
Abstract
Purpose
To analyze the performance and quality of intraoperative radiation therapy (IORT) publications identified in medical databases during a recent period in terms of bibliographic metrics.
Materials and methods
A bibliometric search was conducted for IORT papers published in the PubMed database between 1997 and 2013. Publication rate was used as a quantity indicator; the 2012 Science Citation Index Impact Factor as a quality indicator. Furthermore, the publications were stratified in terms of study type, scientific topic reported, year of publication, tumor type and journal specialty. We performed a one-way analysis of variance (ANOVA) to determine differences between the means of the analyzed groups.
Results
Among the total of 207 journals, articles were reported significantly more frequently in surgery (n = 399, 41 %) and radiotherapy journals (n = 273, 28 %; p < 0.01). The highest impact factor was achieved by clinical oncology journals (p < 0.01). The majority of identified articles were retrospective cohort reports (n = 622, 64 %), followed by review articles (n = 204, 21 %; p < 0.001). Regarding primary topic, reports on cancer outcome following specific tumor therapy were most frequently published (n = 661, 68 %; p < 0.001) and gained the highest mean impact factor (p < 0.01). Gastrointestinal tumor reports were represented most frequently (n = 456, 47 %; p < 0.001) and the mean superior impact factor was earned by breast and gynecologic publications (p < 0.01).
Conclusion
We identified a consistent and sustained scientific productivity of international IORT expert groups. Most publications appeared in journals with surgical and radiooncological content. The highest impact factor was achieved by medical oncology journals.
Zusammenfassung
Ziel
Ziel war es, in Form von bibliographischen Metriken die wissenschaftliche Effizienz und Qualität von Publikationen über die Anwendung intraoperativer Strahlentherapie (IORT) zu analysieren, die in einer bestimmten Zeitspanne in medizinischen Datenbanken gefunden wurden.
Material und Methoden
Es wurde eine bibliometrische Suche nach IORT-Publikationen vorgenommen, die in der Pubmed-Datenbank zwischen 1997 und 2013 veröffentlicht wurden. Als Mengenindikator verwendeten wir die Publikationsrate und als Qualitätsindikator den „2012 Citations Index Impact Factor“. Die Arbeiten wurden außerdem geordnet nach Studientyp, wissenschaftlichem Fokus, Tumorentität, Art der Zeitschrift sowie Erscheinungsjahr. Um die Unterschiede zwischen den Mittelwerten der untersuchten Gruppen zu bestimmen, wurde eine Einwegvarianzanalyse (ANOVA) durchgeführt.
Ergebnisse
Von insgesamt 207 Fachzeitschriften wurde signifikant häufiger in jenen der Chirurgie (n = 399; 41 %) und der Strahlentherapie (n = 273; 28 %; p < 0,01) publiziert, wobei der höchste Impactfaktor in Fachjournalen der klinischen Onkologie erzielt wurde (p < 0,01). Die meisten Veröffentlichungen bezogen sich auf retrospektive Kohortenstudien (n = 622; 64 %), gefolgt von Übersichtsarbeiten (n = 204; 21 %; p < 0,001). Zu klinischen Ergebnissen nach spezifischer Tumortherapie erschienen im Vergleich zu anderen Themen die zahlreichsten Arbeiten (n = 661; 68 %, p < 0,001); hier wurde auch der höchste mittlere Impactfaktor erreicht (p < 0,01). Am häufigsten fanden sich Veröffentlichungen über gastrointestinale Tumoren (n = 456; 47 %; p < 0,001); im Bereich gynäkologischer Tumoren und Mammakarzinome wurde dagegen der höchste mittlere Impactfaktor erzielt (p < 0,01).
Schlussfolgerung
Es war festzustellen, dass die wissenschaftliche Produktivität internationaler IORT-Expertengruppen beständig und nachhaltig ist. Die meisten Veröffentlichungen erschienen in chirurgischen und radioonkologischen Fachzeitschriften. Der höchste Impactfaktor wurde in Fachzeitschriften mit internistisch-onkologischer Ausrichtung erzielt.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Intraoperative radiotherapy (IORT) is widely used in all continents to deliver precise radiotherapy at the time of cancer surgery [1]. Initial pioneering experiences in Japan and the USA were documented in the late 1970s and since then, a significant body of knowledge on methodology, result analysis in terms of cancer site and development projects has become available in the medical literature [2–4].
Systematic literature reviews of IORT studies have documented feasibility, tolerability and high local control promotion using IORT as a boost component of escalated radiotherapy; including similar specific results for primary rectal, recurrent rectal and pancreatic cancer [5–7]. Overviews and editorials on IORT practice and results have identified technological diversity among the procedures performed (electron beams, kilovoltage X-rays and brachytherapy with isotopes) and consistent methodology in terms of reporting clinical results emphasizing local control and toxicity [1]. Expert IORT institutions have demonstrated particular commitment to evaluating clinical outcomes observed in cancer location- or type-oriented IORT-containing treatment approaches [8]. Nevertheless, evaluating scientific quality is a difficult problem to which there is no standard solution. Prior to publication, experts in a specific field estimate the importance and relevance of scientific articles (peer review; [9]). Alternative methods (statistical and mathematical data), such as citation rates and journal impact factors, measure the quantity and performance (i.e. quality) of published science, as well as the connectivity between scientific fields, research departments or authors [10].
In terms of the bibliographic metrics found in medical databases during a recent period, this paper focuses on an extensive analysis of the available literature reporting IORT data. This information provides authors and editorial journals with a reflection of the preferences and policies relating to the transfer of scientific knowledge generated in studies with IORT as a cancer treatment modality.
Materials and methods
We reviewed the publication pattern of scientific journal articles and analyzed the bibliometry of IORT-related papers published in PubMed during a certain time period. As a quantity indicator, we used the number of articles published in PubMed between 1997 and 2013. As a quality indicator, we used the 2012 Science Citation Index Impact Factor in order to evaluate the impact of the research on the scientific community. Furthermore, we stratified the identified publications by study type, scientific topic reported, tumor site, journal specialty and the year of publication.
Statistical analysis
We performed a one-way analysis of variance (ANOVA) to determine any significant differences between the means of the analyzed groups. In order to determine which specific group was significantly different from the others we performed a post-hoc test (Tukey’s test).
Results
Between 1997 and 2012, a total of 972 journal papers from 534 different first authors (281 different institutions from 32 countries) were published in the PubMed database (mean journal impact factor of 2.73, standard deviation ± 2.62).
Study type
The majority of articles identified are retrospective cohort reports (n = 622, 64 %), followed by review articles (n = 204, 21 %; p < 0.001). Only 6 % (n = 55) of the reported articles are phase II-III trials. The highest mean impact factor was related to prospective publications (p < 0.001; ◉ Fig. 1a).

Publication quantity (total rate; solid bars) and quality (journal Impact factor; black line) stratified by a study type and b journal specialty
Journal specialty
From a total of 207 journals, IORT articles were significantly more frequently reported in surgery (n = 399, 41 %) and radiotherapy journals (n = 273, 28 %; p < 0.01). The highest impact factor was achieved by radiotherapy and medical oncology journals (p < 0.01; ◉ Fig. 1b).
Primary scientific topic
Clinical cancer outcome reports represented the most frequently published primary topic (n = 661, 68 %; p < 0.001). Clinical reports and technology were associated with the highest mean impact factor (p < 0.01; ◉ Fig. 2a).

Publication quantity (total rate; solid bars) and quality (journal impact factor; black line) stratified by a primary topic and b tumor site
Tumor sites
Gastrointestinal tumor reports were most frequent (n = 456, 47 %; p < 0.001). The mean superior impact factor was related to breast and gynecologic cancer publications (p < 0.01; ◉ Fig. 2b). Of the 28 tumor sites reported, the most commonly mentioned sites were breast (n = 191, 19.7 %) pancreatic (n = 183, 18.8 %) and colorectal cancer (n = 179, 18.4 %).
Year of publication
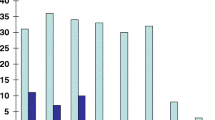
The year of highest productivity was 1997 (n = 102, 11 %; p < 0.001) and the year with the highest mean impact factor was 2008 (p < 0.001; ◉ Fig. 3).

Publication quantity (total rate; solid bars) and quality (journal impact factor; black line) stratified by year of publication
Discussion
Used either alone or in combination, specialized radiotherapy techniques are developed to improve the therapeutic index of conventional cancer therapies [11]. Brachytherapy, radiosurgery, intensity-modulated radiotherapy (IMRT) and image-guided radiotherapy (IGRT) are all examples of radiation technology-driven developments aimed at assuring high cancer local control rates while minimizing toxicity [12].
Bibliometrics is a set of methods (statistical and mathematical) generally used to measure and analyze the quantity and quality of articles and publications [10]. Quantity indicators measure the productivity of a particular researcher: in the present analysis, we have used the simplest method available to asses this (i.e. the number of articles published in PubMed). Although this count is a very straightforward indicator that can be easily calculated, one must be very careful when using it to compare different groups. While the number of publications does reflect productivity, it does not address the quality of the articles [10]. By analyzing the article methodology, this limitation can potentially be overcome (the impact of a case report is obviously not equivalent to that of a multicenter randomized controlled clinical trial). Additionally, the number of publications is also influenced by cohort size [10]. Beyond productivity, the level of quality of the publication can be identified by using performance indicators [10]. In the present analysis we used the Journal Citation Index Impact Factor as a surrogate measure of quality.
Bibliometrics of highly specialized radiotherapy techniques have never been reported; either because they have evolved into the development of a specific journal devoted to this particular scientific area (brachytherapy or radiosurgery), or because the information was spread due to its multispecialty nature (IORT). The evaluation of metrics for cancer treatment techniques is relevant to understanding the patterns of medical practice result reporting, as well as to evaluating the sensitivity of the peer review system within the broad spectrum of oncology journals.
The main findings of the present analysis of metrics in IORT publications during the period 1997–2013 are: the limited availability of phase III trials specific to IORT [2]; the balanced reporting of IORT data in surgical- and radiation oncology-based journals; the progressive incremental increase in impact factor over time and the increasing tendency to report data from early-stage breast cancer studies [13, 14]. Additionally, the fact that IORT is a cancer treatment modality able to contribute with competitive results for a variety of cancer sites and histological types is extensively documented; with most reports published in the first quartile of the specific specialty journals. Due to the retrospective nature of IORT clinical reports, it is identified that the relevance of editorial interest in the published data is related to the potency of the analysis performed (number of patients and long-term follow-up maturation; [10]).
Pooled analysis strategies for interinstitutional data sharing and reporting have found a particularly positive status in terms of the quality of their metrics [11, 14]. This effect on interinstitutional pooled analyses has recently been confirmed in soft tissue and renal cancer models [12, 16, 17].
Nonrandomized surgical and radiotherapeutic clinical cancer control results have an intrinsic limitation to the attainment of metric publication standards. This fact affects the discrimination of knowledge. Additionally, local cancer therapies have methodological and intrinsic restrictions in terms of generating hypotheses to be tested in randomized oncology trials. This fact contributes to the marginal success of designed and completed randomized trials for IMRT/IGRT, brachytherapy and radiosurgery.
Designed IORT trials employing dose-escalation strategies and using radiotherapy precision techniques have indicated that improved cancer control with equivalent normal tissue toxicity is a realistic scenario [2]. Reports are consistent with improved promotion of local control in pancreatic [18], gastric [19] and gastroesophageal cancer [20], as well as in locally advanced [21, 22] and locally recurrent rectal cancer [23]; while decreased normal tissue toxicity (severe enteritis) has been proven in the retroperitoneal sarcoma model [24].
New hypotheses have also been tested with IORT in studies searching for noninferiority or equivalence of outcomes using single-fraction IORT compared to conventional radiotherapy in early stage breast cancer [13, 14]. Results are questionable regardless of the technology employed (electrons or kilovoltage X-rays).
Finally, of relevant potential for the understanding and reporting of IORT contributions to combined cancer management is the analysis of risk factors associated with local relapse and identification of the effect of adverse features such as close or positive surgical margins, multiple involved surgical specimens, extensive nodal involvement, radioresistant disease, etc. The cancer models including this kind of analysis in IORT-containing radiosurgical strategies are oligorecurrence [17, 23–26] and resectable pancreatic cancer [18]. Technical reports of IORT implementation involving physical science developments (e.g. in vivo dosimetry or quality assurance; [3]), treatment planning modified for surgical features and radiation equipment design are scarce in the medical literature and, with occasional exceptions, published in the latter quartiles of impact-factor rated specialty journals [27].
Conclusion
We identified a consistent and sustained scientific productivity of international IORT expert groups. Journals with surgical and radiooncological content showed the dominant publication frequency [28–30].The highest impact factor was achieved by medical oncology-based journals. Quantity and quality indicators could potentially help researchers to select the journals to which they submit their manuscripts and organizations to make decisions regarding appointments, promotions and funding of particular research, individual researchers or a research group. Moreover, they could help to determine the geographic origin of research and detect growth of a country’s scientific impact. These indicators could also help to measure research focus, detect misallocation of resources, predict research success and orient research funding to optimize support of research policy.
References
Debenham BJ, Hu KS, Harrison LB (2013) Present status and future directions of intraoperative radiotherapy. Lancet Oncol 14:457–464
Gunderson LL, Willet CG, Calvo FA, Harrison LB (2011) Intraoperative irradiation techniques and results. Current Clinical Oncology, 2 edition. Humana, New York, pp 27–50
Calvo FA, Sole CV, González ME, Tangco ED, López-Tarjuelo J, Koubychine I et al (2013) Research opportunities in intraoperative radiation therapy: the next decade 2013–2023. Clin Transl Oncol 15:683–690
Krengli M, Calvo FA, Sedlmayer F, Sole CV, Fastner G, Alessandro M et al (2013) Clinical and technical characteristics of intraoperative radiotherapy. Analysis of the ISIORT-Europe database. Strahlenther Onkol 189:729–737
Mirnezami R, Chang GJ, Das P, Chandrakumaran K, Tekkis P, Darzi A et al (2013) Intraoperative radiotherapy in colorectal cancer: systematic review and meta-analysis of techniques, long-term outcomes, and complications. Surg Oncol 22:22–35
Cantero-Muñoz P, Urién MA, Ruano-Ravina A (2011) Efficacy and safety of intraoperative radiotherapy in colorectal cancer: a systematic review. Cancer Lett 306:121–133
Skandarajah AR, Lynch AC, Mackay JR, Ngan S, Heriot AG (2009) The role of intraoperative radiotherapy in solid tumors. Ann Surg Oncol 16:735–744
Gunderson LL, Ashman JB, Haddock MG, Petersen IA, Moss A, Heppell J et al (2013) Integration of radiation oncology with surgery as combined-modality treatment. Surg Oncol Clin N Am 22:405–432
Whitehouse GH (2001) Citation rates and impact factors: should they matter? Br J Radiol 74:1–3
Durieux V, Gevenois PA (2010) Bibliometric indicators: quality measurements of scientific publication. Radiology 255:342–351
Kusters M, Valentini V, Calvo FA, Krempien R, Nieuwenhuijzen GA, Martijn H et al (2010) Results of European pooled analysis of IORT-containing multimodality treatment for locally advanced rectal cancer: adjuvant chemotherapy prevents local recurrence rather than distant metastases. Ann Oncol 21:1279–1284
Paly JJ, Hallemeier CL, Biggs PJ, Niemierko A, Roeder F, Martínez-Monge R et al (2014) Outcomes in a Multi-institutional cohort of patients treated with intraoperative radiation therapy for advanced or recurrent renal cell carcinoma. Int J Radiat Oncol Biol Phys. doi: 10.1016/j.ijrobp.2013.11.207
Veronesi U, Orecchia R, Maisonneuve P, Viale G, Rotmensz N, Sangalli C et al (2013) Intraoperative radiotherapy versus external radiotherapy for early breast cancer (ELIOT): a randomised controlled equivalence trial. Lancet Oncol 14:1269–1277
Vaidya JS, Wenz F, Bulsara M, Tobias JS, Joseph DJ, Keshtgar M et al (2013) Risk adapted targeted intraoperative radiotherapy versus whole-breast radiotherapy for breast cancer: 5-year results for local control and overall survival from the TARGIT-A randomised trial. Lancet 13:61950–61959
Valentini V, Calvo F, Reni M, Krempien R, Sedlmayer F, Buchler MW et al (2009) Intra-operative radiotherapy (IORT) in pancreatic cancer: joint analysis of the ISIORT Europe experience. Radiother Oncol 91:54–59
Calvo FA, Sole CV, Martinez-Monge R, Azinovic I, Aristu J, Zudaire J et al (2013) Intraoperative EBRT and resection for renal cell carcinoma: twenty-year outcomes. Strahlenther Onkol 189:129–136
Calvo FA, Sole CV, Cambeiro M, Montero A, Polo A, Gonzalez C et al (2014) Prognostic value of external beam radiation therapy in patients treated with surgical resection and intraoperative electron beam radiation therapy for locally recurrent soft tissue sarcoma: a multicentric long-term outcome analysis. Int J Radiat Oncol Biol Phys 88:143–150
Calvo FA, Sole CV, Atahualpa F, Lozano MA, Gomez-Espi M, Calin A et al (2013) Chemoradiation for resected pancreatic adenocarcinoma with or without intraoperative radiation therapy boost: long-term outcomes. Pancreatology 13:576–582
Calvo FA, Sole CV, Obregón R, Gómez-Espí M, González-San Segundo C, González-Bayón L et al (2013) Intraoperative radiotherapy for the treatment of resectable locally advanced gastric adenocarcinoma: topography of locoregional recurrences and long-term outcomes. Clin Transl Oncol 15:443–449
Calvo FA, Sole CV, Obregón R, Gómez-Espí M, Lozano MA, Gonzalez-Bayon L et al (2013) Postchemoradiation resected locally advanced esophageal and gastroesophageal junction carcinoma: long-term outcome with or without intraoperative radiotherapy. Ann Surg Oncol 20:1962–1969
Calvo FA, Sole CV, Serrano J, Del Valle E, Rodriguez M, Muñoz-Calero A et al (2014) Preoperative chemoradiation with or without induction oxaliplatin plus 5-fluorouracil in locally advanced rectal cancer: Long-term outcome analysis. Strahlenther Onkol 190:149–157
Calvo FA, Sole CV, Serrano J, Rodriguez M, Marcos F, Muñoz-Calero A et al (2013) Postchemoradiation laparoscopic resection and intraoperative electron-beam radiation boost in locally advanced rectal cancer: long-term outcomes. J Cancer Res Clin Oncol 139:1825–1833
Calvo FA, Sole CV, Alvarez deSP, Gómez-Espí M, Blanco J, Lozano MA et al (2013) Prognostic impact of external beam radiation therapy in patients treated with and without extended surgery and intraoperative electrons for locally recurrent rectal cancer: 16-year experience in a single institution. Int J Radiat Oncol Biol Phys 86:892–900
Sindelar WF, Kinsella TJ, Chen PW et al (1993) Intraoperative radiotherapy in retroperitoneal sarcomas. Final results of a aprospective randomized clinical trial. Arch Surg 128:402–410
Sole CV, Calvo FA, Lozano MA, Gonzalez-Bayon L, Gonzalez-Sansegundo C, Alvarez A et al (2014) External-beam radiation therapy after surgical resection and intraoperative electron-beam radiation therapy for oligorecurrent gynecological cancer: Long-term outcome. Strahlenther Onkol. doi: 10.1007/s00066-013-0472-5
Calvo FA, Sole CV, Lozano MA, Gonzalez-Bayon L, Gonzalez-Sansegundo C, Alvarez A et al (2013) Intraoperative electron beam radiotherapy and extended surgical resection for gynecological pelvic recurrent malignancies with and without external beam radiation therapy: long-term outcomes. Gynecol Oncol 130:537–544
Pascau J, Santos Miranda JA, Calvo FA, Bouché A, Morillo V, González-San Segundo C et al (2012) An innovative tool for intraoperative electron beam radiotherapy simulation and planning: description and initial evaluation by radiation oncologists. Int J Radiat Oncol Biol Phys 83:e287–e295
Calvo FA, Sole CV, Polo A, Cambeiro M, Montero A, Alvarez A et al (2014) Limb-sparing management with surgical resection, external-beam and intraoperative electron-beam radiation therapy boost for patients with primary soft tissue sarcoma of the extremity: a multicentric pooled analysis of long-term outcomes. Strahlenther Onkol. 2014 Apr 9. (Epub ahead of print)
Sole CV, Calvo FA, de Sierra PA, Herranz R, Gonzalez-Bayon L, García-Sabrido JL (2014) Multidisciplinary therapy for patients with locally oligo-recurrent pelvic malignancies. J Cancer Res Clin Oncol. 2014 Apr 10. (Epub ahead of print)
Sole CV, Calvo FA, Cambeiro M, Polo A, Montero A, Hernanz R et al (2014) Intraoperative radiotherapy-containing multidisciplinary management of trunk-wall soft-tissue sarcomas. Clin Transl Oncol. 2014 Jan 31. (Epub ahead of print)
Compliance with ethical guidelines
Conflict of interest. Supported in part by a grant from the Health Institute of Research Carlos III, Spanish Ministry of Science and Innovation (project code PI11-02908). C.V. Sole, F.A. Calvo, C. Ferrer, J. Pascau and H. Marsiglia state that there are no conflicts of interest. The accompanying manuscript does not include studies on humans or animals.
Author information
Authors and Affiliations
Rights and permissions
About this article

Cite this article
Sole, C., Calvo, F., Ferrer, C. et al. Bibliometrics of intraoperative radiotherapy. Strahlenther Onkol 190, 1111–1116 (2014). https://doi.org/10.1007/s00066-014-0695-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-014-0695-0