynn WM et al (1990) Arthrometric evaluation of knees that have a torn anterior cruciate ligament. J Bone Joint Surg 72A:1299–1306
Bathis H, Perlick L, Tingart M et al (2004) Alignment in total knee arthroplasty a comparison of computer-assisted surgery with the conventional technique. J Bone Joint Surg Br 86:682–687
Blick SS, Daniel DM, Davis J et al (1989) Kinematics of the quadriceps stabilized anterior cruciate disrupted knee. Trans Orthop Res Soc 14:25
Cossey AJ, Spriggins AJ (2005) The use of computer-assisted surgical navigation to prevent malalignment in unicompartmental knee arthroplasty. J Arthroplasty 20:29–34
Daniel DM, Malcolm LL, Losse G et al (1985) Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg 67A:720–725
Daniel DM, Stone ML, Sachs R et al (1985) Instrumented measurement of anterior knee laxity in patients with acute anterior cruciate ligament disruption. Am J Sports Med 13:401–407
Degenhart M (2004) Computer-navigated ACL reconstruction with the OrthoPilot. Surg Technol Int 12:245–251
Dessenne V, Lavallee S, Julliard R et al (1995) Computer-assisted knee anterior cruciate ligament reconstruction: first clinical tests. J Image Guid Surg 1:59–64
Ferretti A, Monaco E, Labianca L et al (2008) Double-bundle anterior cruciate ligament reconstruction: a computer-assisted orthopaedic surgery study. Am J Sports Med 36(4):760–766
Fleming B, Beynnon B, Erickson A et al (1989) An in vivo comparison of anterior joint laxity and strain in the anteromedial band of the anterior cruciate ligament. Trans Orthop Res Soc 14:326
Fleute M, Lavallee S, Julliard R (1999) Incorporating a statistically based shape model into a system for computer-assisted anterior cruciate ligament surgery. Med Image Anal 3:209–222
Fukubayashi T, Torzilli PA, Sherman MF et al (1982) An in vitro biomechanical evaluation anterior-posterior motion of the knee. J Bone Joint Surg 64A:258–264
Granberry WM, Noble PC, Woods GW et al (1989) The accuracy and reliability of instrumented measurement of knee laxity using the Genucom knee analysis system. Trans Orthop Res Soc 14:211
Haaker RG, Stockheim M, Kamp M et al (2005) Computer-assisted navigation increases precision of component placement in total knee arthroplasty. Clin Orthop Relat Res 433:152–159
Highgenboten CL, Jackson AW, Jansson KA et al (2004) KT-1000 arthrometer: conscious and unconscious test results using 15, 20, and 30 pounds of force. Am J Sports Med 20:450–454
Kim SJ, Macdonald M, Hernandez J et al (2005) Computer-assisted navigation in total knee arthroplasty: improved coronal alignment. J Arthroplasty 20(6 Suppl 3):123–131
King JB, Kumar SJ (1989) The Striker knee arthrometer in clinical practice. Am J Sports Med 17:649–650
Klos TV, Habets RJ, Banks AZ et al (1998) Computer assistance in arthroscopic anterior cruciate ligament reconstruction. Clin Orthop Relat Res 354:65–69
Kowalk DL, Wojtys EM, Disher J et al (1993) Quantitative analysis of the measuring capabilities of the KT-1000 knee ligament arthrometer. Am J Sports Med 21:744–747
Malcolm LL, Daniel DM, Stone ML et al (1985) The measurement of anterior knee laxity after ACL reconstructive surgery. Clin Orthop 196:35–41
Malcolm LL, Daniel DM, Stone ML (1980) Instrumented knee stability measurement technique knee ligament arthrometer, model KT-1000. MedMetric Corp., San Diego
Markolf KL, Kochan A, Amstutz HC (1984) Measurement of knee stiffness and laxity in patients with documented absence of the anterior cruciate ligament. J Bone Joint Surg 66A:242–253
Monaco E, Labianca L, Conteduca F et al (2007) Double bundle or single bundle plus extraarticular tenodesis in ACL reconstruction? A CAOS study. Knee Surg Sports Traumatol Arthrosc 15(10):1168–1174
Moody JE, Nikou C, Picard F et al (2002) Computer-integrated anterior cruciate ligament reconstruction system. J Bone Joint Surge Am 84(Suppl 2):99–101
Muller-Alsbach UW, Staubli AE (2004) Computer-aided ACL reconstruction. Injury 35(Suppl 1):S-A65-7
Pearle AD, Solomn DJ, Wanich T, Moreau-Gaudry A et al (2007) Reliability of navigated knee stability examination a cadaveric evaluation. Am J Sports Med 35:1315–1320
Picard F, DiGioia AM, Moody J et al (2001) Accuracy in tunnel placement for ACL reconstruction comparison of traditional arthroscopic and computer-assisted navigation techniques. Comput Aided Surg 6:279–289
Rangger C, Daniel DM, Stone ML (1993) Diagnosis of an ACL disruption with KT-1000 arthrometer measurements. Knee Surg Sports Traumatol Arthrosc 1:60–66
Sherman OH, Markolf KL, Ferkel RD (1987) Measurements of anterior laxity in normal and anterior cruciate absent knees with two instrumented test devices. Clin Orthop 215:156–161
Steiner ME, Brown C, Zarins B et al (1990) Measurement of anterior-posterior displacement of the knee: a comparison of the results with instrumented devices and with clinical examination. J Bone Joint Surg 72A:1307–1315
Torzilli PA, Greenberg RL, Hood RW et al (1984) Measurement of anterior-posterior motion of the knee in injured patients using a biomechanical stress machine. J Bone Joint Surg 66A:1438–1442
Wroble RR, Van Ginkel LA, Grood ES et al (1990) Repeatability of the KT-1000 arthrometer in a normal population. Am J Sports Med 18:396–399
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Monaco, E., Labianca, L., Maestri, B. et al. Instrumented measurements of knee laxity: KT-1000 versus navigation. Knee Surg Sports Traumatol Arthrosc 17, 617–621 (2009). https://doi.org/10.1007/s00167-009-0724-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-009-0724-1