
Abstract
Objectives
To study the pattern of lung emptying and expiratory resistance in mechanically ventilated patients with chronic obstructive pulmonary disease (COPD).
Design
A prospective physiological study.
Setting
A 12-bed Intensive Care Unit.
Patients
Ten patients with acute exacerbation of COPD.
Interventions
At three levels of positive end-expiratory pressure (PEEP, 0, 5 and 10 cmH2O) tracheal (Ptr) and airway pressures, flow (V’) and volume (V) were continuously recorded during volume control ventilation and airway occlusions at different time of expiration.
Measurements and results
V-V’ curves during passive expiration were obtained, expired volume was divided into five equal volume slices and the time constant (τ) and dynamic deflation compliance (Crsdyn) of each slice was calculated by regression analysis of V-V’ and post-occlusion V-Ptr relationships, respectively. In each volume slice the existence or not of flow limitation was examined by comparing V-V’ curves with and without decreasing Ptr. For a given slice total expiratory resistance was calculated as τ/Crsdyn, whereas expiratory resistance (Rrs) and time constant (τrs) of the respiratory system were subsequently estimated taken into consideration the presence of flow limitation. At zero PEEP, τrs increased significantly toward the end of expiration due to an increase in Rrs. PEEP significantly decreased Rrs at the end of expiration and resulted in a faster and relatively constant rate of lung emptying.
Conclusions
Patients with COPD exhibit a decrease in the rate of lung emptying toward the end of expiration due to an increase in Rrs. PEEP decreases Rrs, resulting in a faster and uniform rate of lung emptying.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by increased resistance to airflow and loss of lung elastic recoil. These disturbances in respiratory system mechanics decrease the rate of lung emptying and may cause flow limitation during passive expiration [1, 2, 3]. As a result dynamic hyperinflation and intrinsic positive end-expiratory pressure (PEEPi) may develop [1, 2, 3]. Although flow limitation and PEEPi may be present in stable COPD [4], it is invariably encountered during acute exacerbation of the disease [5].
In mechanically ventilated patients with acute exacerbation of COPD, dynamic hyperinflation is an important factor which considerably increases the morbidity and mortality of the disease. Indeed, ventilatory strategies in these patients are mainly planned to reduce the magnitude of dynamic hyperinflation [6]. It follows that the assessment of pattern of lung emptying and, particularly, expiratory resistance (the main determinant of dynamic hyperinflation in these patients) is of fundamental importance for understanding the disease pathophysiology and its interaction with the mechanical ventilation. However, in the presence of flow limitation, expiratory flow is independent of airway pressure (Paw) and, thus, the assessment of expiratory resistance using the difference between alveolar and airway pressure as driving pressure for flow is not valid [2, 7, 8]. Recently, in patients with acute respiratory distress syndrome (ARDS), we described a technique that estimates the expiratory resistance of respiratory system at presence of flow limitation [9]. The purpose of the present study was to examine the pattern of lung emptying and assess expiratory resistance in patients with acute exacerbation of COPD during controlled mechanical ventilation, taking the presence of flow limitation into consideration. This may help us to gain a better understanding of the behavior of the respiratory system during expiration in these patients. Furthermore, because indirect data indicate that external positive end-expiratory pressure (PEEP) may decrease expiratory resistance in flow-limited patients by counteracting airway compression [10, 11], the effects of PEEP on respiratory system mechanics were also examined.
Methods (see also Electronic Supplementary Material)
Ten patients with COPD, requiring mechanical ventilation to manage acute respiratory failure due to an acute exacerbation of chronic airflow obstruction, were studied. All patients had a previous diagnosis of COPD and met established spirometric criteria for this diagnosis [12]. The Institutional Ethics Committee approved the study and informed consent was obtained from each patient or next of kin.
All patients were ventilated on volume control mode (Puritan-Bennett, Carlsad, CA, or Evita 2, Drager, Germany) using a constant inspiratory flow rate and settings determined by the primary physician (Table 1). In all patients no end-inspiratory pause was applied, whereas inspiratory time to total breath duration was equal to or less than 1/3. For the purpose of the study the patients were heavily sedated to achieve respiratory muscle inactivity [13]. Flow (V’) at the airway opening was measured with a heated pneumotachograph (3700, Hans-Rudolf, Kansas City, MO), placed between the endotracheal tube and the Y-piece of the ventilator. A manually operated pneumatic driven occlusion valve (Hans-Rudolf 9300) was inserted between the pneumotachograph and the Y-piece of the ventilator. Volume (V) and airway and tracheal pressures were measured as previously described [9].
Protocol
Each patient was studied at three levels of PEEP (0, 5 and 10 cmH2O) applied randomly. Ventilator settings were the same at all levels of PEEP as determined by the primary physician (Table 1). Tidal volume (VT) was, however, increased by 70 ml to compensate for the increase in dead space due to instrumentation. When the patients were stable on each PEEP level (at least 25 min) arterial blood gasses were measured. Thereafter, the airways were occluded at end-inspiration for 3 s using the end-inspiratory hold button of the ventilator and after the release of the occlusion various manipulations were performed [9]. These manipulations were as follow:
-
1.
The patient was permitted to exhale to end-expiratory lung volume determined by the PEEP level and the duration of expiration (Fig. 1a).
Fig. 1 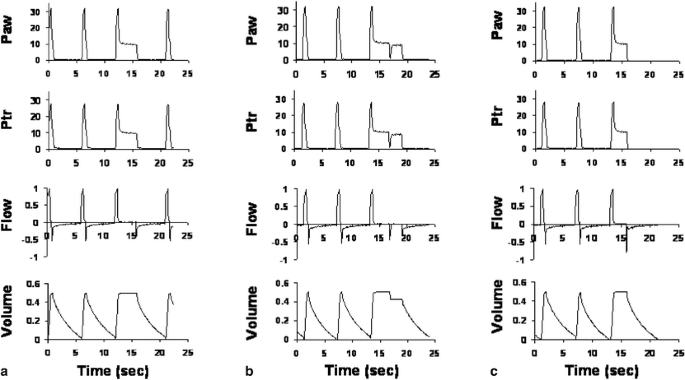
Airway (Paw, cmH2O) and tracheal (Ptr, cmH2O) pressures, flow (l/s) and volume (l) in a representative patient ventilated with zero positive end-expiratory pressure during the various manipulations of the study. a Passive un-interrupted expiration after end-inspiratory occlusion, to end-expiratory lung volume (determined by the ventilator expiratory time) in the presence of the ventilator expiratory circuit. b Rapid airway occlusion during expiration. c Passive un-interrupted expiration after end-inspiratory occlusion to end-expiratory lung volume without the ventilator expiratory circuit. Observe the difference in peak expiratory flow after release of end-inspiratory occlusion between a (0.44 l/s) and c (0.78 l/sec), due to different downstream pressure (i.e., lower Ptr and Paw in c). Notice also that Ptr is lower during inspiration and higher during expiration than the corresponding values of Paw. At low expiratory flow Ptr is slightly higher than Paw, while at zero flow Paw and Ptr are identical
-
2.
Airway occlusions lasting approximately 3 s were performed randomly at different time of expiration (Fig. 1b). Each study breath was occluded once during expiration after the release of end-inspiratory occlusion using the pneumatic occlusion valve. In each subject and for a given level of PEEP at least 20 airway occlusions during expiration were performed aiming to obtain data throughout expiration. Tracheal pressure exhibited two distinct pressure changes after interruption, an initial rapid increase (Ptrinit) followed by a slower increase to a plateau value [9, 14, 15, 16]. By plotting Ptrinit against the corresponding volume above passive functional residual capacity (FRC) Ptrinit-volume curve were constructed at all PEEP levels [9].
-
3.
With zero PEEP, passive expiration was performed directly to the atmosphere by removing the expiratory ventilator circuit during the preceding end-inspiratory occlusion (Fig. 1c). When PEEP was applied, the PEEP was reduced by 2 cmH2O during the end-inspiratory occlusion and the patient permitted to exhale to the new PEEP level [9].
-
4.
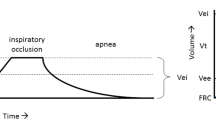
At each level of PEEP, end-expiratory lung volume above passive FRC (EELV) was calculated by removing the expiratory ventilator circuit during the preceding end-inspiratory occlusion and permitting the patient to exhale passively to the atmosphere until expiratory flow became zero. EELV was calculated as the difference between the total expired volume and VT.

For a given experimental condition PEEPi was measured using the end-expiratory occlusion method [17].
Data analysis
Step 1: Assessment of flow limitation
For a given PEEP, an expiratory flow-volume curve was obtained with and without decreasing the downstream pressure. The presence of flow limitation was assessed by comparing expiratory flows at a given portion of lung volume (Fig. 2) [2, 9, 18, 19].

Expiratory flow-volume curves, obtained at two PEEP levels (upper panel: zero PEEP; lower panel: 10 cmH2O PEEP) with (dashed lines) and without (solid lines) decreasing the airway pressure in a representative patient. With zero PEEP, bypassing the expiratory ventilator circuit caused an initial increase in expiratory flow, which subsequently decreased to values obtained with expiratory ventilator circuit in place. With 10 cmH2O of PEEP expiratory flows were consistently lower (>5%) than those observed when PEEP was reduced by 2 cmH2O during the preceding end-inspiratory occlusion (PEEP positive end-expiratory pressure)
Step 2: Determination of the pattern of emptying
The pattern of emptying was assessed using the method of Guttmann et al. [20]. Briefly, at each PEEP level the average volume-flow curve during uninterrupted expiration was analyzed. Volume was plotted against flow and the inflection point of the curve, defined as the point of maximum slope of the curve following the expiratory peak flow, was identified [9]. The expired volume from inflection point to the end of expiration was then subdivided into five consecutive slices of equal size (Fig. 3). The slope of the linear fit to V-V’ data pertaining to a given volume slice was taken as the time constant (τ) for that slice.

Flow-volume (upper panel) and post-occlusion tracheal pressure-volume (lower panel) curves during passive expiration in a representative patient ventilated with zero PEEP. Upper panel: Small arrows indicate the analyzed volume slices. Lower panel: Closed circles; Data points. Open triangles; Points obtained by the equation curve-fitted to the data. Long arrows (both panels) indicate the direction of expiration
For a given volume slice, total resistance (Rtot) was calculated as τ/Crsdyn, where Crsdyn was the dynamic deflation compliance, defined as the slope of volume/Ptrinit relationship, obtained by linear regression analysis of the deflation Ptrinit-volume curve on points at that particular volume slice. Although for a given PEEP, to construct the Ptrinit-volume curve, at least 20 points were obtained, the number of points was not sufficient for some volume slices, making the regression analysis questionable. For this reason the Ptrinit-volume curve was described using the sigmoidal equation proposed by Venegas et al. [21, 22] (Fig. 3). Considering that Crsdyn was nearly constant in each volume slice, linear regression analysis on points obtained by the sigmoidal equation was performed and Crsdyn of the volume slice was determined as the slope of volume/Ptrinit relationship.
Volume slices were considered to be non-flow limited if expiratory flows were consistently higher (>5%) when Paw was lowered for at least 90% of the volume slice (Fig. 2). In these slices, the time constant of pure respiratory system (τrs) was calculated as the product of Crsdyn and flow resistance of respiratory system (Rrs). Rrs was calculated by subtracting from Rtot the endotracheal tube (Rtube) and expiratory ventilator circuit (Rvent) resistances [9]. Where flow limitation was present for at least 90% of the volume slice (Fig. 2), τ obtained from the slope of volume/flow relationship and Rtot calculated from τ/Crsdyn ratio were considered, respectively, to be the τrs and Rrs. Where flow limitation was present for less than 90% of the total volume slice the flow and non-flow limited segments were analyzed separately, as described above for volume slices with and without flow limitation. The Rrs of that volume slice was calculated by adding the Rrs of the flow and non-flow limited segment, corrected for their contribution to the total resistance as previously described [9].
Data were analyzed by multi-factorial analysis of variance for repeated measurements (ANOVA) and linear regression analysis, where appropriate. A value of P<0.05 was considered statistically significant. Data are expressed as mean ± SD.
Results (see also Electronic Supplementary Material)
The analyzed volume slice averaged 0.09±0.01, 0.09±0.01 and 0.10±0.01 l with 0, 5 and 10 cmH2O of PEEP, respectively (P>0.05). With zero PEEP, EELV amounted to 0.43±0.39 l, and increased significantly with increasing PEEP (ΔEELV 0.17±0.16 and 0.60±0.25 l with 5 and 10 cmH2O of PEEP, respectively). Total PEEP (external + intrinsic) is shown in Table 2. Blood gasses remained relatively stable throughout (P>0.05, data not shown).
In all cases and independent of conditions studied, the sigmoidal equation was fitted to the V-Ptrinit data adequately, yielding R2 values above 0.98. Similarly, in each volume slice the V/Ptrinit relationships were described with excellent accuracy, due to the relatively small volume size, by linear regression analysis (R2>0.99). Furthermore, in each volume slice the V/V’ relationship was highly linear (R2>0.90).
Crsdyn did not differ as a function of PEEP and increased progressively toward the end of expiration (Table 3). The difference between Ptrinit and Ptrplateau did not differ as a function of PEEP, averaging at mid-tidal volume 0.9±0.2, 1.0±0.3 and 1.1±0.5 cmH2O with 0, 5 and 10 cmH2O PEEP, respectively. Independent of PEEP, at the first volume slice Crsdyn was slightly, but significantly, lower than volume/Ptrplateau relationship. Without PEEP, τ and τrs increased significantly from the beginning (first slice) to the end expiration (fifth slice) (Table 4). This difference decreased progressively with increasing PEEP. These changes in time constant were mainly due to alteration in expiratory resistance (Rtot and Rrs) (Table 5 and Fig. 4).

Individual respiratory system expiratory resistance as a function of volume slice and PEEP. Arrow indicates the direction of expiration. In each plot the patient’s number appears in the upper right corner. Notice in each patient the effect of PEEP on end-expiratory lung volume above passive FRC. Black lines: zero PEEP. Red lines: 5 cmH2O PEEP. Green lines: 10 cmH2O PEEP. For clarity of presentation the scale of x and y axes is different in each patient depending on individual values
Discussion
The main findings of this study were: (1) patients with acute exacerbation of COPD, mechanically ventilated with zero PEEP, exhibited flow limitation during a significant part of expiration, (2) with zero PEEP expiratory resistance of respiratory system at the end of expiration was significantly higher than that at the beginning of expiration, causing a significant braking of the lung emptying, and (3) application of PEEP caused a graded decrease in expiratory resistance, resulting in a faster and more uniform rate of lung emptying.
Previous studies have shown that flow limitation during passive expiration is common feature in this group of patients [2, 23]. We also demonstrated that the magnitude of flow limitation decreased progressively with increasing PEEP, in line with data showing a reduction in flow limitation by external resistance, as suggested by the decrease in spike area of expiratory flow obtained after rapid release of airway occlusion [11]. It is of interest to note that with PEEP in some of our patients flow limitation was observed only at the beginning of expiration, probably due to relatively high expiratory flows and alveolar-tracheal pressure difference [7, 8]. The existence of flow limitation makes the calculation of expiratory resistance using the difference between alveolar and mouth pressures as driving pressure for flow unreliable [7, 8]. The calculation of expiratory resistance is further complicated by the non-linear dynamic pressure-volume relationship of the respiratory system observed during tidal expiration, which precludes the use of a single value of elastance to estimate alveolar pressure.
In our study we assumed that, in the presence of flow limitation, removal of endotracheal tube did not affect expiratory flow. However, this is not always true because endotracheal tube removal, by decreasing tracheal pressure to zero, may cause further compression of downstream airways and decrease in expiratory flow, a phenomenon referred to as negative effort dependence [24]. In this case, in the presence of flow limitation, time constant and expiratory resistance of respiratory system are underestimated. We believe that this underestimation, if any, should be of a small magnitude because negative effort dependence is observed with considerable decrease in downstream pressure [23, 24]. In our study the pressure drop across the tube was minimal due to low expiratory flow. Additionally, we did not observe negative effort dependence when Paw decreased by 1–2 cmH2O. Nevertheless, the phenomenon of negative effort dependence should be present mainly at zero PEEP where flow limitation was observed during a significant part of expiration, thus strengthening the results of our study (i.e., underestimation of τrs and Rrs with zero PEEP).
The volume/flow relationship was obtained during passive deflation after a 3-s end-inspiratory pause. During that time elastic energy stored during inspiration to the viscoelastic elements of the respiratory system was dissipated [25], and the pressure that initially drove expiratory flow was the static recoil pressure [26]. Thereafter, the recoil pressure that determined the expiratory flow was estimated by rapid airway occlusion and measuring Ptrinit, which was lower than the static recoil pressure, due to regional ventilation and/or viscoelasticity (stress recovery) [14, 15, 16, 27]. It follows that during expiration the V/Ptrinit relationship dictates, in association with total airflow resistance, the V/V’ relationship [9].
Lourens et al. [28] measured the expiratory time constant in mechanically ventilated COPD patients by calculating the quotient of exhaled volume and the corresponding change in flow at 100% and the last 75%, 50% and 25% of exhaled volume, and observed a progressive increase in time constant toward the end of expiration, results qualitatively similar to ours. Their analysis, however, is greatly complicated by the curvilinear shape of volume-flow curve [29]. It follows that mainly qualitative information on the pattern of lung emptying can be obtained by this method [29]. Indeed, the limits of agreements between the predicted time needed for complete expiration and the actual time were quite large (approximately ±6 s) [28]. On the other hand, in our study, expiratory time constant was calculated by regression analysis using independent small volume portions (approximately 90 ml), a method that largely circumvents the problem of the shape of volume-flow curve. In this relatively small volume range, the V/V’ relationship was highly linear with an r value approaching unity in all cases. Therefore, it is reasonable to assume that the volume course in each volume slice might be adequately described by a mono-exponential function with a single time constant. Thus, we were able to quantify the volume dependence of expiratory time constant. Furthermore, we demonstrated that the pattern of passive lung emptying is considerably affected by PEEP. The observed volume and PEEP dependence of the rate of lung emptying indicate that when expiratory time constant is calculated in these patients the expired volume at which calculation was performed, as well as the PEEP level, should be specified.
The fact that, with zero PEEP, flow limitation was observed in all patients during a significant portion of expired volume caused, as dictated by our method of data analysis, the expiratory resistance and time constant of the whole system (respiratory system, endotracheal tube and expiratory ventilator circuit) to be closely similar to those pertaining only to respiratory system. These results are different from those obtained in patients with ARDS (using a similar analysis) in whom the expiratory time constant of the whole system was significantly different from that of respiratory system [9]. This discrepancy is likely due to two reasons. Firstly, compared to patients with ARDS, patients with COPD exhibited flow limitation during a significant greater portion of expired volume. Secondly, in our patients expired flows were considerably lower than these in ARDS patients. Low expiratory flow in the absence of flow limitation minimizes the contribution of endotracheal tube and ventilator expiratory circuit to total pressure drop. It follows that in patients with COPD mechanically ventilated with zero PEEP, neither endotracheal tube nor expiratory circuit modifies significantly the pattern of lung emptying. In these patients, calculating the time constant using the volume-flow relationship may give a relatively accurate estimate of the true time constant of respiratory system. This, however, may not apply in presence of PEEP, which by decreasing expiratory resistance may eliminate the flow limitation.
Without PEEP, Rrs increased considerably toward the end of expiration. Compared to the first volume slice (beginning of expiration), Rrs of the fifth volume slice (end of expiration) increased more than twofold. To our knowledge this is the first study that quantifies effective expiratory resistance in mechanically ventilated patients with COPD. Airway closure and increasing airway compression could be the pathogenetic mechanisms of this increase [11, 30]. In patients in whom application of low levels of PEEP (5 cmH2O) caused a significant drop of respiratory system expiratory resistance without a concomitant increase in end-expiratory lung volume airway compression downstream from the choke point may predominate (Fig. 4, patients 1, 4, 7 and 9). Indeed, it has been shown that small airway closure is critically dependent on end-expiratory lung volume [30] and, therefore, if airway closure was the predominant mechanism for the observed change in expiratory resistance in these patients, we would expect a decrease only with corresponding increase in end-expiratory lung volume with PEEP. However, in other patients, particularly those with minimal end-expiratory air trapping and/or large increase in end-expiratory lung volume with PEEP application (Fig. 4), airway closure [30] should certainly contribute to the increase in effective expiratory resistance toward the end of expiration.
The significant decrease in expiratory resistance of the respiratory system observed with PEEP resulted in an increase in the overall rate of emptying. Although the purpose of the study was not to examine the effect of PEEP on dynamic hyperinflation, our data indicate that PEEP may be used as a method to reduce absolute lung volume by increasing the rate of lung emptying (see patients 7 and 9), in line with prediction of recent mathematical models of flow limitation [31]. It seems that, similar to assisted ventilatory support [32], PEEP may also be beneficial during passive mechanical ventilation. Nevertheless, the optimal amount of PEEP (certainly less than intrinsic PEEP) that reduces the dynamic hyperinflation, as well as the group of patients for whom application of PEEP for this purpose is indicated, remains to be studied. In several of our patients PEEPi at zero PEEP was relatively low (<5 cmH2O, Table 2), mainly due to applying ventilator strategy (low VT and long expiratory time). Thus, PEEP levels of 5 and 10 cmH2O were excessive and resulted in further increase in EELV. A different study design may clarify this issue.
The method of calculation of expiratory resistance is rather complex and might not be currently applicable at the bedside. Although the purpose of the study was to examine the pattern of lung emptying and expiratory resistance, and not to propose a new bedside method of measuring the time constant and expiratory resistance of respiratory system, future development of appropriate ventilator software might simplify the procedures.
References
Pepe PE, Marini JJ (1982) Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: the auto-PEEP effect. Am Rev Respir Dis 126:166–170
Georgopoulos D, Giannouli E, Patakas D (1993) Effects of extrinsic positive end-expiratory pressure on mechanically ventilated patients with chronic obstructive pulmonary disease and dynamic hyperinflation. Intensive Care Med 19:197–203
Ranieri VM, Giuliani R, Cinnella G, Pesce C, Brienza N, Ippolito EL, Pomo V, Fiore T, Gottfried SB, Brienza A (1993) Physiologic effects of positive end-expiratory pressure in patients with chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Am Rev Respir Dis 147:5–13
Haluszka J, Chartrand DA, Grassino AE, Milic-Emili J (1990) Intrinsic PEEP and arterial PCO2 in stable patients with chronic obstructive pulmonary disease. Am Rev Respir Dis 141:1194–1197
Rossi A, Polese G, Brandi G, Conti G (1995) Intrinsic positive end-expiratory pressure (PEEPi). Intensive Care Med 21:522–536
Georgopoulos D, Brochard L (1988) Ventilatory Strategies in acute exacerbations of COPD. Eur Respir Monogr 8:12–44
Dawson SV, Elliott EA (1977) Wave-speed limitation on expiratory flow-a unifying concept. J Appl Physiol 43:498–515
Elliott EA, Dawson SV (1977) Test of wave-speed theory of flow limitation in elastic tubes. J Appl Physiol 43:516–522
Kondili E, Prinianakis G, Athanasakis H, Georgopoulos D (2002) Lung emptying in patients with acute respiratory distress syndrome: effects of positive end-expiratory pressure. Eur Respir J 19:811–819
Smith TC, Marini JJ (1988) Impact of PEEP on lung mechanics and work of breathing in severe airflow obstruction. J Appl Physiol 65:1488–1499
Aerts JG, Berg B van den, Bogaard JM (1997) Controlled expiration in mechanically-ventilated patients with chronic obstructive pulmonary disease (COPD). Eur Respir J 10:550–556
Siafakas NM, Vermeire P, Pride NB, Paoletti P, Gibson J, Howard P, Yernault JC, Decramer M, Higenbottam T, Postma DS, et al (1995) Optimal assessment and management of chronic obstructive pulmonary disease (COPD). The European Respiratory Society Task Force. Eur Respir J 8:1398–1420
Prechter GC, Nelson SB, Hubmayr RD (1990) The ventilatory recruitment threshold for carbon dioxide. Am Rev Respir Dis 141:758–764
Bates JH, Baconnier P, Milic-Emili J (1988) A theoretical analysis of interrupter technique for measuring respiratory mechanics. J Appl Physiol 64:2204–2214
Beydon L, Svantesson C, Brauer K, Lemaire F, Jonson B (1996) Respiratory mechanics in patients ventilated for critical lung disease. Eur Respir J 9:262–273
Jonson B, Beydon L, Brauer K, Mansson C, Valind S, Grytzell H (1993) Mechanics of respiratory system in healthy anesthetized humans with emphasis on viscoelastic properties. J Appl Physiol 75:132–140
Gottfried SB, Rossi A, Higgs BD, Calverley PM, Zocchi L, Bozic C, Milic-Emili J (1985) Noninvasive determination of respiratory system mechanics during mechanical ventilation for acute respiratory failure. Am Rev Respir Dis 131:414–420
Koutsoukou A, Armaganidis A, Stavrakaki-Kallergi C, Vassilakopoulos T, Lymberis A, Roussos C, Milic-Emili J (2000) Expiratory flow limitation and intrinsic positive end-expiratory pressure at zero positive end-expiratory pressure in patients with adult respiratory distress syndrome. Am J Respir Crit Care Med 161:1590–1596
Valta P, Corbeil C, Lavoie A, Campodonico R, Koulouris N, Chasse M, Braidy J, Milic-Emili J (1994) Detection of expiratory flow limitation during mechanical ventilation. Am J Respir Crit Care Med 150:1311–1317
Guttmann J, Eberhard L, Fabry B, Bertschmann W, Zeravik J, Adolph M, Eckart J, Wolff G (1995) Time constant/volume relationship of passive expiration in mechanically ventilated ARDS patients. Eur Respir J 8:114–120
Venegas JG, Harris RS, Simon BA (1998) A comprehensive equation for the pulmonary pressure-volume curve. J Appl Physiol 84:389–395
Harris RS, Hess DR, Venegas JG (2000) An objective analysis of the pressure-volume curve in the acute respiratory distress syndrome. Am J Respir Crit Care Med 161:432–439
Lourens MS, Berg BV, Hoogsteden HC, Bogaard JM (2001) Detection of flow limitation in mechanically ventilated patients. Intensive Care Med 27:1312–1320
Morris MJ, Lane DJ (1981) Tidal expiratory flow patterns in airflow obstruction. Thorax 36:135–142
Barberis L, Manno E, Guerin C (2003) Effect of end-inspiratory pause duration on plateau pressure in mechanically ventilated patients. Intensive Care Med 29:130–134
Georgopoulos D, Mitrouska I, Markopoulou K, Patakas D, Anthonisen NR (1995) Effects of breathing patterns on mechanically ventilated patients with chronic obstructive pulmonary disease and dynamic hyperinflation. Intensive Care Med 21:880–886
Bates JH, Brown KA, Kochi T (1989) Respiratory mechanics in the normal dog determined by expiratory flow interruption. J Appl Physiol 67:2276–2285
Lourens MS, Berg B van den, Aerts JG, Verbraak AF, Hoogsteden HC, Bogaard JM (2000) Expiratory time constants in mechanically ventilated patients with and without COPD. Intensive Care Med 26:1612–1618
Rossi A, Polese G (2000) As simple as possible, but not simpler. Intensive Care Med 26:1591–1594
Guerin C, LeMasson S, de Varax R, Milic-Emili J, Fournier G (1997) Small airway closure and positive end-expiratory pressure in mechanically ventilated patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 155:1949–1956
Khirani S, Biot L, Eberhard A, Baconnier P (2001) Positive end expiratory pressure and expiratory flow limitation: a model study. Acta Biotheor 49:277–290
Guerin C, Milic-Emili J, Fournier G (2000) Effect of PEEP on work of breathing in mechanically ventilated COPD patients. Intensive Care Med 26:1207–1214
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00134-004-2435-x
Electronic Supplementary Material
Rights and permissions
About this article
Cite this article
Kondili, E., Alexopoulou, C., Prinianakis, G. et al. Pattern of lung emptying and expiratory resistance in mechanically ventilated patients with chronic obstructive pulmonary disease. Intensive Care Med 30, 1311–1318 (2004). https://doi.org/10.1007/s00134-004-2255-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00134-004-2255-z