
Abstract
Objective
To investigate the effect of enteral Synbiotic 2000 FORTE® (a mixture of lactic acid bacteria and fibre) on the incidence of ventilator associated pneumonia (VAP) in critically ill patients.
Design
Prospective, randomised, double blind, placebo controlled trial.
Setting
Tertiary referral centre, general Adult Intensive Care Unit (ICU).
Patients and participants
259 enterally fed patients requiring mechanical ventilation for 48 h or more were enrolled.
Intervention
All patients were enterally fed as per a standard protocol and randomly assigned to receive either synbiotic 2000 FORTE® (twice a day) or a cellulose-based placebo for a maximum of 28 days.
Measurements and results
Treatment group (n = 130) was well matched with placebo group (n = 129) for age (mean 49.5 and 50 years, respectively) and APACHE II score (median 17 for both). Oropharyngeal microbial flora and colonisation rates were unaffected by synbiotics. The overall incidence of VAP was lower than anticipated (11.2%) and no statistical difference was demonstrated between groups receiving synbiotic and placebo in the incidence of VAP (9 and 13%, P = 0.42), VAP rate per 1,000 ventilator days (13 and 14.6, P = 0.91) or hospital mortality (27 and 33%, P = 0.39), respectively.
Conclusions
Enteral administration of Synbiotic 2000 FORTE® has no statistically significant impact on the incidence of VAP in critically ill patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ventilator-associated-pneumonia (VAP) complicates the course of between 8 and 28% of patients receiving mechanical ventilation (MV) in intensive care [1–3]. VAP is associated with a mortality of 10–40%, increased ICU and hospital stay and an estimated cost of US$ 12,000 (€7,500) to US$ 16,000 (€10,000) per episode [3, 4].
Many approaches aimed at VAP prevention have been proposed including head up tilt, selective decontamination of the digestive tract (SDD), chlorhexidine mouthwashes and supraglottic tracheal tube aspiration. An alternative, novel approach may be the use of synbiotics [5]. A synbiotic is a combination of pre- and probiotics [6]. Probiotics are live microbial feed supplements, which affect the host beneficially by improving its intestinal microbial balance. Prebiotics are non-digestible food ingredients that affect the host beneficially by selectively stimulating the growth and/or activity of one or a limited number of bacteria in the colon.
The aetiology of VAP is extremely controversial but appears to be closely correlated with colonisation of the nasopharynx followed by microaspiration into the lung parenchyma [7, 8]. Synbiotics may reduce the incidence of VAP via a combination of local and systemic effects resulting in decreased colonisation. Local effects include reduced overgrowth of potentially pathogenic microorganisms (PPM) by competitive inhibition and direct antimicrobial effects [9, 10]. Secondary systemic benefits may result from improved gut mucosal barrier function, reduced bacterial translocation and upregulation of immune function [11–13]. Evidence supporting this theory is limited, but trials enrolling trauma, neurosurgical, liver transplantation patients and general surgical patients have all demonstrated trends towards a reduction in the incidence of pneumonia [14–17].
The hypothesis tested in this study was whether administration of enteral synbiotics would significantly decrease the incidence of VAP in mechanically ventilated (MV) critically ill patients when compared to placebo. For the purposes of this study, VAP was defined as, pneumonia occurring more than 48 h after endotracheal intubation [2, 18].
Some of the results of these studies have been previously reported in the form of an abstract [19].
Methods
Study location and patients
The study was undertaken between January 2004 and February 2005 in the 14-bedded general ICU of a 1,400-bedded UK tertiary care University hospital. All MV critically ill patients expected to require invasive ventilation for a minimum of 48 h and with no contraindications to enteral nutrition were eligible for the study. The criteria for exclusion was age less than 16 years, active immunosuppression, pregnancy, transfer from other institution (if already intubated for more than 24 h), intubation more than 24 h after admission to ICU and participation in other pharmacological research within the last 30 days. All patients were subjected to standard care protocols with closed suctioning, ranitidine for stress ulcer prophylaxis and a semi-recumbent body position with head elevation of 30° or greater, if possible. Selective decontamination of the digestive tract (SDD), chlorhexidine mouthwashes and continuous aspiration of subglottic contents were not performed in any patient.
The study protocol received full local research and ethics committee approval. Written informed consent was obtained from all competent patients; in cases in which prior consent could not be obtained due to critical illness, two doctors could consent to initiation of the study. In cases where patient consent was delayed, the patient or next-of-kin were informed as soon as possible and written consent/assent was sought to continue the study.
The study was a prospective, randomised, placebo-controlled trial. Patients were assigned to either a synbiotic mixture or placebo according to the contents of randomly assorted, sequentially numbered, sealed, opaque envelopes. The patient, study investigators, treating medical/nursing staff and microbiologists were all blinded to treatment allocation.
Treatment
All patients admitted to the ICU received a standard enteral feeding protocol as soon as possible (Table 1).
On arrival in ICU, patients were assigned randomly to receive at least two days (4 doses in 48 h) of either Synbiotic 2000 FORTE® (Medipharm, Kågero¨d, Sweden and Des Moines, IA), twice a day, or a crystalline cellulose-based placebo. Synbiotic 2000 FORTE® contains Pediococcus pentosaceus, Leuconostoc mesenteroides, Lactobacillus paracasei subsp paracasei and Lactobacillus plantarum (at a dose of 1010 bacteria per sachet [10]) as probiotics and Betaglucan, Inulin, Pectin and Resistant starch (2.5 g of each) as prebiotics. Synbiotic or placebo were dissolved in 50–100 ml of sterile water and given as a bolus through a nasogastric/orogastric tube. Both mixtures were presented in identical packaging and when prepared for administration, it was not possible to tell which was active material and which was placebo. Synbiotic/placebo administration was commenced in all patients within 24 h of admission to ICU and was continued twice daily to the earliest of the following time points: day 28 after admission, death or discharge from a critical care area.
Data collection
Demographic data (sex, age, medical speciality, etc.) and Acute Physiology and Chronic Health Evaluation (APACHE) II scores were recorded on admission. Number of days of ventilation, ICU and hospital stay, volume of nasogastric feed, successful administration of synbiotic, use of prokinetic agents, parameters of infection (temperature, leukocyte count) and antibiotic use were monitored prospectively. Microbiological investigations, including bronchoalveolar lavage (BAL), were performed when indicated clinically.
Microbiological analysis
Oropharyngeal throat swabs (Probact™Transport Swabs, Technical Service Consultants Ltd, Heywood, Lancashire) were obtained on admission to the trial and on the fourth and seventh day thereafter. Swabs were cultured by a microbiologist blinded for study groups. The timing of these cultures was designed to reflect baseline pharyngeal flora (admission swab), the flora at the pre-determined arbitrary watershed between early and late onset VAP (fourth day) and to describe flora at a time when the incidence of VAP is high (seventh day) [2]. The fourth day was also chosen to correlate with information from a preliminary study, which demonstrated presence of lactobacillus in stool culture after 3 days of synbiotic therapy [20]. We chose not to collect gastric microbiological data because a number of trials have demonstrated that, whilst tracheal colonisation is almost a prerequisite to development of VAP, the same organisms can be retrieved from the stomach in only a minority of cases [21–23].
Tracheal aspirates and bronchoalveolar lavage (BAL) specimens were obtained from patients as indicated clinically. Samples were processed routinely in the laboratory to yield qualitative results.
Diagnosis of VAP
Ventilator associated pneumonia was suspected if there were new progressive, or persistent (>24 h) infiltration on chest radiograph plus at least two of the following: (1) Temperature >38.0°C, (2) Leucocytosis (WBC count >12 × 103 μL−1) or leucopoenia (WBC count <4 × 103 μL−1), (3) Purulent tracheobronchial secretions [24]. All suspected cases were reviewed with appropriate clinical, radiological and sequential microbiological data (tracheal aspirates and bronchoalveolar lavage). Diagnosis was made prospectively and only confirmed if a blinded microbiologist and intensive care physician agreed on the diagnosis. Pneumonia was classified as VAP when diagnosed >48 h after intubation. Pneumonia was classified as early onset when diagnosed within the first 4 days of mechanical ventilation, and late onset thereafter [2].
Outcome variables
The primary outcome variable of the study was the incidence of VAP. Secondary outcome variables were oropharyngeal flora, ventilator days, and VAP rates per 1,000 ventilator days, ICU length of stay, ICU mortality and hospital mortality [25].
Safety
Throughout the study, all deaths were reviewed to see if a probiotic species administered might have contributed to the death. Any microbiological sample containing a probiotic species was highlighted and the option of withdrawing the patient from the trial was discussed with the treating clinician.
Statistics
The magnitude of any potential effect of synbiotics on the incidence of VAP is unknown. However, studies in allied areas of critical care including, liver transplantation, major surgery, pancreatitis and head injury have demonstrated impressive results with infectious complications decreasing by 50–75% [15–17, 26]. Based on these data, a 50% reduction in the incidence of VAP was the objective of this study.
Power analysis was performed with an expected decrease in the incidence of VAP from 28 to 14% [2]. This predicted that 130 patients would be required in each group (β 0.80, α 0.05). Local experience obtained during a preliminary study suggested an approximate 20% dropout rate after randomisation; we therefore aimed to recruit 300 patients in total and analyse data per protocol. Data are expressed as absolute numbers with or without percentages, as mean values with standard deviation or as medians with ranges as appropriate. Anderson–Darling tests were performed to check for normality of distribution. Chi-squared or Fisher’s exact test were used to compare proportions, Students T test or Mann–Whitney test to compare continuous variables. Incidence rates for pneumonia were compared using risk ratios with 95% confidence interval. The duration of mechanical ventilation, ICU and hospital stays were modified to take into account patients who died, by allocating those patients a surrogate value that was greater than the maximal value in any patient who survived [27]. This technique has been utilised to reduce the statistical distortion caused by early death upon length of stay parameters. A probability value <0.05 was considered significant and all tests were two sided.
Results
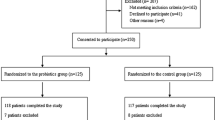
During the 13-month study period, 259 patients successfully completed the trial (Fig. 1). The baseline characteristics of the two groups were similar and summarised in Table 2.

CONSORT flow diagram of trial
Primary endpoint
During the study period, VAP was diagnosed in 12 (9%) of the patients receiving synbiotics and 17 (13%) in the placebo group (Table 3). The relative risk of VAP among patients assigned to receive synbiotics as compared with those assigned to receive placebo was 0.70 (95% CI 0.35–1.41; P = 0.42). The incidence of early and late VAP was also similar with 2 early episodes in both groups and 10 and 15 late episodes (P = 0.37) in the synbiotic and placebo groups, respectively.
Secondary endpoints
As expected, oropharyngeal flora was seen to change from Day 0 to Days 4 and 7 (Table 4). Importantly, however, the use of synbiotics did not alter the microbial species isolated or the rates of colonisation by potential pathogens. Interestingly, several of the patients had oropharyngeal colonisation with enteric Gram-negative organisms on admission (18% in the synbiotic and 18% in the placebo group). Oropharyngeal colonisation patterns predicted the organism responsible for VAP in 9 of 12 and 9 of 16 VAP episodes in the synbiotic and placebo group, respectively. However, as detailed phenotyping of microorganisms was not part of the protocol, we cannot be sure if oropharyngeal and VAP organisms were identical.
The number of VAP episodes per 1,000 ventilator days, ICU length of stay, ICU mortality and hospital mortality are all shown in Table 5. Synbiotic administration did not decrease the number of days ventilated (5.0 days in both groups), VAP episodes per 1,000 ventilator days (13 vs. 14.6 for placebo) or alter the bacterial flora responsible for VAP. ICU and hospital length of stay data did not differ significantly between treatment and placebo groups. Patients receiving synbiotic, when compared to placebo had ICU mortality rates of 21.5 and 26.9% and hospital mortality rates of 26.3 and 32.5%, P = 0.44 and 0.39, respectively.
Antibiotic administration was similar between the two groups. Every patient who received antibiotics at some point during their ICU stay is represented in Supplementary table, which shows the number of patients receiving different classes of antibiotics on a daily basis for the first 7 days. In addition to those patients represented in Supplementary table, 22 patients received no antibiotics during their stay (n = 12 placebo).
Safety
No obvious complications attributable directly to the synbiotic mixture or placebo were noted during the study period. The overall incidence of diarrhoea was low affecting only 16 patients in total (9 in placebo and 7 in synbiotic group). Organisms contained within the synbiotic mixture were cultured only once (Leuconostoc species) from a single tracheal aspirate. The significance of this result (Leuconostoc is a common oropharyngeal commensal) is uncertain as further, repeat cultures failed to isolate the organism.
Discussion
Our study demonstrated that administration of Synbiotic 2000 FORTE® via a nasogastric tube in a general ICU had no statistically significant impact on the incidence of VAP in the critically ill patients studied when compared with placebo. Although a negative study, this is an important finding as no other studies have examined the use of synbiotics in such a large, general critically ill population examining the effect on VAP, a real clinical problem on which synbiotics might be reasonably expected to have an impact.
This finding is supported by two recent meta-analyses, of small heterogeneous populations of critically ill patients, which [also] failed to show a reduction in infectious complications [28, 29]. Contrary to these findings positive results have been published in small studies in trauma and liver transplant patients, demonstrating strong trends towards pneumonia reduction with synbiotic use [14, 16].
The possibility of type II error and erroneously concluding an absent effect is a potential criticism of our trial. The power of the study was based on the assumption that synbiotics would reduce the incidence of VAP from 28 to 14%. The absence of similar studies made power calculations difficult and the eventual number chosen was based on published VAP rates and the published effects of probiotics in other critical care areas. A 50% absolute reduction in VAP may have been overly optimistic, but previous VAP interventions have surpassed this effect [30]. If our data can be regarded as hypothesis generating, then our study had a power of 18% to detect a 30% relative (4% absolute) VAP reduction from a baseline incidence of 13% and an appropriately powered trial would have needed 750 patients in each arm. This is clearly beyond a single centre trial.
We hypothesised that one of the main mechanisms by which synbiotics could reduce VAP is by modification of oropharyngeal flora. The observed failure to modify this flora is likely to be central in accounting for an absent benefit. The frequent identification of baseline PPM oropharyngeal colonisation, high preliminary antibiotic requirement (81% synbiotic, 78% placebo) and prevalence of gastric dysmotility all conspired to reduce any potential efficacy of the trial. Indeed, our dysmotility rates were lower than previously published synbiotic studies [17]. Restricting entry criteria to include only patients who were enterally fed successfully, may have improved the results. We considered this during trial design but noted that the high incidence of dysmotility observed within this population could have led to an unacceptably high exclusion rate and an even later initiation of synbiotics [31].
Diagnosing VAP is highly controversial and no gold standard exists. We chose not to use quantitative cultures to confirm VAP for a number of reasons: first, the reliability and reproducibility of quantitative samples relies on appropriately trained ICU and laboratory staff being available 24 h per day [32]. This system is not currently standard in our institution and we felt that adoption of this technique could introduce an unacceptable error rate. Second, quantitative sampling have not convincingly demonstrated either improved diagnostic accuracy or a mortality benefit to general ICU patients [33, 34].
As an alternative, we chose to diagnose VAP using two blinded, independent adjudicators. This technique is not new and has been used successfully in a number of studies [30, 34]. The potential advantage of this method is that it increases sensitivity (confirming VAP where the diagnosis seems likely despite a quantitative result below an arbitrary threshold) and specificity. The risk of oversensitivity was reduced by maintenance of strict blinding and adherence to explicit diagnostic criteria throughout. The success of this technique is supported by an observed incidence of VAP that is comparable to quantitative studies [35, 36]. In addition, the double-blind nature of the trial meant that any error introduced by our diagnostic technique would affect both groups equally.
The potential effect of antibiotic use on the observed VAP incidence cannot be excluded. During the study period, 80% of patients were receiving antibiotics on ICU admission and only 3 patients, diagnosed with VAP, were antibiotic naïve to that point. The diagnosis of VAP can be more difficult under these circumstances, particularly when quantitative cultures are relied upon. The diagnostic technique we chose resulted in frequent lower airway sampling (79% of eventual VAP diagnoses) and isolation of a pathogenic microorganism. Sterile qualitative cultures may have been present in some cases of VAP and this may explain why we observed a VAP rate 50% lower than predicted.
The synbiotic mixture with maximum effect in the critically ill has yet to be defined. The synbiotic mixture chosen for this trial was based on critical care experience (500 patients worldwide) and an exemplary safety record. The dose and potential impact of Synbiotic 2000 FORTE® is extrapolated from published data demonstrating benefit in trauma, liver transplantation and major abdominal surgery (pylorus-preserving pancreatoduodenectomy) [14, 16, 17]. The two key differences between these successful studies and our own are the homogenous nature of each studies population and early, successful initiation of synbiotic containing enteral nutrition.
The individual probiotic species selected for synbiotic 2000 are based on careful selection, as only a tiny minority of lactic acid producing bacteria have antimicrobial, anti-inflammatory, antioxidant effects and survive to reach the colonic mucosa [20, 37]. The choice of synbiotic mixture has been highlighted by the recently published PRObiotics in PAncreatitis TRIAl (PROPATRIA), which used a mixture of six probiotic strains of which only two have been shown to effectively reduce the growth of pathogens frequently observed in pancreatitis [38, 39]. This trial has also brought into question the safety of probiotics with an increased mortality in the probiotic group. The unexpected increased incidence of bowel ischaemia observed in the PROPATRIA trial was not seen in our trial and, whilst not explicitly reported, does not seem to be a problem reproduced by any other synbiotic trial.
In conclusion, in a prospective, randomised, double blind, placebo controlled trial of 259 heterogeneous MV critically ill patients, the administration Synbiotic 2000 FORTE® had no statistically significant impact on the incidence of VAP, the bacterial flora responsible for VAP or the number of days of mechanical ventilation. No complications directly attributable to the synbiotic mixture were noted during the trial in terms of increased mortality or morbidity. If synbiotics do reduce the incidence of VAP then this effect is the modest and future trials will require much larger patient populations.
References
Ibrahim EH, Tracy L, Hill C, Fraser VJ, Kollef MH (2001) The occurrence of ventilator-associated pneumonia in a community hospital: risk factors and clinical outcomes. Chest 120:555–561
American Thoracic Society Infectious Diseases Society of America (2005) Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med 171:388–416
Rello J, Ollendorf DA, Oster G, Vera-Llonch M, Bellm L, Redman R, Kollef MH (2002) Epidemiology and outcomes of ventilator-associated pneumonia in a large US database. Chest 122:2115–2121
Richards MJ, Edwards JR, Culver DH, Gaynes RP (1999) Nosocomial infections in medical intensive care units in the United States: National Nosocomial Infections Surveillance System. Crit Care Med 27:887–892
Tenover FC, Hughes JM (1994) WHO Scientific working group on monitoring and management of bacterial resistance to antimicrobial agents. Emerg Infect Dis 1:37
Schrezenmeir J, de Vrese M (2001) Probiotics, prebiotics, and synbiotics—approaching a definition. Am J Clin Nutr 73:361S–364S
Du Moulin GC, Paterson DG, Hedley-Whyte J, Lisbon A (1982) Aspiration of gastric bacteria in antacid-treated patients: a frequent cause of postoperative colonisation of the airway. Lancet 1:242–245
Valles J, Artigas A, Rello J, Bonsoms N, Fontanals D, Blanch L, Fernandez R, Baigorri F, Mestre J (1995) Continuous aspiration of subglottic secretions in preventing ventilator-associated pneumonia. Ann Intern Med 122:179–186
Jain PK, McNaught CE, Anderson ADG, MacFie J, Mitchell CJ (2004) Influence of synbiotic containing Lactobacillus acidophilus LA5, Bifidobacterium lactis BP12, Streptococcus thermophilus, Lactobacillus bulgaricus and oligofructose on gut barrier function and sepsis in critically ill patients: a randomized controlled trial. Clin Nutr 23:467–475
Bhatia SJ, Kochar N, Abraham P (1989) Lactobacillus acidophilus inhibits growth of Campylobacter pylori in vitro. J Clin Microbiol 27:2328–2330
van Minnen LP, Timmerman HM, Lutgendorff F, Verheem A, Harmsen W, Konstantinov SR, Smidt H, Visser MR, Rijkers GT, Gooszen HG, Akkermans LM (2007) Modification of intestinal flora with multispecies probiotics reduces bacterial translocation and improves clinical course in a rat model of acute pancreatitis. Surgery 141:470–480
Zareie M, Johnson-Henry K, Jury J, Yang P-C, Ngan B-Y, McKay DM, Soderholm JD, Perdue MH, Sherman PM (2006) Probiotics prevent bacterial translocation and improve intestinal barrier function in rats following chronic psychological stress. Gut 55:1553–1560
Alberda C, Gramlich L, Meddings J, Field C, McCargar L, Kutsogiannis D, Fedorak R, Madsen K (2007) Effects of probiotic therapy in critically ill patients: a randomized, double-blind, placebo-controlled trial. Am J Clin Nutr 85:816–823
Spindler-Vesel A, Bengmark S, Vovk I, Cerovic O, Kompan L (2007) Synbiotics, prebiotics, glutamine, or peptide in early enteral nutrition: a randomized study in trauma patients. J Parenter Enteral Nutr 31:119–126
Arruda ISF, Aguilar-Nascimento JE (2004) Benefits of early enteral nutrition with glutamine and probiotics in brain injury patients. Clin Sci 106:287–292
Rayes N, Seehofer D, Hansen S, Boucsein K, Müller AR, Serke S, Bengmark S, Neuhaus P (2002) Early enteral supply of lactobacillus and fiber versus selective bowel decontamination: a controlled trial in liver transplant recipients. Transplantation 74:123–127
Rayes N, Seehofer D, Theruvath T, Mogl M, Langrehr JM, Nüssler NC, Bengmark S, Neuhaus P (2007) Effect of enteral nutrition and synbiotics on bacterial infection rates after pylorus-preserving pancreatoduodenectomy: a randomized, double-blind trial. Ann Surg 246:36–41
Tablan OC, Anderson LJ, Besser R, Bridges C, Hajjeh R (2004) Healthcare Infection Control Practices Advisory Committee, Centres for Disease Control and Prevention. Guidelines for preventing health-care-associated pneumonia 2003: recommendations of the CDC and the Healthcare Infection Control Practices Advisory Committee. MMWR Recomm Rep 53(RR-3):1–36
Knight D, Girling K, Banks A, Snape S, Weston V, Bengmark S (2006) The effect of enteral synbiotics on the incidence of ventilator-associated pneumonia in mechanically ventilated critically ill patients. Crit Care 10(Suppl 1):P213
Knight DJW, Girling KJ (2004) The effect of Probiotics on gastrointestinal flora in the critically ill. Br J Anaesth 92:307–308
Cendrero J, Solé-Violá J, Benítez AB, Catalán JN (1999) Role of different routes of tracheal colonization in the development of pneumonia in patients receiving mechanical ventilation. Chest 116:462–470
Bonten MJ, Gaillard CA, van Tiel FH, Smeets HG, van der Geest S, Stobberingh EE (1994) The stomach is not a source for colonization of the upper respiratory tract and pneumonia in ICU patients. Chest 105:878–884
de Latorre FJ, Pont T, Ferrer A, Rossello J, Palomar M, Planas M (1995) Pattern of tracheal colonization during mechanical ventilation. Am J Respir Crit Care Med 152:1028–1033
Johanson WG, Pierce Ak, Sandford JP (1972) Nosocomial respiratory infections with gram-negative bacilli: the significance of colonization of the respiratory tract. Ann Intern Med 77:701–706
Institute for Healthcare Improvement: measuring the ventilator-associated pneumonia rate per 1000 ventilator days. http://www.ihi.org/IHI/Topics/CriticalCare/IntensiveCare/Measures/VentilatorAssociatedPneumoniaRateper1000VentilatorDays.htm. Accessed 07 March 2008
Oláh A, Belágyi T, Issekutz Á, Gamal ME, Bengmark S (2002) Early enteral nutrition with specific Lactobacillus and fibre reduces sepsis in severe acute pancreatitis. Br J Surg 89:1103–1107
Gomersall CD, Joynt GM, Freebairn RC, Hung V, Buckley TA, Oh TE (2000) Resuscitation of critically ill patients based on the results of gastric tonometry: a prospective, randomized, controlled trial. Crit Care Med 3:607–614
Isakow W, Morrow LE, Kollef MH (2007) Probiotics for preventing and treating nosocomial infections: review of current evidence and recommendations. Chest 132:286–294
Watkinson P, Barber V, Dark P, Young J (2006) The use of pre- pro- and synbiotics in adult intensive care unit patients: systematic review. Clin Nutr 26:182–192
Drakulovic MB, Torres A, Bauer TT, Nicolas JM, Nogue S, Ferrer M (1999) Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial. Lancet 354:1851–1858
Montejo JC, Grau T, Acosta J, Ruiz-Santana S, Planas M, Garcia-De-Lorenzo A, Mesejo A, Cervera M, Sanchez-Alvarez C, Nunez-Ruiz R, Lopez-Martinez JJ (2002) Multicentre, prospective, randomised, single blind study comparing the efficacy and gastrointestinal complications of jejunal feeding with early gastric feeding in critically ill patients. Crit Care Med 30:796–800
Gerbeaux P, Ledoray V, Boussuges A, Molenat F, Jean P, Sainty JM (1998) Diagnosis of nosocomial pneumonia in mechanically ventilated patients: repeatibility of the bronchoalveolar lavage. Am J Respir Crit Care Med 157:76–80
Rea-Neto A, Youssef NC, Tuche F, Brunkhorst F, Ranieri VM, Reinhart K, Sakr Y (2008) Diagnosis of ventilator-associated pneumonia: a systematic review of the literature. Crit Care 12:R56
The Canadian Critical Care Trials Group (2006) A randomized trial of diagnostic techniques for ventilator-associated pneumonia. N Engl J Med 355:2619–2630
Clec’h C, Jauréguy F, Hamza L, Karoubi P, Fosse JP, Hamdi A, Vincent F, Gonzalez F, Cohen Y (2006) Agreement between quantitative cultures of postintubation tracheal aspiration and plugged telescoping catheter, protected specimen brush, or BAL for the diagnosis of nosocomial pneumonia. Chest 130:956–961
Camargo LFA, De Marco FV, Barbas CSV, Hoelz C, Bueno MAS, Rodrigues M Jr, Amado VM, Caserta R, Martino MDV, Pasternak J, Knobel E (2004) Ventilator associated pneumonia: comparison between quantitative and qualitative cultures of tracheal aspirates. Crit Care 8:R422–R430
Kruszewska D, Lan J, Lorca G, Yanagisawa N, Marklinder I, Ljungh Å (2002) Selection of lactic acid bacteria as probiotic strains by in vitro tests. Microecol Ther 29:37–51
Besselink MG, van Santvoort HC, Buskens E, Boermeester MA, van Goor H, Timmerman HM (2008) Probiotic prophylaxis in predicted severe acute pancreatitis: a randomised, double-blind, placebo-controlled trial. Lancet 371:651–659
Ridwan BU, Koning CJ, Besselink MG, Timmerman HM, Brouwer EC, Verhoef J, Gooszen HG, Akkermans LM (2008) Antimicrobial activity of a multispecies probiotic (Ecologic 641) against pathogens isolated from infected pancreatic necrosis. Lett Appl Microbiol 46:61–67
Acknowledgments
The authors were supported by grants from Special trustees fund, Nottingham NHS trust. Medipharm (free supply of synbiotic and placebo).
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
134_2008_1368_MOESM1_ESM.doc
Daily mean Nasogastric feed administration and numbers of patients receiving antibiotic administration by class (DOC 48 kb)
Rights and permissions
About this article
Cite this article
Knight, D.J.W., Gardiner, D., Banks, A. et al. Effect of synbiotic therapy on the incidence of ventilator associated pneumonia in critically ill patients: a randomised, double-blind, placebo-controlled trial. Intensive Care Med 35, 854–861 (2009). https://doi.org/10.1007/s00134-008-1368-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-008-1368-1