
Abstract
Aim/hypothesis
We investigated the effects of the common polymorphisms in the peroxisome proliferator-activated receptor γ2 (PPAR-γ2; Pro12Ala) and in PPAR-γ coactivator 1α (PGC-1α; Gly482Ser) genes on the conversion from impaired glucose tolerance to type 2 diabetes in participants in the STOP-NIDDM trial. This trial aimed to study the effect of acarbose in the prevention of type 2 diabetes.
Methods
Genotyping was performed in 770 study subjects whose DNA was available. The Gly482Ser variant in the PGC-1α gene was determined with the polymerase chain reaction amplification, Hpa II enzyme digestion, and gel electrophoresis. The Pro12Ala polymorphism of the PPAR-γ2 gene was determined by the polymerase chain reaction–single-strand conformation polymorphism analysis.
Results
The Pro12Pro genotype of the PPAR-γ2 gene predicted the conversion to diabetes in women in the acarbose group (odds ratio 2.89, 95% CI 1.20 to 6.96; p=0.018). The 482Ser allele of the PGC-1α gene had a significant interaction with the mode of treatment (p=0.012), and in the placebo group the 482Ser allele was associated with a 1.6-fold higher risk for type 2 diabetes compared to the Gly482Gly genotype (95% CI 1.06 to 2.33; p=0.023). Acarbose prevented the development of diabetes independently of the genotype of the PPAR-γ2 gene, but only the carriers of the 482Ser allele of the PGC-1α gene were responsive to acarbose treatment.
Conclusion/interpretation
We conclude that the Pro12Pro genotype of the PPAR-γ2 gene and the 482Ser allele of the PGC-1α gene are associated with the conversion from impaired glucose tolerance to type 2 diabetes in the STOP-NIDDM trial.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes is a common disease due to both genetic and environmental factors [1, 2, 3, 4]. Although up to 40 genes have been reported to be associated with this disease, the Pro12Ala polymorphism of the peroxisome proliferator-activated receptor γ2 (PPAR-γ2) gene has been identified as the most widely reproduced genetic variation for the risk of type 2 diabetes [4]. Another important association with type 2 diabetes has been reported for a missense variant (Gly482Ser) in the peroxisome proliferator-activated receptor γ coactivator-1 (PGC-1α) gene [4].
PPARγ is a ligand-activated transcription factor, a member of the nuclear hormone receptor superfamily, that functions as a heterodimer with a retinoid X receptor (RXR) to promote transcription of numerous target genes [5, 6]. PPAR-γ2, an isoform of PPAR-γ with 28 additional amino acids at its N-terminus, is expressed almost exclusively in adipose tissue [7]. It plays a key role in adipogenesis [8, 9, 10, 11], is involved in the regulation of insulin sensitivity [12, 13], and is the major functional receptor for the thiazolidinedione class of insulin-sensitising drugs [11, 14]. Therefore, the PPAR-γ gene has been viewed as a “thrifty gene”, with an important role in the development of type 2 diabetes and diabetes-related traits [7, 15]. Additionally, the Pro12Ala substitution in exon B of the PPAR-γ2 gene, first reported in Caucasians [16], has been associated with diabetes mellitus [17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28]. Although not all associations have been consistent, a meta-analysis of published studies has confirmed a modest (1.25-fold), but statistically significant, increase in diabetes risk for the Pro12Pro genotype [4, 19].
PGC-1 co-activates a series of nuclear receptors including PPAR-γ, and controls transcription of genes involved in adaptive thermogenesis, adipogenesis and oxidative metabolism [29, 30, 31]. Moreover, PGC-1α regulates the determination of muscle fibre type [32], enhances glucose uptake by controlling insulin-sensitive glucose transporter (GLUT-4) expression in muscle cells [33] and is implicated in hepatic gluconeogenesis by increasing gene transcription of phosphoenolpyruvate carboxykinase and glucose-6-phosphatase [34]. Genes involved in oxidative metabolism and responsive to PGC-1α, as well as PGC-1α itself, have been showed to be co-ordinately down-regulated in diabetic subjects [35, 36] and even in insulin-resistant individuals [37]. The Gly482Ser variant in the PGC-1α gene has been reported to be associated with type 2 diabetes in Danish [38] and Japanese [39] subjects. In contrast, no association was found in French Caucasians [40] or in Pima Indians [41] and in additon, no interaction was observed between this variant and the Pro12Ala polymorphism of the PPAR-γ2 gene [38].
We investigated the association of the Pro12Ala polymorphism of the PPAR-γ2 gene, and the Gly482Ser variant of the PGC-1α gene with the risk of type 2 diabetes among the participants in the Study To Prevent Non Insulin Dependent Diabetes Mellitus (STOP-NIDDM).
Materials and methods
Study population and design
The STOP-NIDDM trial design and rationale have previously been described in detail [42]. The aim of this study was to investigate the effect of α-glucosidase inhibitor acarbose on the prevention of type 2 diabetes in a population with IGT. This international, multicentre, double-blind, placebo-controlled trial, conducted in Canada, Germany, Austria, Finland, Sweden, Norway, Denmark, Israel and Spain randomised 1429 subjects with fasting plasma glucose 5.6–7.7 mmol/l and 2-h plasma glucose 7.8–11.0 mmol/l to either the acarbose or placebo group.
All patients met with a dietician before randomisation and then on a yearly basis, and were recommended to follow a weight-reduction or weight-maintenance diet and encouraged to exercise regularly. Fasting plasma glucose (FPG) was measured every 3 months and a 2-h glucose tolerance test was performed if FPG levels were ≥7 mmol/l. All subjects underwent annual OGTT to evaluate the conversion to diabetes according to the World Health Organization criteria [43]. Improvement of glucose tolerance (i.e. return to normal glucose tolerance (NGT), either from IGT or from diabetes) was also assessed. Mean follow-up time for the whole population was 3.3±1.2 years.
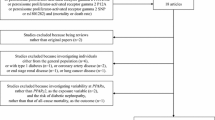
DNA was available from 770 subjects (387 men and 383 women), 356 of whom were initially allocated to acarbose and 414 to placebo. Their mean body mass index (BMI) was 30.8±4.1 kg/m2 and their mean age was 54.7±7.9 years. DNA was not available for subjects recruited in Israel and Sweden. Subjects who were included in the study did not differ from those whose DNA was not available with respect to sex and age, baseline characteristics such as weight, BMI, waist circumference and waist-to-hip ratio and laboratory measures such as fasting and 2-h glucose and insulin. However, those subjects whose DNA was available, had a higher systolic blood pressure and a significantly higher incidence of diabetes (40.3 vs 32.8%, p=0.004) compared to those whose DNA was not available. The incidence of diabetes was higher among subjects whose DNA was available compared to subjects whose DNA was not available for all countries with the exception of Denmark and Germany. All participants signed an informed consent form, approved by appropriate Institutional Review Boards.
Measurements
Anthropometric measurements, nutritional evaluations and laboratory analyses were carried out at baseline, at annual visits and at the end of the study, as previously reported [42, 44]. Homeostasis model assessment for insulin resistance (HOMA-IR) was calculated according to the formula: fasting plasma glucose (mmol/l) × fasting serum insulin (mU/l)/22.5 [45].
Genomic DNA was isolated from human leukocytes by the salt-precipitation method. Genotyping of the Gly482Ser polymorphism of the PGC-1α gene was performed with the polymerase chain reaction–restriction fragment length polymorphism (PCR-RFLP) method. The sequences of the primers were 5′-TGC TAC CTG AGA GAG ACT TTG-3′ (forward primer) and 5′-CTT TCA TCT TCG CTG TCA TC-3′ (reverse primer). PCR amplification was carried out in a volume of 10 µl, that contained 50 ng of genomic DNA, 5 pmol of each primer, 10 mmol/l Tris-HCl (pH 8.8), 50 mmol/l KCl, 1.5 mmol/l of MgCl2, 0.1% Triton X-100, 112 µmol/l dNTP and 0.25 U of DNA polymerase (Dynazyme DNA polymerase, Finnzymes, Espoo, Finland). Reaction mixtures were incubated at 94°C for 4 min, followed by 35 cycles of denaturation at 94°C for 30 s, annealing at 56°C for 30 s and extension at 72°C for 30 s, with the final extension at 72° for 6 min, and 260-bp length PCR products were then digested with Hpa II at 37°C overnight, resolved by electrophoresis on 9% polyacrylamide gel, and visualised by staining with ethidium bromide.
The Pro12Ala polymorphism of the PPAR-γ2 gene was detected by polymerase chain reaction–single-strand conformation polymorphism (PCR-SSCP) analysis as previously described [17]. The 167-bp length product, encompassing the polymorphic site was amplified by PCR with the sense primer 5′-GAC AAA ATA TCA GTG TGA ATT ACA GC-3′ and the antisense primer 5′-CCC AAT AGC CGT ATC TGG AAG G-3′. Amplification was performed using 50 ng of DNA in a total volume of 6 µl containing 2.8 pmol of each primer, 10 mmol/l Tris-HCl (pH 8.8), 50 mmol/l KCl, 1.5 mmol/l of MgCl2, 0.1% Triton X-100, 95 µmol/l dNTP, 0.14 U DNA polymerase (Dynazyme DNA polymerase, Finnzymes, Espoo, Finland), and 0.25 µCi [α-33]dCTP. The cycling programme was denaturation step at 94°C for 4 min, followed by 35 cycles of denaturation at 94°C for 30 s, annealing and extension at 66°C for 1 min, with the final extension at 72°C for 6 min. Thereafter, PCR products were diluted 4-fold with 0.1% SDS and 10 mmol/l EDTA and the loading mix (95% formamide, 20 mmol/l EDTA, 0.05% bromphenol blue, 0.05% xylene cyanol) was then added (1:1). After denaturation at 94°C for 4 min, the samples were placed on ice and 4 µl of each was loaded onto non-denaturating 6% acrylamide gels. Electrophoresis was carried out at 38°C for approximately 5 h, the gels were subsequently dried and autoradiographed overnight.
Statistical analysis
All statistical analyses were undertaken using the Statistical Package for Social Sciences (SPSS, Chicago, Ill., USA) version 11.0 for Windows. Data are expressed as either mean ± SD or percentages, unless indicated otherwise. The normality of the distribution of variables was tested with the Kolmogorov–Smirnov test, and parameters that did not have a normal distribution were logarithmically transformed (systolic and diastolic blood pressure, weight, BMI, fasting and 2-h plasma glucose and insulin). Comparison of variables between the genotype groups was carried out with the two-tailed Student’s t test or the Mann–Whitney non-parametric test, when appropriate. Categorical variables were compared using the chi square test. In order to evaluate whether the PGC-1α and PPAR-γ2 polymorphisms and other variables predicted the development of type 2 diabetes, odds ratios and 95% CIs (non-adjusted and adjusted for confounding variables) were calculated by logistic regression analysis. A p-value equal to or less than 0.05 was considered to be statistically significant.
Results
In 770 study subjects the frequencies of genotypes were as follows: 592 (76.9%) Pro12Pro, 164 (21.3%) Pro12Ala and 14 (1.8%) Ala12Ala for the PPAR-γ2 gene and 334 (43.4%) Gly482Gly, 339 (44.0%) Gly482Ser and 97 (12.6%) Ser482Ser for the PGC-1α gene. The frequencies of the 12Ala allele ranged from 0.186 to 0.307 and of the 482Ser allele from 0.498 to 0.780 in different countries (Austria was excluded because of a low number of cases). No differences in the frequencies of these polymorphisms were found between the acarbose and placebo groups and all genotypic distributions were in Hardy–Weinberg equilibrium.
Clinical characteristics, fasting and 2-h plasma glucose, fasting and 2-h serum insulin, HOMA IR and lipid levels at baseline did not differ significantly in relation to the Pro12Ala polymorphism of the PPAR-γ2 gene or the Gly482Ser polymorphism of the PGC-1α gene either in the entire study population (Table 1) or within the acarbose and placebo groups (data not shown). Carriers of the 12Ala allele showed a significantly higher reduction in 2-h serum insulin levels (p=0.035) compared to subjects with the Pro12Pro genotype. In the placebo group, carriers of the 482 Ser allele, compared to carriers of the Gly482Gly genotype, showed a significant increase in their 2-h glucose levels during the 3-year follow-up (0.66±2.81 vs 0.15±2.56 mmol/l, p=0.048) whereas carriers of the 482 Ser allele in the acarbose group showed a more pronounced decrease in their 2-h glucose levels compared to the 2-h glucose levels among carriers of the Gly482Gly genotype (−0.64±2.60 vs −0.25±2.58 mmol/l, p=0.131).
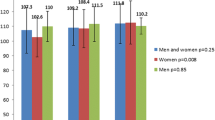
During the follow-up of 3.3 years, a total of 310 genotyped subjects (190 in the placebo group and 120 in the acarbose group) developed type 2 diabetes. In the placebo group four of eight subjects (50.0%) having the Ala 12Ala genotype, 37 of 85 subjects (43.5%) having the Pro12Ala genotype and 149 of 321 subjects (46.4%) having the Pro12Pro genotype of the PPAR-γ2 gene developed diabetes. In the acarbose group the corresponding numbers were one of six (16.7%), 22 of 79 (27.8%) and 97 of 271 (35.8%). In both treatment groups there was a trend for subjects with the Pro12Pro genotype to have a higher incidence of type 2 diabetes, but the difference was not statistically significant (p=0.673 in the placebo group and p=0.131 in the acarbose group; Fig. 1a). When the results were analysed by sex, the Pro12Pro genotype was associated with the conversion to diabetes in women treated with acarbose (p=0.014; Fig. 2).

Conversion (%) to type 2 diabetes in the placebo group and in the acarbose group in relation to the presence of the 12Ala allele (white bars) and the Pro12Pro genotype (black bars) of the PPAR-γ2 gene (a). Conversion (%) to type 2 diabetes in the placebo group and in the acarbose group in relation to the presence of the Gly482Gly genotype (white bars) and the 482Ser allele (black bars) of the PGC-1α gene (b)

Conversion (%) to type 2 diabetes in the placebo group and in the acarbose group in men (a), and conversion (%) to type 2 diabetes in the placebo group and in the acarbose group in women (b) according to the presence of the 12Ala allele (white bars) and the Pro12Pro genotype (black bars) of the PPAR-γ2 gene
In the placebo group 73 of 184 subjects (39.7%) with the Gly482Gly genotype, 96 of 178 subjects (53.9%) with the Gly482Ser genotype and the 21 of 52 subjects (40.4%) with the Ser482Ser genotype of the PGC-1α gene developed diabetes (p=0.017 over the three genotype groups). In the acarbose group the corresponding numbers were 57 of 150 subjects (38.0%), 51 of 161 subjects (31.7%), and 12 of 45 subjects (26.7%). In the placebo group the 482Ser allele of the PGC-1α gene, compared to the Gly482Gly genotype, was associated with a higher incidence of diabetes (p=0.023; Fig. 1b). The association in the placebo group was even more marked among men (p=0.012), as 36.4% of those (36 of 99) having the Gly482Gly genotype and 53.2% of those (66 of 124) with the 482Ser allele converted to diabetes. As shown in Table 2, acarbose was effective in the prevention of diabetes independently of the genotypes of the PPAR-γ2 gene in all subjects, but if analysed by sex, women with the 12Ala allele were more responsive to treatment with acarbose than men. In contrast, acarbose treatment prevented the development of diabetes only among carriers of the 482Ser allele of the PGC-1α gene in both men and women. There was no difference in weight change with respect to the polymorphisms of the PPAR-γ2 or PGC-1α genes among the different treatment groups or according to sex (data not shown).
Univariate logistic regression analysis showed that the Pro12Pro genotype of the PPAR-γ2 gene was not associated with a higher risk of developing type 2 diabetes in the placebo group or in the acarbose group (Table 3, Model 1). However, in women the presence of the Pro12Pro genotype was related to a 2.9-fold higher risk (95% confidence intervals (CI) 1.20 to 6.96; p=0.018) of developing diabetes in the acarbose group (Table 4). Adjustment for age and smoking (odds ratio (OR) 2.87, 95% CI 1.19 to 6.93; p=0.019), or for age, smoking and the country of origin (OR 2.90, 95% CI 1.17 to 7.20; p=0.022) or for age, weight at baseline and weight change (Table 4, Model 4, OR 3.55, 95% CI 1.38 to 9.13; p=0.009) did not essentially change the results.
No statistically significant gene–gene interaction was found between the PPAR-γ2 and PGC-1α genes (p=0.562). However, the 482Ser allele of the PGC-1α had a significant interaction (interaction term: PGC-1α/482Ser allele × treatment group) with the mode of the treatment (p=0.012). In the placebo group subjects with the 482Ser allele had an approximate 1.6-fold increase (95% CI 1.06 to 2.33, p=0.023) in the risk of developing diabetes (Table 3, Model 2). The results remained essentially unchanged after adjustment for age, sex and smoking (OR 1.59, 95% CI 1.07 to 2.36; p=0.021), or for age, sex, smoking and the country of origin (OR 1.53, 95% CI 1.01 to 2.32; p=0.043), or for age, sex, weight at baseline and weight change (odds ratio 1.56, 95% CI 1.04 to 2.34; p=0.031).
The 12Ala allele of the PPAR-γ2 tended to be related to an increase in conversion to normal glucose tolerance (NGT) in both sexes, but the results were not statistically significant among the different treatment groups (data not shown).
Discussion
We have shown that the Pro12Pro genotype of the PPAR-γ2 gene and the 482Ser allele of the PGC-1α gene predicts the conversion from IGT to diabetes in the STOP-NIDDM trial. The Pro12Pro genotype of the PPAR-γ2 gene was associated with a 2.9-fold higher risk of developing diabetes compared to the 12Ala allele in women in the acarbose group (p=0.018), whereas the 482Ser allele of the PGC-1α gene predicted the conversion to diabetes in the placebo group (OR 1.57, p=0.023).
There is substantial evidence that PPAR-γ contributes to the risk for type 2 diabetes by influencing insulin sensitivity, insulin secretion and susceptibility to obesity [6]. The 12Ala allele of the PPAR-γ2 gene, that has been shown to have a decreased transcriptional activity, is also associated with improved insulin sensitivity and lower risk for diabetes [17]. This finding is in agreement with results from heterozygous PPAR-γ null mice exhibiting increased insulin sensitivity compared with wild-type mice [46]. The 12Ala allele was associated with a higher reduction in the 2-h serum insulin level, probably indicating an increase in insulin sensitivity. However, it cannot be excluded that a decrease in insulin levels could also be due to impaired insulin secretion, because the 12Ala allele has been associated with reduced insulin secretion capacity in previous studies [20, 47].
PPAR-γ plays a key role in adipocyte differentiation [10, 11], and can therefore influence body fat mass and obesity. In our study subjects, those with the 12Ala allele had a somewhat higher BMI at baseline, and tended to lose more weight. This finding is in accordance with our results from the Finnish Diabetes Prevention Study [48]. In that study, subjects belonging to the intervention group (lifestyle changes) and who had the Ala12 allele lost significantly more weight (and were protected from type 2 diabetes) than subjects with the Pro12Pro genotype, although in the control group the 12Ala allele did not confer protection against diabetes. In the present study, the effect of the Pro12Pro genotype in increasing the risk for diabetes was independent of baseline weight change and other confounding factors in women in the acarbose group, indicating that women possessing the Pro12Pro genotype were less responsive to acarbose treatment. This implies that the effect of acarbose treatment was modified by the Pro12Ala polymorphism.
Several mechanisms could explain why the Gly482Ser polymorphism of the PGC-1α gene regulates the conversion from IGT to diabetes. PGC-1α increases and coordinates the expression of different genes that stimulate mitochondrial biogenesis, adaptive thermogenesis, fibre-type switching [32], expression of GLUT-4 in skeletal muscle [33], and regulation of gluconeogenesis in the liver [34]. Thus, a reduction in the activity of PGC-1α, possibly also as a result of the Gly482Ser mutation, might lead to insulin resistance in skeletal muscle. Additionally, a quantitative trait linkage analysis in Pima Indians suggested a link between basal insulin concentrations and chromosome 4p15.1 [49] in cases where the PGC-1α gene has been mapped [50]. In the present study the Gly482Ser variant was not related to fasting and 2-h plasma glucose, serum insulin, or their changes, or to BMI and weight change. However, compared to the Gly482Gly genotype, the 482Ser allele was associated with a 1.6-fold higher risk for diabetes in the placebo group but not in the acarbose group. The 482Ser allele had a significant interaction with treatment and acarbose treatment was able to reduce the risk of diabetes particularly among carriers of the 482Ser allele.
Previous attempts to relate the Gly482Ser polymorphism to type 2 diabetes have shown an 1.34-fold increase in risk among Danish Caucasians [38] and a significant association among Japanese subjects [39]. In contrast, the 482Ser allele did not predict diabetes in French Caucasians or Pima Indians [40, 41]. These studies were carried out in single populations. Because several different populations were used in the STOP-NIDDM trial, our data provides strong evidence that the Gly482Ser polymorphism of the PGC-1α gene contributes to the risk of type 2 diabetes. In agreement with this, the reduced expression of PGC-1α in adipose tissue has been associated with insulin resistance [51]. Moreover, recent studies have reported that down-regulation of the PGC-1α gene and coordinated changes in other genes involved in oxidative phosphorylation in man are associated with IGT, diabetes mellitus [35] and insulin resistance [37].
The regulation of many important metabolic processes and energy homeostasis by the PGC-1α gene is achieved through a specific interaction with a variety of transcription factors and nuclear hormone receptors, including PPAR-γ2. Moreover, PGC-1α was first identified as a transcriptional co-activator for PPAR-γ [29]. Therefore, it is possible that polymorphisms in both of these genes might interact. In our study no statistically significant interaction which may lead to an increase in the conversion to type 2 diabetes was found between the polymorphisms of the PPAR-γ2 and PGC-1α genes, this is in accord with the results of a previous study among Danish subjects [38].
In summary, we have demonstrated that the Pro12Pro genotype of the PPAR-γ2 gene and the 482Ser allele of the PGC-1α gene predict the conversion from IGT to type 2 diabetes. Our study also shows that the interaction between drug treatment (acarbose) and genetic variation may be significant with respect to the conversion from impaired glucose tolerance to type 2 diabetes.
Abbreviations
- FPG:
-
fasting plasma glucose
- HOMA-IR:
-
homeostasis model assessment for insulin resistance
- PGC-1:
-
peroxisome proliferator-activated receptor γ coactivator-1
- PPAR:
-
peroxisome proliferator-activated receptor
- SSCP:
-
single-strand conformation polymorphism
- STOP-NIDDM:
-
Study To Prevent Non Insulin Dependent Diabetes Mellitus
References
Kahn CR, Vicent D, Doria A (1996) Genetics of non-insulin-dependent (type-II) diabetes mellitus. Annu Rev Med 47:509–531
Medici F, Hawa M, Ianari A, Pyke DA, Leslie RD (1999) Concordance rate for type II diabetes mellitus in monozygotic twins: actuarial analysis. Diabetologia 42:146–150
Lehtovirta M, Kaprio J, Forsblom C, Eriksson J, Tuomilehto J, Groop L (2000) Insulin sensitivity and insulin secretion in monozygotic and dizygotic twins. Diabetologia 43:285–293
Florez JC, Hirschhorn J, Altshuler D (2003) The inherited basis of diabetes mellitus: implications for the genetic analysis of complex traits. Annu Rev Genomics Hum Genet 4:257–291
Rosen ED, Spiegelman BM (2001) PPARgamma: a nuclear regulator of metabolism, differentiation, and cell growth. J Biol Chem 276:37731–37734
Gurnell M, Savage DB, Chatterjee VK, O’Rahilly S (2003) The metabolic syndrome: peroxisome proliferator-activated receptor gamma and its therapeutic modulation. J Clin Endocrinol Metab 88:2412–2421
Auwerx J (1999) PPARgamma, the ultimate thrifty gene. Diabetologia 42:1033–1049
Tontonoz P, Hu E, Graves RA, Budavari AI, Spiegelman BM (1994) mPPAR gamma 2: tissue-specific regulator of an adipocyte enhancer. Genes Dev 8:1224–1234
Tontonoz P, Hu E, Spiegelman BM (1994) Stimulation of adipogenesis in fibroblasts by PPAR gamma 2, a lipid-activated transcription factor. Cell 79:1147–1156
Rosen ED, Walkey CJ, Puigserver P, Spiegelman BM (2000) Transcriptional regulation of adipogenesis. Genes Dev 14:1293–1307
Spiegelman BM (1998) PPAR-gamma: adipogenic regulator and thiazolidinedione receptor. Diabetes 47:507–514
Yamauchi T, Kamon J, Waki H et al. (2001) The mechanisms by which both heterozygous peroxisome proliferator-activated receptor gamma (PPARgamma) deficiency and PPARgamma agonist improve insulin resistance. J Biol Chem 276:41245–41254
Picard F, Auwerx J (2002) PPAR(gamma) and glucose homeostasis. Annu Rev Nutr 22:167–197
Lehmann JM, Moore LB, Smith-Oliver TA, Wilkison WO, Willson TM, Kliewer SA (1995) An antidiabetic thiazolidinedione is a high affinity ligand for peroxisome proliferator-activated receptor gamma (PPAR gamma). J Biol Chem 270:12953–12956
Tenenbaum A, Fisman EZ, Motro M (2003) Metabolic syndrome and type 2 diabetes mellitus: focus on peroxisome proliferator activated receptors (PPAR). Cardiovasc Diabetol 2:14
Yen CJ, Beamer BA, Negri C et al. (1997) Molecular scanning of the human peroxisome proliferator activated receptor gamma (hPPAR gamma) gene in diabetic Caucasians: identification of a Pro12Ala PPAR gamma 2 missense mutation. Biochem Biophys Res Commun 241:270–274
Deeb SS, Fajas L, Nemoto M et al. (1998) A Pro12Ala substitution in PPARgamma2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nature Genet 20:284–287
Hara K, Okada T, Tobe K et al. (2000) The Pro12Ala polymorphism in PPAR gamma2 may confer resistance to type 2 diabetes. Biochem Biophys Res Commun 271:212–216
Altshuler D, Hirschhorn JN, Klannemark M et al. (2000) The common PPARgamma Pro12Ala polymorphism is associated with decreased risk of type 2 diabetes. Nature Genet 26:76–80
Mori H, Ikegami H, Kawaguchi Y et al. (2001) The Pro12→Ala substitution in PPAR-gamma is associated with resistance to development of diabetes in the general population: possible involvement in impairment of insulin secretion in individuals with type 2 diabetes. Diabetes 50:891–894
Douglas JA, Erdos MR, Watanabe RM et al. (2001) The peroxisome proliferator-activated receptor-gamma2 Pro12A1a variant: association with type 2 diabetes and trait differences. Diabetes 50:886–890
Memisoglu A, Hu FB, Hankinson SE et al. (2003) Prospective study of the association between the proline to alanine codon 12 polymorphism in the PPARgamma gene and type 2 diabetes. Diabetes Care 26:2915–2917
Ringel J, Engeli S, Distler A, Sharma AM (1999) Pro12Ala missense mutation of the peroxisome proliferator activated receptor gamma and diabetes mellitus. Biochem Biophys Res Commun 254:450–453
Mancini FP, Vaccaro O, Sabatino L et al. (1999) Pro12Ala substitution in the peroxisome proliferator-activated receptor-gamma2 is not associated with type 2 diabetes. Diabetes 48:1466–1468
Oh EY, Min KM, Chung JH et al. (2000) Significance of Pro12Ala mutation in peroxisome proliferator-activated receptor-gamma2 in Korean diabetic and obese subjects. J Clin Endocrinol Metab 85:1801–1804
Meirhaeghe A, Fajas L, Helbecque N et al. (2000) Impact of the Peroxisome Proliferator Activated Receptor gamma2 Pro12Ala polymorphism on adiposity, lipids and non-insulin-dependent diabetes mellitus. Int J Obes Relat Metab Disord 24:195–199
Clement K, Hercberg S, Passinge B et al. (2000) The Pro115Gln and Pro12Ala PPAR gamma gene mutations in obesity and type 2 diabetes. Int J Obes Relat Metab Disord 24:391–393
Lei HH, Chen MH, Yang WS et al. (2000) Peroxisome proliferator-activated receptor gamma 2 Pro12Ala gene variant is strongly associated with larger body mass in the Taiwanese. Metabolism 49:1267–1270
Puigserver P, Wu Z, Park CW, Graves R, Wright M, Spiegelman BM (1998) A cold-inducible coactivator of nuclear receptors linked to adaptive thermogenesis. Cell 92:829–839
Wu Z, Puigserver P, Andersson U et al. (1999) Mechanisms controlling mitochondrial biogenesis and respiration through the thermogenic coactivator PGC-1. Cell 98:115–124
Puigserver P, Spiegelman BM (2003) Peroxisome proliferator-activated receptor-gamma coactivator 1 alpha (PGC-1 alpha): transcriptional coactivator and metabolic regulator. Endocr Rev 24:78–90
Lin J, Wu H, Tarr PT et al. (2002) Transcriptional co-activator PGC-1 alpha drives the formation of slow-twitch muscle fibres. Nature 418:797–801
Michael LF, Wu Z, Cheatham RB et al. (2001) Restoration of insulin-sensitive glucose transporter (GLUT4) gene expression in muscle cells by the transcriptional coactivator PGC-1. Proc Natl Acad Sci USA 98:3820–3825
Yoon JC, Puigserver P, Chen G et al. (2001) Control of hepatic gluconeogenesis through the transcriptional coactivator PGC-1. Nature 413:131–138
Mootha VK, Lindgren CM, Eriksson KF et al. (2003) PGC-1alpha-responsive genes involved in oxidative phosphorylation are coordinately downregulated in human diabetes. Nature Genet 34:267–273
Attie AD, Kendziorski CM (2003) PGC-1alpha at the crossroads of type 2 diabetes. Nature Genet 34:244–245
Patti ME, Butte AJ, Crunkhorn S et al. (2003) Coordinated reduction of genes of oxidative metabolism in humans with insulin resistance and diabetes: potential role of PGC1 and NRF1. Proc Natl Acad Sci USA 100:8466–8471
Ek J, Andersen G, Urhammer SA, Gaede PH et al. (2001) Mutation analysis of peroxisome proliferator-activated receptor-gamma coactivator-1 (PGC-1) and relationships of identified amino acid polymorphisms to Type II diabetes mellitus. Diabetologia 44:2220–2226
Hara K, Tobe K, Okada T et al. (2002) A genetic variation in the PGC-1 gene could confer insulin resistance and susceptibility to Type II diabetes. Diabetologia 45:740–743
Lacquemant C, Chikri M, Boutin P, Samson C, Froguel P (2002) No association between the G482S polymorphism of the proliferator-activated receptor- gamma coactivator-1 (PGC-1) gene and Type II diabetes in French Caucasians. Diabetologia 45:602–603; author reply 604
Muller YL, Bogardus C, Pedersen O, Baier L (2003) A Gly482Ser missense mutation in the peroxisome proliferator-activated receptor gamma coactivator-1 is associated with altered lipid oxidation and early insulin secretion in Pima Indians. Diabetes 52:895–898
Chiasson JL, Gomis R, Hanefeld M, Josse RG, Karasik A, Laakso M (1998) The STOP-NIDDM Trial: an international study on the efficacy of an alpha-glucosidase inhibitor to prevent type 2 diabetes in a population with impaired glucose tolerance: rationale, design, and preliminary screening data. Study to Prevent Non-Insulin-Dependent Diabetes Mellitus. Diabetes Care 21:1720–1725
World Health Organization (1985) Diabetes mellitus. WHO, Geneva, pp 10–11
Chiasson JL, Josse RG, Gomis R, Hanefeld M, Karasik A, Laakso M (2002) Acarbose for prevention of type 2 diabetes mellitus: the STOP-NIDDM randomised trial. Lancet 359:2072–2077
Albareda M, Rodriguez-Espinosa J, Murugo M, Leiva A de, Corcoy R (2000) Assessment of insulin sensitivity and beta-cell function from measurements in the fasting state and during an oral glucose tolerance test. Diabetologia 43:1507–1511
Kubota N, Terauchi Y, Miki H et al. (1999) PPAR gamma mediates high-fat diet-induced adipocyte hypertrophy and insulin resistance. Mol Cell 4:597–609
Stefan N, Fritsche A, Haring H, Stumvoll M (2001) Effect of experimental elevation of free fatty acids on insulin secretion and insulin sensitivity in healthy carriers of the Pro12Ala polymorphism of the peroxisome proliferator-activated receptor-gamma2 gene. Diabetes 50:1143–1148
Lindi VI, Uusitupa MI, Lindström J, et al. for the Finnish Diabetes Prevention Study Group (2002) Association of the Pro12Ala polymorphism in the PPAR-gamma2 gene with 3-year incidence of type 2 diabetes and body weight change in the Finnish Diabetes Prevention Study. Diabetes 51:2581–2586
Pratley RE, Thompson DB, Prochazka M et al. (1998) An autosomal genomic scan for loci linked to prediabetic phenotypes in Pima Indians. J Clin Invest 101:1757–1764
Esterbauer H, Oberkofler H, Krempler F, Patsch W (1999) Human peroxisome proliferator activated receptor gamma coactivator 1 (PPARGC1) gene: cDNA sequence, genomic organization, chromosomal localization, and tissue expression. Genomics 62:98–102
Hammarstedt A, Jansson PA, Wesslau C, Yang X, Smith U (2003) Reduced expression of PGC-1 and insulin-signaling molecules in adipose tissue is associated with insulin resistance. Biochem Biophys Res Commun 301:578–582
Acknowledgements
The STOP-NIDDM trial and DNA analysis were funded by an unrestricted grant from Bayer AG. We thank Ms. Leena Uschanoff for genotyping.
Duality of interest
J.-L. Chiasson has received research support as well as an honorarium for lectures from Bayer.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
The members of the STOP-NIDDM Study Group are listed in a previous article published in the Lancet (2002; 359:2072–2077)
Rights and permissions
About this article
Cite this article
Andrulionytè, L., Zacharova, J., Chiasson, JL. et al. Common polymorphisms of the PPAR-γ2 (Pro12Ala) and PGC-1α (Gly482Ser) genes are associated with the conversion from impaired glucose tolerance to type 2 diabetes in the STOP-NIDDM trial. Diabetologia 47, 2176–2184 (2004). https://doi.org/10.1007/s00125-004-1577-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00125-004-1577-2