
Abstract
Background
Bronchoalveolar lavage fluid (BALF) is an important diagnostic source to investigate molecular changes occurring in lung disorders. The objective of this study was to assess and compare the peptidomic profiles of BALF from premature neonates with and without bronchopulmonary dysplasia (BPD).
Methods
Samples were obtained on the 3rd day of life from 34 neonates with gestational age ≤32 weeks. Two pools of samples from patients with and without BPD were analyzed by high performance liquid chromatography. Several differentially expressed peptides were collected and sequenced. Moreover, samples from single donors were analyzed by liquid chromatography-electrospray ionization mass spectrometry to define the molecular mass values of various peptides and to quantify their expression. Levels of some matrix metalloproteinases and their tissue inhibitors were also determined in single samples.
Results
Neonates of the BPD group (N = 16) showed significantly lower mean gestational age and birth weight with respect to the no-BPD group (N = 18; P < 0.0001). Levels of six peptides were significantly higher in BPD patients (P < 0.05). Two of them were identified as the albumin fragments 1–21 (2,428 Da) and 399–406 (956 Da). Levels of matrix metalloproteinase-3 (MMP-3) enzyme probably involved in albumin fragment generation were also significantly higher in the BPD group compared to the no-BPD group (P < 0.05), whereas the levels of tissue inhibitor of metalloproteinases-1 were significantly lower (P < 0.05). Levels of albumin fragments and MMP-3 showed a significant correlation (P < 0.05).
Conclusions
This study shows that proteomic techniques can be applied to investigate the involvement of proteolytic enzymes on the airways of mechanically ventilated premature infants.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bronchoalveolar lavage fluid (BALF) proteome analysis in adults by comparative measuring of protein expression both in normal and pathologic conditions has made an important contribution to better understanding of the molecular mechanisms underlying lung disorders [1–3]. At the moment, more than 100 proteins and derivatives have been identified in adult human BALF by using different proteomic approaches, mainly based on two-dimensional gel electrophoresis (2-DE) coupled to matrix-assisted laser desorption ionization mass spectrometry [4–6]. The proteins identified may be either released locally in the lung by inflammatory or epithelial cells, or derived from the serum by diffusion across the capillary-alveolar barrier. The BALF proteome showed significant alterations in sarcoidosis, idiopathic pulmonary fibrosis, allergic asthma, acute lung injury and chronic obstructive pulmonary disease in adult patients [2, 4–13].
Apart from a previous report regarding surfactant composition [14], proteomic approaches have not yet been reported in the study of acute lung injury of premature neonates suffering from respiratory distress syndrome and subsequent development of bronchopulmonary dysplasia (BPD), which remains the most frequent chronic morbidity afflicting prematurely born infants. This analysis is challenging due to difficulties in specimen collection, low sample volume as well as low peptide and protein concentration [1].
However, the ability to identify peptides differently expressed in the lower airways of preterm infants with BPD as compared with preterm infants without BPD might provide new insight into the molecular mechanisms of disease development.
Therefore, the objective of this study was to compare the peptide profile of BALF of the preterm infants that did not develop BPD with that of newborns developing BPD. The analytical approach was centered on a peptidomic top-down strategy (i.e., detection of naturally occurring peptides and proteins of BALF) carried out by reverse-phase high performance liquid chromatography coupled to electrospray ionization mass spectrometry.
Materials and methods
See the electronic supplementary material for a detailed description of methods.
Study subjects
The study was carried out in the Neonatal Intensive Care Unit (NICU) of the Catholic University of Rome and included 34 premature babies consecutively admitted between January 2006 and January 2007. Neonates with gestational age ≤32 weeks were studied. They were eligible: (1) if they were born in our hospital; (2) if endotracheal intubation was required at birth; (3) if on-going intensive care and mechanical ventilation were required. Newborns with major congenital malformations, prenatal infection (positive blood and/or BALF culture at birth), or infants enrolled in the study but who died before BPD diagnosis was made were all excluded from final analysis. Surfactant (a pig-derived, natural surfactant, Curosurf, Chiesi Farmaceutici, Parma, Italy) was administered to all studied newborns at a dose of 200 mg/kg as soon as possible after birth, always in the neonatal unit. All the babies were ventilated in elective high-frequency oscillatory ventilation modality with Draeger Babylog 8000 plus (Draeger, Lubeck, Germany), as previously described [15], and received ibuprofen therapy if the ductus arteriosus was hemodynamically significant [16]. BPD was defined as the need for supplemental oxygen at 28 days of life and a typical radiographic lung picture [17]. The study protocol and consent forms were approved by the Ethics Committee of the Department of Pediatrics, and the parents gave their informed consent.
We also evaluated the incidence of some clinical outcomes: sepsis (defined as the presence of clinical signs of infection with a positive blood culture), pneumonia (proved by worsening of respiratory status with radiological persistent anomalies and a positive BALF culture), severe intracranial hemorrhage (grade III or IV), necrotizing enterocolitis and surgical ligation of the ductus arteriosus.
Bronchoalveolar lavage procedure, cell count and sample processing
BALF samples were obtained on the 3rd day of life according to a standardized procedure [15].
The flow-chart reported in Fig. 1 clarifies the whole experimental design. After collection, specimens were centrifuged at 1,000g for 3 min. Cells were suspended in 250 μl of 0.9% sodium chloride, and the absolute and differential cell count was obtained by automatic analyzer (Bayer-ADVIA 120, Hematology System) and by spinning 25 μl of suspended cells onto two glass slides using May-Grünwald-Giemsa stain, as previously described [18]. Cell-free supernatants were divided into two approximately equal aliquots. One aliquot was immediately frozen at −80°C without any treatment until its use for the metalloproteinase and TIMP assays described in the following sections. The other aliquot, utilized for peptidomic analysis, was immediately mixed with an acidic solution, 0.2% trifluoroacetic acid (TFA) in 1:1 v/v ratio, centrifuged at 8,000g at 4°C for 5 min and the acidic supernatant stored at −80°C until freeze-dried. The acidic treatment reduced the action of BALF proteases and thus the incidence of artifacts.

Experimental design of the top-down peptidomic study; TFA trifluoroacetic acid, HPLC–ESI-MS high-performance liquid chromatography electrospray ionization mass spectrometer; XIC eXtracted ion current, MEROPS peptidase database
The high performance liquid chromatography electrospray ionization mass spectrometer (HPLC–ESI-MS) analysis and peptide characterization
The freeze-dried acidic supernatants were re-suspended in 300 μl of 0.2% TFA solution before the HPLC analysis; 100 μl of this soluble fraction from each sample was analyzed by HPLC ESI-MS, which identified the molecular mass values of various peptides. After BPD diagnosis and inclusion of each sample in the proper group (either BPD or no BPD group), the eXtracted Ion Current (XIC) peak areas of some peptides were used to perform a statistical analysis, as reported in the following. The low protein concentration of these samples precluded the possibility to characterize peptide sequences both by MS/MS and/or classical automatic Edman sequencing.
After the BPD diagnosis was made, namely after 28 days of life, the still available acidic solutions (ca. 200 μl) of BALF samples from the enrolled subjects were combined into two pools. One pool included the samples of all subjects with BPD diagnosis (BPD pool, N = 16), and the other one included the samples of all those subjects not developing BPD (no-BPD pool, N = 18). The comparison between the preparative chromatographic profiles of the BPD and no-BPD pools identified ten peaks that were higher in the BPD group compared to the no-BPD group. They were collected and freeze dried. A small part of the freeze-dried material was analyzed by HPLC–ESI-MS in order to establish the mass of the peptide(s) present in each peak. In order to verify if the amounts of these ten peptides were statistically different in the two groups, the already recorded HPLC–ESI-MS profiles of the BALF from each subject (N = 34) were analyzed by XIC peak area. Indeed, under the constant general analytical conditions adopted in this study, the integrated XIC peak area can be used as a label-free method for an estimation of relative changes in protein amount between two conditions [19, 20], in our case BPD and no-BPD groups. At the same time, the freeze-dried powders of these ten peaks were submitted to automated Edman sequencing.
BALF matrix metalloproteinases (MMPs) and tissue inhibitors of metalloproteinases (TIMP-s) assays
Primary sequence data were analyzed by BLAST similarity search (Expasy-Swiss-Prot/TrEMBL; http://us.expasy.org), and the enzymes potentially responsible for fragment generation were suggested by consulting the MEROPS peptidase database (http://merops.sanger.ac.uk/). On the basis of MEROPS suggestions, in the absence of a unique commercial array that could measure at the same time all the proteinases of potential interest, the Chemiluminescent Array kit (Human MMP array, Thermo Scientific SearchLight) for the simultaneous measurement of seven metalloproteinases (MMP-1, MMP-2, MMP-3, MMP-8, MMP-9, MMP-10 and MMP-13) and the two tissue inhibitors TIMP-1 and TIMP-2 was chosen for the best cost/efficacy ratio. The results regarding the MMP-3 concentrations were confirmed by a specific sandwich ELISA kit (Biosource- Invitrogen Corporation, Camarillo, CA). The minimum detectable concentration of Hu MMP-3 is <0.1 ng/ml. Intra-assay coefficient of variation was <6.7%. The assay measures total Hu MMP-3 (pro-MMP-3, activated MMP-3 and MMP-3 in complex with TIMP-1 or TIMP-2).
Data treatment and statistical analysis
Quantification of specific peptides was based on the XIC peak area. XIC analysis allows revealing selectively a peptide/protein in the chromatographic profile by extracting the ion current associated to its characteristic multicharged ions. Deconvolution of averaged ESI-MS spectra was automatically performed by using the Bioworks Browser software provided with the Deca XP instrument.
In order to normalize the dilution bias resulting from the BALF collection practice and to obtain epithelial lining fluid (ELF) concentration for the different molecules, including MMPs levels and XIC peak area of different peptides, the urea method was used on each sample (N = 34) according to the following equation: ELF = BALF MMPs concentration (or XIC peak area) × (serum urea/BALF urea) [21] (see Fig. 1).
Categorical variables were compared by using a two-tailed Fisher’s exact test. Testing for differences of continuous variables between groups was accomplished by Mann–Whitney U test for non-parametric data and Student’s t test for parametric data, as appropriate. The statistical software used included Instat (GraphPad PRISM Version 3.02). A P value <0.05 was considered statistically significant. Exact logistic regression, based on permutation resampling, was used to determine the association of BPD and some studied variables. Gestational age and birth weight were entered in the model to account for confounding variables. The results are presented as odds ratios with exact 95% confidence intervals and exact P values. Exact logistic regression was performed with Stata/IC 10.
Results
During the study period, 42 neonates met the entry criteria. Two neonates were excluded for later diagnosis of congenital pneumonia, three babies died before 28 days of life, one baby had a major congenital malformation, and in two cases BALF samples were not analyzed for technical problems. The BALF samples of the remaining 34 neonates were utilized for the study. As reported in Fig. 1, 16 newborns developed BPD (BPD group) and 18 did not (no-BPD group). Table 1 reports baseline characteristics and some outcome variables of these infants. The BPD group had significantly lower gestational age and birth weight compared to the no-BPD group (P < 0.0001). No episodes of early onset sepsis (≤72 h of life) occurred in the studied babies. The incidence of late-onset sepsis (>72 h of life), pneumonia and ductus arteriosus requiring surgical ligation was more represented in the BPD group compared to the no-BPD group, but the difference was not statistically significant (Table 1). No significant differences were found between the two groups for both mean airway pressure and fraction of inspired oxygen (FiO2) at the time of BALF procedure (Table 2). Concerning the BALF cytology, the absolute cell count, the neutrophils and alveolar macrophages absolute number resulted in being higher in the BPD group, although this difference did not reach statistical significance (Table 2).
The top-down peptidomic approach utilized for the analysis of the BALF samples is shown in the flow chart of Fig. 1.
Only the sequence of three (out of ten) peptides collected by preparative HPLC was unambiguously determined (Fig. 2).

Typical HPLC preparative ultraviolet profiles of the two BALF pooled samples of the BPD group (a) and the no-BPD group (b) detected at 214 nm: arrows indicate the retention time (RT) and the primary structure determined for three peptides differentially expressed in the BPD group. NL normalization level, MA measured area, AU arbitrary unit
-
Peptide-1: GEYKFQNA (956.0 ± 0.3 Da)
-
Peptide-2: DAHKSEVAHRFKDLGEENFKA (2428.0 ± 0.5 Da)
-
Peptide-3: VLSPADKTNVKAAWGKVGAHAGEY (2469.3 ± 0.5 Da)
The theoretical masses of these peptides exactly corresponded to the experimental masses determined by HPLC–ESI-MS analysis of the purified peaks. A similarity search carried out with BLAST (Expasy-Swiss-Prot/TrEMBL; http://us.expasy.org) revealed that the first peptide (M 956.0 Da) corresponded to the fragment 399–406 of human serum albumin (Swiss-Prot Code P02768), the second one (M 2,428.0 Da) corresponded to the fragment 1–21 of the same protein, and the third one (M 2,469.3 Da) corresponded to the fragment 1–24 of the α-globin chain of human hemoglobin (Swiss-Prot code P69905). Automated Edman sequencing experiments of the other seven peptides differentially detected in the two pools (Table 3) did not give definitive results due to the scarcity of peptide amount and the presence of other contaminant peptides.
The XIC procedure applied to the HPLC–ESI-MS profiles registered on the BALF from each subject (N = 34) immediately after sample collection allowed performing the quantification of the ten peptides in each sample. Figure 3 shows the application of the XIC procedures for the quantification of fragment 1 and 2 (fragments 399–406 and 1–21 of albumin). To take into account the dilution factor the XIC peak areas were multiplied by the ratio serum/BALF urea [19]. The statistical analysis showed significantly higher levels for six peptides in the BPD group compared to the no-BPD group (P < 0.05) (Table 3): the unknown peptides with masses 1,499.0, 2,022.1, 2,260.6, 5,481.9 Da and the fragments 399–406 and 1–21 of albumin. Quantification of intact albumin did not show significant differences between the two groups (data not reported). The statistical analysis of the other four remaining peptides, α-globin chain fragment 1–24 comprised, showed higher median levels in the BPD group, but the differences were not statistically significant.

Typical BALF HPLC–ESI-MS total ion current profile in the 10.65–21.75 min range is reported (a). b The ion peak of the albumin fragment 1–21 evidenced by eXtracted Ion Current strategy, searching the two- and three-charged ions at 1,215.1 and 810.4 m/z. c The ion peak of the albumin fragment 399–406 evidenced by eXtracted Ion Current strategy, searching the mono- and two-charged ions at 957.0 and 479.0 m/z. The area of the XIC peaks and the retention times (at the peak apex) are reported. RT retention time, NL normalization level, MA measured area
The two albumin fragments originated from a similar Ala↓Leu cleavage at the C-terminus. By consulting the MEROPS peptidase database (http://merops.sanger.ac.uk/), the enzymes potentially responsible for this cleavage were: matrix metalloproteinase-1 (MMP-1), MMP-2, MMP-3, MMP-7, MMP-9, MMP-11, MMP-12, MMP-13, MMP-20, MMP-26, cathepsin N, cathepsin D and cathepsin E.
The results obtained using our Chemiluminescent Array kit showed that MMP-1, MMP-10 and MMP-13 were not detectable in the majority of the samples of both groups. No significant differences were found in the levels of MMP-2, MMP-8 and MMP-9 in the two groups (Table 4), whereas the levels of MMP-3 and tissue inhibitor 1 of MMPs (TIMP-1) were respectively significantly higher and lower in the BPD group compared to the no-BPD patients (P < 0.05, Table 4). TIMP-1 is the specific inhibitor of MMP-9 with overlapping inhibitor effects on other MMPs, including MMP-3. The MMP-9/TIMP-1 ratio was significantly higher in infants who went on to develop BPD compared to the no-BPD subjects (Table 4). Because of the scarcity of BALF samples still available, confirmation by ELISA of the array results were possible only for MMP-3 (P < 0.05, Table 4).
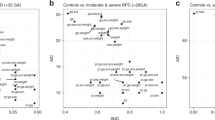
A significant positive correlation between the levels of the two albumin fragments and MMP-3 amounts was found (P < 0.05, Fig. 4). A significant positive correlation between levels of TIMP-1 and MMP-3 was also found (r = 0.39, P = 0.02).

Correlation between levels of MMP-3 and albumin fragment 399–406 (a) and albumin fragment 1–21 (b) in BALF of the studied neonates on day 3 of life. The values of the molecules are corrected by the urea method. The least mean squares regression line is indicated
Exact logistic regression was applied to account for confounding by gestational age or birth weight for the MMP-3 significant difference between the groups. It revealed that both gestational age and MMP-3 are independent significant risk factors for BPD [MMP-3 OR 1.07 95% CI (1.01; + ∞); gestational age OR 0.68 95% CI (0.01–0.96)].
Discussion
Apart from a previous report regarding surfactant composition [14], to our knowledge this is the first study evaluating the peptide content of the BALF from premature neonates by a proteomic approach. In fact, information deriving from the study of only adults patients are actually available [6, 11]. Also these studies reported the presence of different fragments of albumin, although the antibody recognition didn’t allow elucidation of their structure [11]. Fietta et al. [6] found by 2D electrophoresis 13 spots corresponding to serum albumin fragments that are significantly different in two groups of patients suffering from systemic sclerosis with or without functional, clinical and radiological signs of lung fibrosis. Also, these authors were not able to establish the exact molecular weight and the cleavage site of these fragments.
Proteins in BALF may originate from a broad range of sources, such as diffusion from serum across the air–blood barrier (i.e., albumin), secretion from different lung cell types or release from cellular debris. However, the higher concentration of albumin fragments found in the BPD group could not be ascribed to an enhanced diffusion of the albumin molecule from serum because the values observed for the entire protein in the two groups were not significantly different. Until now, a physiological function of albumin fragments is not known. Nevertheless, the two albumin fragments characterized in this study represented a clue to investigate the levels of the enzymes responsible of the specific cleavage. A significantly higher concentration only of MMP-3 was found in BALF of the BPD neonates. Therefore, the higher number of albumin fragments in the BPD group could be ascribed to the greater activity of MMP-3, as also suggested by the significant correlation between albumin fragments and MMP-3 levels. MMP-3, also called transin or stromelysin 1, is a proteoglycanase with a wide range of substrate specificities. It is a secreted metalloproteinase predominantly produced by connective tissue cells and, together with other metalloproteinases, can synergistically degrade the major components of the extra cellular matrix [22]. Nerusu et al. [23] demonstrated that experimental lung injury induced by immunoglobulin G immune complexes is reduced in rodents lacking MMP-3 (MMP-3 −/− mice) as compared to their normal counterparts. The importance of the patho-physiological role of MMP-3 in lung injury is suggested also by a clinical study [24] based on the analysis of BALF samples from adult patients affected by acute respiratory distress syndrome. The overall mortality and disease severity were greater in patients with detectable MMP-1 and MMP-3 than in patients where these enzymes were not-detectable. Another study showed that the protective effect in the lung of MMP-3-deficient mice is associated with a reduction in leukocyte recruitment, suggesting that this protease is involved in neutrophil and macrophage recruitment into sites of inflammation, with possible direct effect on the extracellular matrix [25]. Moreover, a direct role for MMP-3 in the generation of chemotactic activity for leukocytes has been demonstrated in a dinitrofluorobenzene-induced model of contact hypersensitivity [26]. According to the latter observation, the cytology of our BALF samples showed that the absolute number of neutrophils and alveolar macrophages was higher in the BPD neonates compared to the no-BPD group, although this difference did not reach statistical significance (Table 2).
In our experience no significant differences were found between the two groups in terms of other detectable MMPs levels, whereas the amount of TIMP-1 resulted in being significantly higher in the no-BPD group compared to the BPD patients. Finally, the MMP-9/TIMP-1 ratio was significantly higher in infants who went on to develop BPD compared to the no-BPD patients, according to previous studies [27, 28]. It has to be taken into account that some differences exist between our study and previous reports [27–32] evaluating MMPs in the BALF of premature neonates in relation to BPD development. In fact, different postnatal days of sampling, specific techniques used for detecting molecules and finally the different internal markers used for ELF estimation may, at least in part, justify different results.
There are some limitations to our pilot study: (1) we did not collect BALF samples after the 3rd day of life. In fact, most of our patients (25/34 = 73%) were extubated during the 1st week. (2) The number of patients was limited, even if the differences observed were statistically confirmed. (3) A possible confounding effect due to the significantly younger gestational age of the BPD patients might indeed be responsible for higher levels of MMP-3 if this proteinase was developmentally regulated. A gestational age-dependent expression of plasma MMP-2 and MMP-9 activities has been found by Schulz et al. [33], but only in healthy neonates. Until now a correlation between gestational age and MMP-3 has not been reported. However, the employment of the exact logistic regression revealed that the increased MMP-3 levels in our patients are associated with an increased risk of BPD independently of gestational age. (4) The methods employed in this report could only detect the total levels of MMP-3 in BALF, including active enzyme, pro-enzyme and also MMP-3 bound to TIMPs. Therefore, our results do not allow making any conclusion about the net activity of this enzyme in vivo. (5) Other proteinases could be responsible for the albumin cleavage.
In conclusion, this study shows that proteomic techniques can be applied to investigate the involvement of proteolytic enzymes and their cleavage products on the inflammatory milieu that exists in the alveoli and smaller airways of premature infants undergoing mechanical ventilation. We believe that the observations reported in this work may be useful to address future experiments to explore some of the mechanisms involved in the BPD pathogenesis.
Further studies will be necessary to establish the sequence of the other not characterized peptides differently expressed in BPD and no-BPD groups (Table 3) and to define their possible role in the BPD pathogenesis.
References
Waittiez R, Falmagne P (2005) Proteomics of bronchoalveolar lavage fluid. J Chromatogr B Analyt Technol Biomed Life Sci 815:169–178
Bowler RP, Duda B, Chan ED, Enghild JJ, Ware LB, Matthay MA, Duncan MW (2004) Proteomic analysis of pulmonary edema fluid and plasma in patients with acute lung injury. Am J Physiol Lung Cell Mol Physiol 286:L1095–L1104
Hirsch J, Hansen KC, Burlingame AL, Matthay MA (2004) Proteomics: current techniques and potential applications to lung disease. Am J Physiol Lung Cell Mol Physiol 287:L1–L23
Waittiez R, Hermans C, Bernard A, Lesur O, Falmagne P (1999) Human bronchoalveolar lavage fluid: two-dimensional gel electrophoresis, amino acid microsequencing and identification of major proteins. Electrophoresis 20:1634–1645
Waittiez R, Hermans C, Cruyt C, Bernard A, Falmagne P (2000) Human bronchoalveolar lavage fluid protein two dimensional database: study of interstitial lung diseases. Electrophoresis 21:2703–2712
Fietta AM, Bardoni AM, Salvini R, Passadore I, Morosini M, Cavagna L, Codullo V, Pozzi E, Meloni F, Montecucco C (2006) Analysis of bronchoalveolar lavage fluid proteome from systemic sclerosis patients with or without functional, clinical and radiological signs of lung fibrosis. Arthritis Res Ther 8:R160
Noël-Georis I, Bernard A, Falmagne P, Wattiez R (2001) Proteomics as the tool to search for lung disease markers in bronchoalveolar lavage. Dis Markers 17:271–284
Plymoth A, Löfdahl CG, Ekberg-Jansson A, Dahlbäck M, Broberg P, Foster M, Fehniger TE, Marko-Varga G (2007) Protein expression patterns associated with progression of chronic obstructive pulmonary disease in bronchoalveolar lavage of smokers. Clin Chem 53:636–644
Lenz AG, Meyer B, Costabel U, Maier K (1993) Bronchoalveolar lavage fluid proteins in human lung disease: analysis by two-dimensional electrophoresis. Electrophoresis 14:242–244
Lindahl M, Ståhlbom B, Tagesson C (1995) Two-dimensional gel electrophoresis of nasal and bronchoalveolar lavage fluids after occupational exposure. Electrophoresis 16:1199–1204
Lindahl M, Ståhlbom B, Tagesson C (1999) Newly identified proteins in human nasal and bronchoalveolar lavage fluids: potential biomedical and clinical applications. Electrophoresis 20:3670–3676
Magi B, Bini L, Perari MG, Fossi A, Sanchez JC, Hochstrasser D, Paesano S, Raggiaschi R, Santucci A, Pallini V, Rottoli P (2002) Bronchoalveolar lavage fluid protein composition in patients with sarcoidosis and idiopathic pulmonary fibrosis: a two-dimensional electrophoretic study. Electrophoresis 23:3434–3444
Sabounchi-Schütt F, Aström J, Hellman U, Eklund A, Grunewald J (2003) Changes in bronchoalveolar lavage fluid proteins in sarcoidosis: a proteomics approach. Eur Respir J 21:414–420
Ashton MR, Postle AD, Hall MA, Smith SL, Kelly FJ, Normand IC (1992) Phosphatidylcholine composition of endotracheal tube aspirates of neonates and subsequent respiratory disease. Arch Dis Child 67(4 Spec No):378–382
Vento G, Matassa PG, Ameglio F, Capoluongo E, Zecca E, Tortorolo L, Martelli M, Romagnoli C (2005) HFOV in premature neonates: effects on pulmonary mechanics and epithelial lining fluid cytokines. A randomized controlled trial. Intensive Care Med 31:463–470
Su BH, Watanabe T, Shimizu M, Yanagisawa M (1997) Echocardiographic assessment of patent ductus arteriosus shunt flow pattern in premature infants. Arch Dis Child Fetal Neonatal Ed 77:F36–F40
Bancalari E, Claure N (2006) Definitions and diagnostic criteria for bronchopulmonary dysplasia. Semin Perinatol 30:164–170
Vento G, Matassa PG, Zecca E, Tortorolo L, Martelli M, De Carolis MP, Maggio L, Zini G, D’Onofrio G, Valentini S, Romagnoli C (2004) Effect of dexamethasone on tracheobronchial aspirate fluid cytology and pulmonary mechanics in preterm infants. Pharmacology 71:113–119
Inzitari R, Vento G, Capoluongo E, Boccacci S, Fanali C, Cabras T, Romagnoli C, Giardina B, Messana I, Castagnola M (2007) Proteomic analysis of salivary acidic proline-rich proteins in human pre-term and at-term newborns. J Proteome Res 6:1371–1377
Ong SE, Mann M (2005) Mass spectrometry-based proteomics turns quantitative. Nat Chem Biol 1:252–262
Dargaville PA, South M, Vervaart P, McDougall PN (1999) Validity of markers of dilution in small volume lung lavage. Am J Respir Crit Care Med 160:778–784
Sellers A, Murphy G (1981) Collagenolytic enzymes and their naturally occurring inhibitors. Int Rev Connect Tissue Res 9:151–190
Nerusu KC, Warner RL, Bhagavathula N, McClintock SD, Johnson KJ, Varani J (2007) Matrix metalloproteinase-3 (stromelysin-1) in acute inflammatory tissue injury. Exp Mol Pathol 83:169–176
Fligiel SE, Standiford T, Fligiel HM, Tashkin D, Strieter RM, Warner RL, Johnson KJ, Varani J (2006) Matrix metalloproteinases and matrix metalloproteinase inhibitors in acute lung injury. Hum Pathol 37:422–430
Warner RL, Beltran L, Younkin EM, Lewis CS, Weiss SJ, Varani J, Johnson KJ (2001) Role of stromelysin 1 and gelatinase B in experimental acute lung injury. Am J Respir Cell Mol Biol 24:537–544
Wang M, Qin X, Mudgett JS, Ferguson TA, Senior RM, Welgus HG (1999) Matrix metalloproteinase deficiencies affect contact hypersensitivity: stromelysin-1 deficiency prevents the response and gelatinase B deficiency prolongs the response. Proc Natl Acad Sci USA 96:6885–6889
Ekekezie II, Thibeault DW, Simon SD, Norberg M, Merrill JD, Ballard RA, Ballard PL, Truog WE (2004) Low levels of tissue inhibitors of matrix metalloproteinases with a high matrix metalloproteinase-9/tissue inhibitor of metalloproteinase-1 ratio are present in tracheal aspirate fluids of infants who develop CLD. Pediatrics 113:1709–1714
Tambunting F, Beharry KD, Hartleroad J, Waltzman J, Stavitsky Y, Modanlou HD (2005) Increased lung matrix metalloproteinase-9 levels in extremely premature baboons with bronchopulmonary dysplasia. Pediatr Pulmonol 39:5–14
Danan C, Jarreau PH, Franco ML, Dassieu G, Grillon C, Abd Alsamad I, Lafuma C, Harf A, Delacourt C (2002) Gelatinase activities in the airways of premature infants and development of bronchopulmonary dysplasia. Am J Physiol Lung Cell Mol Physiol 283:L1086–L1093
Dik WA, van Kaam AH, Dekker T, Naber BA, Janssen DJ, Kroon AA, Zimmermann LJ, Versnel MA, Lutter R (2006) Early increased level of matrix metalloproteinase-9 in neonates recovering from respiratory distress syndrome. Biol Neonate 89:6–14
Sweet DG, Curley AE, Chesshyre E, Pizzotti J, Wilbourn MS, Halliday HL, Warner JA (2004) The role of matrix metalloproteinases-9 and -2 in development of neonatal chronic lung disease. Acta Paediatr 93:791–796
Cederqvist K, Sorsa T, Tervahartiala T, Maisi P, Reunanen K, Lassus P, Andersson S (2001) Matrix metalloproteinases-2, -8, and -9 and TIMP-2 in tracheal aspirates from preterm infants with respiratory distress. Pediatrics 108:686–692
Schulz CG, Sawicki G, Lemke RP, Roeten BM, Schulz R, Cheung PY (2004) MMP-2 and MMP-9 and their tissue inhibitors in the plasma of preterm and term neonates. Pediatr Res 55:794–801
Acknowledgments
The authors thank the Intensive Care Unit nursing staff for their invaluable collaboration on this work. They also are thankful for the financial support of Università Cattolica in Rome, MIUR, the Italian National Research Council (CNR), Università di Cagliari, Regione Sardegna and thanks fo the Fondazione Banco di Sardegna, International Scientific Institute “Paolo VI” (ISI) for their programs of scientific research promotion and diffusion. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Vento, G., Tirone, C., Lulli, P. et al. Bronchoalveolar lavage fluid peptidomics suggests a possible matrix metalloproteinase-3 role in bronchopulmonary dysplasia. Intensive Care Med 35, 2115–2124 (2009). https://doi.org/10.1007/s00134-009-1646-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-009-1646-6