
Abstract
Objectives
The aim of this study was to evaluate the characteristics affecting different intensities of mandibular asymmetry in skeletal Class II adults using three-dimensional images. This study is clinically relevant since it allows professionals to evaluate the morphological components related to these deformities and more carefully obtain correct diagnosis and treatment plan for such patients.
Methods
Cone-beam computed tomography data of 120 Class II patients (40 with relative symmetry, 40 with moderate asymmetry, and 40 with severe asymmetry) were imported to SimPlant Ortho Pro® 2.0 software (Dental Materialise, Leuven, Belgium). Three reference planes were established and linear measurements were performed from specific landmarks to these planes, comparing the deviated side and the contralateral side in each group, as well as the differences between groups. The correlation between midline mandibular asymmetry and other variables was also evaluated. Statistical analyses considered a significance level of 5%.
Results
Comparing the values obtained on the deviated side and on the contralateral side, there were significant differences for patients with moderate asymmetry and severe asymmetry. However, differences were seen more often in severe mandibular asymmetries. In those patients, there was a significant correlation of the gnathion deviation with lower dental midline deviation, difference in the lateral gonion positions, difference in the mandibular rami heights, and difference in the jugale vertical displacements.
Conclusions
For skeletal Class II patients with mandibular asymmetry, some craniofacial features are related to chin deviation and require proper evaluation, including the bilateral differences in the ramus height, mandibular body length, transverse and vertical positioning of the gonion and jugale points.
Zusammenfassung
Ziele
In der Studie sollten mittels dreidimensionaler Bildgebung die Charakteristika evaluiert werden, welche die unterschiedlich starke Ausprägung von Unterkieferasymmetrien bei erwachsenen Klasse-II-Patienten beeinflussen. Die klinische Relevanz der Untersuchung besteht darin, dass sie die Möglichkeit bietet, mit diesen Deformitäten verbundene morphologische Komponenten zu evaluieren und auf sorgfältigere Weise sowohl die zutreffende Diagnose zu stellen als auch die Behandlung zu planen.
Methoden
Daten der digitalen Volumentomographien (DVT) von 120 Klasse-II-Patienten (40 mit relativer Symmetrie sowie 40 mit mäßiger und 40 mit ausgeprägter Asymmetrie) wurden in die Software SimPlant Ortho Pro® 2.0 (Dental Materialise, Leuven, Belgien) importiert. Anhand von 3 definierten Bezugsebenen und spezifischen Referenzpunkten wurden Messungen durchgeführt, um die abweichende und die kontralaterale Seite miteinander zu vergleichen und um Intergruppenunterschiede zu ermitteln. Ebenso evaluiert wurde die Korrelation zwischen Mittellinienasymmetrie und anderen Variablen. Als Signifikanzniveau für die statistischen Berechnungen wurde p = 0,05 festgelegt.
Ergebnisse
Zwischen den Werten auf der abweichenden und der kontralateralen Seite zeigten sich statistisch signifikante Unterschiede für Patienten mit mäßiger und mit ausgeprägter Asymmetrie. Allerdings ließen sich häufiger Unterschiede beobachten bei den ausgeprägten Unterkieferasymmetrien. Bei diesen Patienten bestanden eine signifikante Korrelation zwischen der Gnathion-Abweichung und der unteren dentalen Mittellinienabweichung, ein Unterschied in den Gnathion-Positionen, ein Unterschied in den Höhen der Rami und in den Längen des Corpus mandibulae und ein Unterschied in den transversalen und vertikalen Abweichungen der Punkte Gonion und Jugale.
Schlussfolgerungen
Bei skelettalen Klasse-II-Patienten stehen einige kraniofaziale Besonderheiten—u. a. bilaterale Unterschiede in der Ramushöhe, der Unterkieferlänge sowie der horizontalen und vertikalen Positionierung der Punkte Gonion und Jugale—in Beziehung zu Abweichungen des Kinns. Diese Eigenschaften sind angemessen zu evaluieren.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Based on several examined cases, Angle [3] estimated that Class II malocclusions would have a prevalence of approximately 26% in the population. Since then, epidemiological studies of different populations and ethnic groups have been performed, observing a prevalence of 7–28% [4, 5, 9, 21] in permanent dentition. When only orthodontic patients were evaluated, the prevalence of Class II malocclusions can approach or exceed 50% [6, 31].
The literature shows a number of studies assessing skeletal Class II malocclusions in the sagittal and vertical dimensions [1, 18]. However, little attention has been devoted to changes in the transverse direction, other than those patients with maxillary constriction. This becomes important as it is not unusual for Class II malocclusions to appear only on one side of the arch (i.e., Class II subdivision) [3, 4]. In many of these cases, occlusal disharmony is associated with skeletal asymmetries [19, 23].
It is known, however, that even pleasant faces have a subclinical level of asymmetry [20]. In this context, the term relative symmetry or fluctuant asymmetry may be used as small random variations; it is also widely used as a measure of instability in the development of plants and other animals [22]. However, in moderate or severe asymmetries orthodontists often face the challenge of obtaining final bilateral harmony, either with orthodontic, orthopedic, or surgical approaches [29].
Thus, the identification of morphological components involved in the asymmetric expression is important in mapping out a treatment plan. Currently three-dimensional images allow a comprehensive evaluation of these patients, observing anatomic structures with real size and without anatomical superimpositions [7, 13, 14, 27]. Thus, the aim of this study was to evaluate by cone-beam computed tomography (CBCT) the craniofacial components related with different categories of mandibular asymmetry in adults with skeletal Class II. The null hypothesis is that there are no differences between the deviated and contralateral sides, as well as that there are no differences between different intensities of mandibular asymmetry.
Materials and methods
The study protocol (reference number: 1.591.220) was approved by the Ethics Committee at Universidade do Sul de Santa Catarina (UNISUL, SC, Brazil). All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964, as updated in 2013.
This study was nested in a previous epidemiological investigation of mandibular asymmetries [28]. CBCT images of 120 orthodontic and orthognathic surgery patients were eligible, and the power calculation for the statistic tests applied demonstrated that this sample size would suffice for this study (β < 0.2 using α = 0.05).
All scans were obtained using the same type of device (iCAT®, Imaging Sciences International, Hatfield, PA, USA), adjusted to operate under the following specifications: extended field of view (16 × 22 cm or 17 × 23 cm) 120 KvP, 3-8 mA, and 0.4 mm voxel size. Patients were asked to occlude at maximum intercuspation and relax their lips.
The images of the CBCT were exported in DICOM format (Digital Imaging and Communication in Medicine), using the iCAT Vision® software. The DICOM files were imported into the SimPlant Ortho Pro® 2.0 software (Dental Materialise, Leuven, Belgium). Landmarks were located using the multiplanar reconstruction view, with a measurement scale of 0.01 mm and 0.01°.
The following inclusion criteria were adopted: CBCT images obtained with clinical justification or in case conventional radiographic techniques failed to meet clinical needs, in accordance with the guidelines of the SedentexCT project and the American Academy of Oral and Maxillofacial Radiology [2, 25]; all permanent teeth erupted (with the exception of third molars); subjects ages 19 through 60 years old and with Class II skeletal jaw relationship (ANB > 4.5°, as proposed by Tweed) [30]. The exclusion criteria were the following: a former history of orthodontic treatment, fractures or surgeries in the facial area, degenerative diseases in the temporomandibular joint, craniofacial syndromes and anomalies.
The outcome was categorized into three groups according to the intensity of mandibular asymmetry. Symmetry was defined through the analysis of gnathion deviation, since lateral displacement of the chin shows a higher influence on the perception of facial asymmetry [16, 26]. Regardless of the side of deviation, patients with a gnathion displacement of up to 2 mm in relation to the midsagittal plane were considered to have relative symmetry [15]. Patients with a displacement of more than 2 mm and up to 4 mm were considered to have moderate asymmetry. Lastly, those with a gnathion deviation greater than 4 mm were considered to have severe asymmetry [12, 17]. These cut-off points were previously suggested in the literature [12, 15, 17]. Each category of asymmetry contained 40 individuals, totaling 120 evaluated patients. The landmarks and reference planes used in this study are described in Table 1.
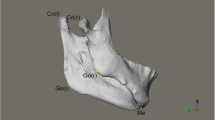
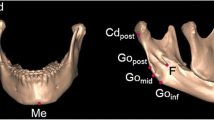
Several measurements were analyzed (mandibular and maxillary components), divided into groups for transverse, sagittal, and vertical evaluation. These measurements were made three-dimensionally and are described in Table 2 and illustrated in Fig. 1.

Illustration of the measurements used in the study: a Gn-MSP, Go-MSP, J-MSP, Cap-MSP, UDM, and LDM; b ANB angle, Go-Coronal, Cap-Coronal, GoGn, CoGo, Go-Camper, and J-Camper. For the bilateral points, the measurements were made both in the contralateral (C) and in the deviated (D) sides
Abb. 1 Darstellung der in der Studie verwendeten Messungen: a Gn-MSP, Go-MSP, J-MSP, Cap-MSP, UDM und LDM; b ANB-Winkel, Go-Coronal, Cap-Coronal, GoGn, CoGo, Go-Camper und J-Camper. Bei bilateralen Punkten wurde sowohl auf der kontralateralen (C) als auch auf der abweichenden (D) Seite gemessen
The methodology used to determine the midsagittal plane in this study was previously validated by the work of Damstra et al. [8]. The deviation of gnathion from the midsagittal plane was calculated in absolute values, regardless of the side of deviation. For other measurements made in midpoints, a positive value was given when the displacement of the point coincided with the side of the gnathion deviation (deviated side); a negative value was given when the displacement occurred on the opposite side (contralateral side). To determine the asymmetry between the measurements made in bilateral cephalometric landmarks, the difference (/dif) of the contralateral side minus the side of mandibular deviation was analyzed.
To estimate the error of the method, 20% of the sample was evaluated at two different times by a single examiner, with an interval of 2 weeks between evaluations. The intraclass coefficient of correlation (ICC) was used, and a value of >0.75 was obtained for all evaluated measurements (with the lowest ICC being 0.77 and the highest 0.99), thus, demonstrating good reliability of the method.
Statistical analyses were conducted using the SPSS® 20.0 software (IBM, Chicago, IL, USA). The Shapiro–Wilk test was applied, demonstrating a normal distribution of the values obtained in bilateral measurements and the abnormal distribution of the values obtained in midpoint measurements. The values obtained on the contralateral side and on the deviated side were compared using the Student’s t test for paired samples. In order to verify possible differences in the measurements between different categories of mandibular asymmetry, the analysis of variance (ANOVA) was conducted (complemented by the Tukey test) when the data were considered normal. The Kruskal–Wallis test, on the other hand, was conducted when the normality criterion was not met (complemented by the Mann–Whitney test with Bonferroni correction). To determine the correlation of the gnathion deviation with other variables evaluated, the Spearman correlation coefficient was applied. A 5% significance level was considered.
Results
The mean of gnathion displacement in relation to the MSP was, in absolute terms, 3.21 mm [standard deviation (SD) 2.75], varying from 0.01–21.49 mm. Other characteristics of the sample and the analyzed groups can be visualized in Table 3.
The null hypothesis was rejected. As to the measurements obtained on the contralateral side and on the deviated side for the bilateral cephalometric measurements, Table 4 presents the means and standard deviations considering the different categories of mandibular asymmetry for these patients. Using the paired samples t test, several differences between the measurements of the contralateral and deviated sides were observed.
A comparison between patients with relative symmetry, moderate asymmetry and severe asymmetry is shown in Table 5. It was possible to verify that the values of Gn-MSP, Go-MSP/dif, UDM, LDM, CoGo/dif, Go-Camper/dif, and J-Camper/dif differed significantly between the groups. For Gn-MSP and Go-MSP/dif, there was a statistically significant difference between all groups. For UDM, LDM, CoGo/dif, Go-Camper/dif, and J-Camper/dif, there was a statistically significant difference between the patients with severe mandibular symmetry and the other ones. Other analyzed variables showed no statistical differences between the groups. It is worthwhile to point out that when the value of the bilateral difference between the measurements (/dif) is negative, this means that the deviated side presented a higher average dimension than that of the contralateral side.
The correlation test (Table 6) demonstrated that there was no variable significantly correlated to the gnathion deviation for patients with moderate asymmetry. For patients with severe asymmetry, the variables Go-MSP/dif, LDM, CoGo/dif, and J-Camper/dif were found to be significantly correlated to gnathion deviation.
Discussion
The results from this study highlight that asymmetrical Class II patients have several disharmonic features that affect the expression of their asymmetries. This could be verified by comparing the values obtained on the contralateral side and on the deviated side of those patients. It is important to mention that it is fundamental to discriminate between different categories of mandibular asymmetry, since these differences can distinguish between a compensatory orthodontic/orthopedic treatment and an orthognatic surgery approach [16, 29].
There are certain limitations in the present study. Functional shifts that could lead to a postural component of the mandibular asymmetries were not analyzed. Since the main goal was to address skeletal mandibular asymmetries, mainly skeletal landmarks were used. However, dental components that could affect craniofacial asymmetries were not assessed. Vertical or transverse deviations of the landmarks A, N, and B can pretend changes in the sagittal dimension of a three-dimensional angle [10], and this may have resulted in errors for establishing the ANB angle, specially in the severe asymmetry group. For establishing the groups, mandibular asymmetry was determined by the lateral displacement of the gnathion point. Nevertheless, it is known that mandibular asymmetries can also be characterized in the vertical plane. In addition, since this study presents a cross-sectional design, it becomes impossible to state the order of occurrence of events in time, and therefore it cannot be defined which abnormal structure was the preliminary cause of the mandibular asymmetry. On the other hand, this study offers advancement with a large sample with controlled data, addressing skeletal alterations in three distinct categories of mandibular asymmetry.
When analyzing Table 4, it can be seen that for individuals with relative mandibular symmetry, the only statistical difference between the contralateral and deviated sides was in the transverse and vertical position of the jugale point in the maxilla. Each was less than 1 mm on average and is clinically nonsignificant. For individuals with asymmetries, bilateral differences could be found in the transverse positioning of the gonion and jugale, as well as the vertical positioning of the gonion and rami height. Moreover, for moderate asymmetry, differences between the contralateral and deviated sides were also found in mandibular body lengths and for severe asymmetry in the vertical position of the jugale points. All these variables should be carefully evaluated, especially for severe asymmetric cases that undergo orthognatic surgery, since this knowledge could determine an atypical osteotomy and/or whether a one- or two-jaw procedure would be indicated [24].
As previously stated by other authors [7, 13, 14, 27], our findings suggest that chin deviations in skeletal Class II individuals seem to be associated with bilateral differences in the position of the gonion and jugale. Bilateral alterations in the gonion position can influence differences in rami heights, mandibular corpus lengths, as well as frontal and lateral mandibular ramal inclination. Alterations in the jugale point positioning can influence maxillary cant and/or laterality.
When the categories of mandibular asymmetry were compared (Table 5), the significant differences, when found, were most often between the severe asymmetry and other groups. This was also stated by Masuoka et al. [16] when they compared patients exhibiting relative symmetry, moderate asymmetry, and severe asymmetry. Hence, the results of the present study indicate that severe mandibular asymmetry has a greater upper and lower dental midline deviation, as well as bilateral difference in the heights of mandibular rami and the vertical position of gonion and jugale points when compared to relative symmetry and moderate asymmetry. For the variables that evaluated lateral gnathion deviation and differences in lateral positioning of the gonion points, all groups were different from each other. For other analyzed variables, there were no differences between the groups.
Ramal inclinations have been shown to be related to severe mandibular asymmetries [7, 13], but most often it is not mentioned if those are related to alterations in the positioning of the condyles or the gonion points. The results presented in Table 5 demonstrated that, for severe mandibular asymmetries, the bilateral difference of the sagittal and lateral position of the condyles occurred to a lesser intensity than the bilateral difference on the sagittal and lateral position of the gonion points (Cap-MSP/dif = −0.51 ± 4.36; Go-MSP/dif = −4.34 ± 4.24; Cap-Coronal/dif = −0.22 ± 2.73; Go-Coronal/dif = 1.27 ± 4.34). Therefore, these findings suggest that frontal and lateral mandibular ramal inclination in severe asymmetries results more from the spatial displacement of the gonion points than that of the condyles.
Chen et al. [7] mentioned that for some patients the lateral deviation of the gonion point from the MSP could be greater than the gnathion displacement to the deviated side. Moreover, few patients exhibited a ramus asymmetry contralateral to the side of chin deviation.
This may also be seen in our findings, where for patients with severe asymmetry the bilateral difference of the positioning of the gonion point in the transverse plane was almost as great as chin deviation, and presented a high standard deviation (Table 5: Gn-MSP = 6.02 ± 2.88; Go-MSP/dif = −4.34 ± 4.24). These aspects need to be carefully evaluated, as the surgical approach, if instituted, should result in the best possible skeletal balance.
Correlation tests (Table 6) were only significant for severe asymmetric patients, and determined that chin deviation was significantly correlated with lower dental midline deviation and difference in the gonion lateral positions, difference in the mandibular rami heights, and difference in the jugale vertical displacements.
The results of this study therefore highlight that for asymmetrical Class II patients not only was the chin deviated, but other craniofacial features were disharmonious as well. The gonion area must be evaluated with caution in all three dimensions. Hajeer et al. [11] analyzed soft-tissue asymmetry in patients before and after orthognatic surgery and stated that in Class II patients surgical changes increased asymmetry. Therefore, for those patients all morphological aspects pointed to in the study are important considerations not only for the surgeon, but also for the orthodontist as the goal should be to create dental asymmetry during decompensation equal in magnitude to the skeletal asymmetry.
Often facial asymmetry is more noticeable in Class III patients, due to the projection of the chin; it is important therefore to not overlook asymmetries in Class II patients whose deformity may be hidden by the “drape” of the soft tissue. This misdiagnosis could lead to extended treatment time and compromised outcomes. Therefore, for severe asymmetric patients, the proper evaluation of characteristics related to mandibular lateral deviation is essential to provide patients with the best treatment possible.
Conclusions
For Class II patients with severe asymmetry, chin deviation was significantly correlated with lower dental midline deviation, differences in the gonion lateral positions, differences in the mandibular rami heights, and differences in the jugale vertical displacements.
References
Al-Khateeb EA, Al-Khateeb SN (2009) Anteroposterior and vertical components of Class II division 1 and division 2 malocclusion. Angle Orthod 79(5):859–866
American Academy of Oral and Maxillofacial Radiology (2013) Clinical recommendations regarding use of cone beam computed tomography in orthodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol 116(2):238–257
Angle EH (1907) Treatment of malocclusion of the teeth, 7th edn. SS White Manufacturing, Philadelphia
Ast DB, Carlos JP, Cons DC (1965) Prevalence and characteristics of malocclusion among senior high school students in up-state New York. Am J Orthod 51(6):437–445
Burgersdijk R, Truin GJ, Frankenmolen F, Kalsbeek H, van’t Hof M, Mulder J (1991) Malocclusion and orthodontic treatment need of 15-74-year-old Dutch adults. Community Dent Oral Epidemiol 19(2):64–67
Celikoglu M, Akpinar S, Yavuz I (2010) The pattern of malocclusion in a sample of orthodontic patients from Turkey. Med Oral Patol Oral Cir Bucal 15(5):e791–e796
Chen YJ, Yao CC, Chang ZC, Lai HH, Lu SC, Kok SH (2016) A new classification of mandibular asymmetry and evaluation of surgical-orthodontic treatment outcomes in Class III malocclusion. J Craniomaxillofac Surg 44(6):676–683
Damstra J, Fourie Z, DeWit M, Ren Y (2012) A three-dimensional comparison of a morphometric and conventional cephalometric midsagittal planes for craniofacial asymmetry. Clinical Oral Investig 16(1):285–294
Emrich RE, Brodie AG, Blayney JR (1965) Prevalence of Class 1, Class 2, and Class 3 malocclusions (Angle) in an urban population. An epidemiological study. J Dent Res 44(5):947–953
Gateno J, Xia JJ, Teichgraeber JF (2011) New 3-dimensional cephalometric analysis for orthognathic surgery. J Oral Maxillofac Surg 69(3):606–622
Hajeer MY, Ayoub AF, Millett DT (2004) Three-dimensional assessment of facial soft-tissue asymmetry before and after orthognathic surgery. Br J Oral Maxillofac Surg 42(5):396–404
Haraguchi S, Takada K, Yasuda Y (2002) Facial asymmetry in subjects with skeletal Class III deformity. Angle Orthod 72(1):28–35
Hwang HS, Hwang CH, Lee KH et al (2006) Maxillofacial 3-dimensional image analysis for the diagnosis of facial asymmetry. Am J Orthod Dentofac Orthop 130(6):779–785
Kim EJ, Palomo JM, Kim SS, Lim HJ, Lee KM, Hwang HS (2011) Maxillofacial characteristics affecting chin deviation between mandibular retrusion and prognathism patients. Angle Orthod 81(6):988–993
Kim SJ, Lee KJ, Lee SH, Baik HS (2013) Morphologic relationship between the cranial base and the mandible in patients with facial asymmetry and mandibular prognathism. Am J Orthod Dentofac Orthop 144(3):330–340
Masuoka N, Momoi Y, Ariji Y, Nawa H, Muramatsu A, Goto S, Ariji E (2005) Can cephalometric indices and subjective evaluation be consistent for facial asymmetry? Angle Orthod 75(4):651–655
Masuoka N, Muramatsu A, Ariji Y, Nawa H, Goto S, Ariji E (2007) Discriminative thresholds of cephalometric indexes in the subjective evaluation of facial asymmetry. Am J Orthod Dentofac Orthop 131(5):609–613
McNamara JA Jr (1981) Components of Class II malocclusion in children 8–10 years of age. Angle Orthod 51(3):177–202
Minich CM, Araújo EA, Behrents RG, Buschang PH, Tanaka OM, Kim KB (2013) Evaluation of skeletal and dental asymmetries in angle Class II subdivision malocclusions with cone-beam computed tomography. Am J Orthod Dentofac Orthop 144(1):57–66
Ovsenik M, Perinetti G, Zhurov A, Richmond S, Primozic J (2014) Three-dimensional assessment of facial asymmetry among pre-pubertal class III subjects: a controlled study. Eur J Orthod 36(4):431–435
Proffit WR, Fields HW Jr, Moray LJ (1998) Prevalence of malocclusion and orthodontic treatment need in the United States: estimates from the NHANES III survey. Int J Adult Orthod Orthognath Surg 13(2):97–106
Quinto-Sánchez M, Adhikari K, Acuña-Alonzo V et al (2015) Facial asymmetry and genetic ancestry in Latin American admixed populations. Am J Phys Anthropol 157(1):58–70
Sanders DA, Rigali PH, Neace WP, Uribe F, Nanda R (2010) Skeletal and dental asymmetries in Class II subdivision malocclusions using cone-beam computed tomography. Am J Orthod Dentofac Orthop 138(5):542.e1-20
Schwartz HC (2011) Efficient surgical management of mandibular asymmetry. J Oral Maxillofac Surg 69(3):645–654
SEDENTEXCT project (2012) Radiation protection no. 172: cone beam CT for dental and maxillofacial radiology. Evidence based guidelines 2012. http://www.sedentexct.eu/content/guidelines-cbct-dental-and-maxillofacial-radiology. Accessed Nov 10 2016.
Severt TR, Proffit WR (1997) The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int J Adult Orthodon Orthognath Surg 12(3):171–176
Sievers MM, Larson BE, Gaillard PR, Wey A (2012) Asymmetry assessment using cone beam CT A Class I and Class II patient comparison. Angle Orthod 82(3):410–417
Thiesen G, Gribel BF, Pereira KCR, Freitas MPM (2016) Is there an association between skeletal asymmetry and tooth absence? Dental Press J Orthod 21(4):73–79
Thiesen G, Gribel BF, Freitas MPM (2015) Facial asymmetry: a current review. Dental Press J Orthod 20(6):110–125
Tweed C (1954) The frankfort-mandibular incisor angle (FMIA) in orthodontic diagnosis, treatment planning and prognosis. Angle Orthod 24(3):121–169
Willems G, De Bruyne I, Verdonck A, Fieuws S, Carels C (2001) Prevalence of dentofacial characteristics in a Belgian orthodontic population. Clin Oral Investig 5(4):220–226
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
G. Thiesen, B. F. Gribel, M. P. M. Freitas, D. R. Oliver, and K. B. Kim declare that they have no conflict of interest.
Human and animal rights statement
This study had no funding. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study. For this retrospective study, the Ethics Committee dismissed formal consent.
Additional information
Professor Guilherme Thiesen.
Rights and permissions
About this article

Cite this article
Thiesen, G., Gribel, B.F., Freitas, M.P.M. et al. Craniofacial features affecting mandibular asymmetries in skeletal Class II patients. J Orofac Orthop 78, 437–445 (2017). https://doi.org/10.1007/s00056-017-0100-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00056-017-0100-6