
Abstract
Objectives
Analyze the association between socioeconomic deprivation and old-age survival in Europe, and investigate whether it varies by country and gender.
Methods
Our study incorporated five countries (Portugal, Spain, France, Italy, and England). A 10-year survival rate expressing the proportion of population aged 75–84 years who reached 85–94 years old was calculated at area-level for 2001–11. To estimate associations, we used Bayesian spatial models and a transnational measure of deprivation. Attributable/prevention fractions were calculated.
Results
Overall, there was a significant association between deprivation and survival in both genders. In England that association was stronger, following a dose–response relation. Although lesser in magnitude, significant associations were observed in Spain and Italy, whereas in France and Portugal these were even weaker. The elimination of socioeconomic differences between areas would increase survival by 7.1%, and even a small reduction in socioeconomic differences would lead to a 1.6% increase.
Conclusions
Socioeconomic deprivation was associated with survival among older adults at ecological-level, although with varying magnitude across countries. Reasons for such cross-country differences should be sought. Our results emphasize the importance of reducing socioeconomic differences between areas.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Health inequalities have been entrenched in European societies for centuries. Between- and within-country differences in mortality and life expectancy have been reported since the 1960s and, despite the overall increase in life expectancy, spatial differentials are still present and seem to be, in part, explained by socioeconomic factors (Mackenbach et al. 2017; Richardson et al. 2013). In the past, the pace of life expectancy improvements was dictated by the decline in premature mortality; currently, further increases in life expectancy depend essentially on reductions in old-age mortality (Huisman et al. 2013). Therefore, survival rates at older ages constitute a good indicator of overall population health and development (Huisman et al. 2004). Although studies among younger groups are relatively common few investigations have, to date, examined the role of socioeconomic factors on the inequalities in life expectancy and mortality among older age groups (Fouweather et al. 2015; Huisman et al. 2004; Kim 2014; Wohland et al. 2014). Nonetheless, there are important reasons to evaluate socioeconomic inequalities in health at advanced ages.
On the one hand, although the impact of socioeconomic deprivation later in life has been found to decrease with age (Green 2013; House et al. 1994), there is also evidence that the disparities in health later in life might not be as small as initially claimed. Huisman et al. found that, in certain countries, socioeconomic inequalities in old-age mortality can be as large as those in middle life (Huisman et al. 2004). Indeed, as the variability in age at death decreases, survivors to older ages have become increasingly heterogeneous in their mortality risks, suggesting that mortality inequalities are shifting in age as survival in early life improves (Engelman et al. 2010). On the other hand, and above all, it is important to note that even if the relative differences between socioeconomic groups decrease with age, absolute differences may not. From a public health perspective, it is crucial to combine relative and absolute measures of inequality (Asada 2010). Notice that subtle differences in mortality risks may represent a large number of potentially preventable deaths; Huisman found that absolute inequalities in mortality rose exponentially with age, reaching a maximum in the ≥ 90 years old age group (Huisman et al. 2004). Moreover, even if the relative inequalities in old-age mortality do not increase in the future, the number of deaths will certainly rise because of the ageing of the population in European countries, which will continue to accelerate in the next decades.
In a previous study, we identified several fold differences in old-age survival across more than four thousand European small areas (Ribeiro et al. 2016). We postulate that a large share of this variation can be attributed to the socioeconomic factors. We also hypothesize there might exist cross-national and gender differences in the association between survival and socioeconomic deprivation. Dozens of studies have compared the socioeconomic gradient in health across different countries and identified noteworthy differences (Dahl and van der Wel 2013; Niedzwiedz et al. 2015). However, these findings are inconsistent and none of these studies looked at old-age survival (Brennenstuhl et al. 2012). There is also evidence that the socioeconomic gradient in health might be stronger among men than in women (Borrell et al. 2014; Gotsens et al. 2013; Hoffmann et al. 2014; Mari-Dell’Olmo et al. 2015), yet not all studies support this conclusion (Koskinen and Martelin 1994; Mustard and Etches 2003).
In this sequence, the present ecological study aimed to determine whether spatial inequalities in old-age survival across European areas are associated with socioeconomic deprivation. Specifically, we addressed the following research questions: (1) is there an ecological association between area-level old-age survival and socioeconomic deprivation and what is the magnitude of the association, (2) does it vary by country and gender, and (3) how much could area-level old-age survival be improved by eliminating and/or reducing socioeconomic differences?
Methods
Study area
Our study included five European countries and 1911 areas: Portugal (308 ‘municípios’), Spain (337 ‘comarcas’), France (329 ‘arrondissements’), England (318 ‘local authorities’) and Italy (619 ‘distrettos sanitarios’). The average population per area in 2011 was 32,246 in Portugal, 69,464 in Spain, 177,853 in France, 83,353 in England, and 46,529 in Italy. Despite not covering all of Europe, the five included countries account for 35% of the European Union population and represent two distinct geographical regions—Southern and Western Europe—and different welfare regimes (Bambra 2011)—England, generally labelled as Liberal; Spain, Portugal and Italy, positioned in the Southern Europe regime; and France classified as Conservative/Corporatist/Bismarckian.
Outcome: old-age survival
Mortality data in the oldest-old was not disclosed for local areas and, even if available, the calculus of life expectancy in late life for local areas comes with well documented problems (Eayres and Williams 2004). Consequently, we derived a measure of old-age survival (\(r_{i} = \frac{{y_{i} }}{{n_{i} }}\)) that expresses the probability of the people aged 75–84 years surviving for an additional 10 years, i.e., surpassing the average life expectancy, where \(r_{i}\) is a 10-year survival rate, \(i\) = 1,…,1911, denotes area, \(y_{i}\) represents the population aged 85–94 years old in 2011 and \(n_{i}\) the population aged 75–84 years, 10 years before, in 2001 (Ribeiro et al. 2016). To calculate this rate we obtained population counts (institutionalized residents were not removed from these counts) from the Statistic Offices of each country, by 5-year age groups (75–79, 80–84, 85–89, and 90–94), gender, census year (2001 and 2011), and by the smallest geographical area available (previously defined).
Covariate: socioeconomic deprivation
The European Deprivation Index (EDI) was used to classify areas according to each one’s level of socioeconomic deprivation (Fig. 1). The EDI is a transnational multivariate index developed for France, England, Italy, Spain, and Portugal (Guillaume et al. 2015). The EDI was used in the present study, because, although there are national deprivation indexes, no other transnationally comparable index of socioeconomic deprivation exists in Europe. The construction of EDI is extensively described elsewhere (Guillaume et al. 2015; Ribeiro et al. 2017). Briefly, in every country, the index included socioeconomic variables related with housing conditions, social class, educational attainment, and demographics. The composing variables differed by country, but the index was comparable between countries because the choice of the variables followed the same methodological procedures and theoretical framework. Included variables and weighting are fully depicted in supplementary material (supplementary material 1). The index was categorized into ten rank-ordered classes (C1—least to C10—most deprived). For categorization, we have used theoretical deciles instead of the ‘traditional’ empirical deciles. Cut-offs for these theoretical deciles were defined based on standard deviations from the overall mean and customized so that the classes included a more even number of geographical units. This approach avoids the well-known problems of using empirical quintiles, which assume homogeneity of risk within groups (Bennette and Vickers 2012).

Spatial distribution of the European deprivation index (a) and spatial distribution of the old-age survival rates posterior means for men (b) and women (c) (England, France, Italy, Portugal and Spain, 2001–2011)
Statistical model
To take into account the spatial autocorrelation and large variance of local areas, we used Hierarchical Bayesian spatial models. Additionally, to account for the fact that the effect of each deprivation class depends on the effect of the previous (ordered categorical covariate), and to allow for flexible slopes in the risk curve, flexible regression models were employed (Rue et al. 2005).
We assumed that the response variable \((Y_{ijk} )\), number of survivors in each country \(k\), area \(i\) and gender \(j\), follows a binomial distribution, where \(p_{ijk}\) is an unknown survival rate and \(n_{ijk}\) is the population aged 75–84 years, 10 years before Eq. (1).
The logit of the survival rate was modelled considering gender, country, and the interaction between the covariate (socioeconomic deprivation) and country, gender and area Eq. (2.1).
where \(\eta_{ijk}\) is the linear predictor, \({\text{gender}}_{j}\) is an intercept in the model that is specific for each gender, \({\text{country}}_{k }\) is an intercept in the model that is specific for each country, and the interaction term, \(f_{jk} (x_{i} )\), is the gender- and country-specific effect of socioeconomic deprivation, which assumes the value \(x_{i}\) for the area \(i\), and \(s_{i}\) is the area-specific effect.
The function \(f_{jk}\) assumes a nonlinear effect of the covariate. This nonlinear effect is modelled as a first order random walk prior over the covariate’ classes, that is, a normal distribution, whose mean at each class is an average over the neighbouring classes (Martino and Rue 2009). As \(x_{i}\) was categorized into classes, we can simplify \(f_{jk} (x_{i} )\) into \(e_{ljk}\), which denotes the effect of covariate class, \(l\), for gender \(j\) and country \(k\).
The area-specific effect \(s_{i}\) was modelled considering a Besag, York and Mollié model Eq. (2.2).
where \(u_{i}\) is the structured effect and \(v_{i}\) is the unstructured effect. The \(u_{i}\) effect was scaled to make the model more intuitive and interpretable, so that \(\varphi\) expresses the proportion of the spatial effect due to the structured part and 1/\(\tau\) is the marginal variance of \(s_{i}\). A penalised complexity prior was considered.
From \(e_{ljk}\) the “relative risk” (RR) of survival for each socioeconomic deprivation class \(l\), gender \(j\) and country \(k\) and was calculated. An RR was considered significantly higher or lower if its 95% credible interval (95% CrI) did not include the value 1. RR and 95% CrI were derived from their posterior means and quantiles. Posterior distributions were obtained using the Integrated Nested Laplace Approximation (INLA), which was implemented in the R INLA library (Rue et al. 2009). The R code is provided in Online resource 1. The model from Eq. (2.1) was our final model, but we started with a model with no country interaction effects to obtain the overall associations between deprivation and survival.
Complementarily, the Slope Index of Inequality (SII) and the Relative Index of Inequality (RRI) and corresponding 95% CrI were computed, using previously described methods (Dalstra et al. 2002; Mackenbach and Kunst 1997). The SII expresses the health Inequality between the top and bottom of the social hierarchy in terms of rate differences, whereas the RRI represents those differences in terms of rate ratios. The larger the RII/SII the larger the inequality.
Population attributable risk proportion and preventable proportion
We calculated the population attributable risk proportion (PAR) by adapting the formulas proposed by Rockhill et al. (Rockhill et al. 1998). Our formula Eq. (3) allows for estimation of what the decrease in old-age deaths would be in the absence of socioeconomic deprivation, i.e., if the ‘risk’ of survival in all the areas was equal to the risk of survival in the least deprived areas.
where \(RR_{i}\) refers to the RR associated to each of the i deprivation class C i and \(P_{i }\) the corresponding proportion of the total population aged 75–84 years in 2001.
Because the elimination of socioeconomic inequalities might not be (easily) achieved, a more realistic measure was also used. The preventable proportion (PP) estimates what would be the decrease in old-age mortality if the areas moved a class upwards in the socioeconomic spectrum (C2 to C1, C3 to C2…) Eq. (4).
Both proportions (PAR and PP) were used to compute the absolute number of “additional” survivors after improvement in socioeconomic deprivation by multiplying them by the number of people aged 75–84 years who reached 85–94 years in each country.
Results
On average, the proportion of the population aged 75–84 years that reached 85–94 years was 35.3% (range 22.9–53.7) among men and 48.5% (31.0–67.8) among women. There were important spatial inequalities, depicted in the maps from Fig. 1. The lowest survival rates were observed in Portugal (31.8 and 43.3% for men and women, respectively), followed by England (33.9; 44.8), Italy (35.8; 49.6), Spain (36.6; 49.8), and France (37.4; 53.7).
Tables 1 and 2 depict the average survival rates of each country and gender according to socioeconomic deprivation. Generally, old-age survival decreased as deprivation level increased. From the least to the most deprived areas, survival rates experienced a decline of 12% in men and 14% in women. However, the deprivation-related gaps in survival rates seemed to be larger in certain countries.
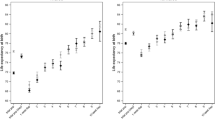
Figure 2 shows the association between area deprivation and survival rates for each country and gender. The RR compares old-age survival in a certain deprivation class with the overall survival in any given country and gender. The inclusion of socioeconomic deprivation as a covariate reduced the variance of the spatial term by 30.8%, meaning that deprivation explains a substantial part of spatial inequalities in old-age survival. Overall, there was a significant, and approximately linear, association between socioeconomic deprivation and survival in both genders [Men in least deprived areas compared with the overall men survival RR = 1.047 (1.033–1.062); Women 1.074 (1.064–1.086)]. Important interactions were observed. England was the country where the effect of socioeconomic deprivation was the strongest—the least deprived areas had about 30% higher survival rates than the most deprived. There, the association followed a clear dose response relationship, with ‘chance’ of survival increasing as deprivation decreases [Men RR = 1.144 (1.109–1.179); Women 1.135 (1.108–1.162)]. Indeed, the RII and SII from England depicted in Tables 1, 2 were the largest from all the studied countries [Men RII = 1.44 (1.37–1.51); Women 1.43 (1.38–1.48); Men SII = 12.00 (10.65–13.35); Women 15.46 (14.25–26.67)]

Association (Relative Risks and 95% Credible Intervals) between old-age survival and socioeconomic deprivation according to gender and country (England, France, Italy, Portugal and Spain, 2001–2011)
Significant associations between deprivation and survival, albeit of lower magnitude, were observed in Spain and Italy, where the most advantaged areas registered consistently higher survival rates as compared to the most disadvantaged [RR: Italian men, 1.028 (1.002–1.055); Italian women, 1.066 (1.046–1.086); Spanish men, 1.058 (1.029–1.088); Spanish women, 1.081 (1.059–1.104)], with corresponding RII of 1.10 (1.05–1.16) and 1.17 (1.11–1.23) for Italy and 1.15 (1.06–1.24) and 1.19 (1.14–1.25) for Spain.
Although most RRs were on the borderline of statistical significance and the magnitude of the inequalities was much smaller, survival rates of women in Portugal and France were significantly higher in the most advantaged end [Portugal = 1.055 (1.031–1.080); France = 1.048 (1.023–1.073)]. Thus, the values of RII were lower than in the other countries [France = 1.14 (1.05–1.23); Portugal = 1.14 (1.08–1.19)]. Among men, survival in France and in Portugal was still significantly (but weakly) associated with deprivation, as expressed by the corresponding RII [France = 1.09 (1.00–1.18) and Portugal = 1.05 (1.00–1.10)].
By eliminating socioeconomic differences between areas (wherein all areas have the same survival levels of the least deprived areas) the number of survivors in men would increase by 5.5 and by 7.9% in women, more than 370,000 fewer deaths in 10 years (Tables 1, 2). Larger gains would be expected in England (+ 15.1% in men; + 14.3% in women), followed by Spain (+ 6.3; + 8.6) and Italy (+ 2.4; + 5.6). In Portugal and France improvements would be almost irrelevant in men, but still notable among women (4.5 and 5.4%, respectively). And even if each area improved by only one class upward in the socioeconomic spectrum, survival could increase by 1.1 and 1.8% in men and women, respectively, i.e., 80,000 fewer deaths in 10 years. Averaging the estimates for men and women, the entire elimination of socioeconomic differences between areas would increase survival by 7.1%, and even a small reduction in socioeconomic differences would lead to a 1.6% increase.
Discussion
Our study reports that socioeconomic deprivation significantly influences survival after 75 years of age in five European countries. England was by far the country where the association between deprivation and old-age survival was stronger, with a clear linear effect of decreasing survival as deprivation levels increase. Although lesser in magnitude, significant associations were observed in Spain and Italy, whereas in France and Portugal these associations were weaker. We projected that the elimination of socioeconomic differences between areas would increase survival by 7.1% and, even a slight reduction in socioeconomic differences would mean a 1.6% higher survival in these countries.
Much has already been published about the effect of area-level of socioeconomic deprivation on life expectancy at birth and on overall mortality (Borrell et al. 2014; Gotsens et al. 2013; Hoffmann et al. 2014; Mackenbach et al. 2008; Mari-Dell’Olmo et al. 2015; Richardson et al. 2013; Taulbut et al. 2014). In our study, we found that this effect exists later in life too. The probability of people aged 75–84 years reaching more advanced ages was significantly higher in the least deprived areas (15–20% higher) compared to the most deprived. Literature in this topic is sparse, and most studies correspond to between-country comparisons. However, they consistently show that socioeconomic deprivation matters. A Europe-wide study reported mortality rate ratios (most vs. the least educated) that ranged from 1.05 in Norway (men) to 1.39 in Austria (women) (Huisman et al. 2004); whilst our study area and design is considerably different, these ratios match ours. Kim (Kim 2014) constructed a similar indicator (probability of reaching 100 years) and found it was highly correlated with socioeconomic factors, such standard of living, as well as health care expenditure and. Looking at other endpoint (healthy life expectancy—HLE—at old ages), three studies found that material deprivation, as well as health care expenditure, explained cross-national HLE inequalities across Europe (Fouweather et al. 2015; Wohland et al. 2014). The influence of socioeconomic deprivation later in life has also been confirmed by individual level studies, recently summarized in a literature review (Huisman et al. 2013). In terms of measures of impact, and compared to other public health and socioeconomic policy interventions’ effects on mortality on this age group (Stringhini et al. 2017), the effects of reducing deprivation gradients demonstrated here are rather large; we showed that the elimination of socioeconomic differences between areas would increase survival by 7.1% and, even a slight reduction in socioeconomic differences, would mean a 1.6% higher survival in these countries.
Corroborating other investigations, we found relevant cross-national differences in the effect of socioeconomic deprivation on mortality. In a study involving 22 European counties, socioeconomic inequalities in mortality were found to be smaller in some southern European countries and larger in the Eastern and Baltic states (Mackenbach et al. 2008). Similarly, researchers of INEQ-CITIES project observed that the effect magnitude of socioeconomic deprivation in all-cause (Borrell et al. 2014), cause-specific (Hoffmann et al. 2014; Mari-Dell’Olmo et al. 2015), and injury related mortality (Gotsens et al. 2013) was smaller in the southern European cities than in northern, western and central-eastern European cities. We did not find such a clear divide between South and Western Europe. Certainly, in England (Western Europe) the effect of socioeconomic deprivation in survival was the strongest, but consistent and significant associations between deprivation and survival were also observed in Italy and Spain, particularly among women.
The welfare regime theory is being increasingly used to understand health inequalities across different nations. The welfare regime refers to the state’s function in providing services, such as education and social protection. Its role in influencing population health is still under intense debate (Brennenstuhl et al. 2012), but the most generous welfare regimes—Scandinavian (e.g., Sweden), Conservative (e.g., France) and, at lesser extent, Southern European (e.g., Portugal, Italy, Spain)—are supposed to ‘protect’ citizens against the detrimental effects of deprivation better than liberal regimes (e.g., United Kingdom). The welfare regime theory might then explain the substantial effect of socioeconomic factors in England and their relative mildness in France and Portugal. Following up the idea that the state generosity may contribute to reduce the effects of socioeconomic deprivation, it is important to note that the net pension replacement rates in the studied countries are rather different and might also help us to understand the differential influence of socioeconomic deprivation on old-age survival (Lundberg et al. 2008). Net pension replacement rates measure how effectively a pension system provides a retirement income to replace earnings, the main source of income before retirement. This indicator is measured in percentage of pre-retirement earnings (OECD 2017). Data from the OECD (Organisation for Economic Co-operation and Development), shown in Table 3, places England amongst the countries with the lowest replacement rates of the European continent (28.5%), contrasting with France (67.7%), Italy (79.7%), Portugal and Spain (89.5%).
The type of healthcare system might also contribute to such differentials: a strong healthcare system that guarantees universal and free access and emphasizes primary care might ameliorate the effects of socioeconomic deprivation. The countries we evaluated have universal (England, Portugal, Italy) or nearly universal healthcare systems (France, Spain) (Jakubowski et al. 1998); and have high (Portugal, England, Spain) or medium (Italy, France) strength primary care systems defined based on their structure, accessibility, continuity, comprehensiveness and coordination (Kringos et al. 2013). However, paradoxically, we observed that the effect of socioeconomic deprivation was particularly prominent in England, known for its primary care centered health system and for being one of the world’s largest publicly funded health systems (Susser 1993).
Finally, the social distribution of risk factors, particularly smoking, might also help to interpret cross-national differences. Large education-related inequalities in smoking were seen in the Western European countries and small inequalities (and, among women, even reverse inequalities, in which smoking rates are higher amongst the most educated) were observed in Southern European countries (Mackenbach et al. 2008), which are in an earlier stage of the smoking epidemic. That might explain the lesser impact of socioeconomic deprivation in Portugal and the stronger effect in England. But, again, it does not clarify the position of Spain and Italy, wherein smoking patterns are less socioeconomically patterned and smoking prevalence is higher in more educated women.
We did not observe the effect of socioeconomic deprivation on survival being stronger among men, contrasting with articles that report men are more susceptible to socioeconomic circumstances (Borrell et al. 2014; Gotsens et al. 2013; Hoffmann et al. 2014; Mari-Dell’Olmo et al. 2015). Yet other studies showed that these gender differences either do not exist or are more evident among women (Koskinen and Martelin 1994; Mustard and Etches 2003). Indeed, we observed that the effects of deprivation on old-age survival were slightly larger among women and, in Portugal and France, almost absent in men. It is actually plausible that inequalities among women become wider later in life. Women live longer than men; in our study mean old-age survival rates were 48.5% in women and 35.3% in men. Therefore, due to delayed mortality selection, the pool of women that reaches advanced ages can be expected to be more diverse in terms of socioeconomic characteristics, leading to a wider gap in survival between the least and most deprived.
Some limitations of the study must be discussed. Although we tried to use areas as comparable as possible, in some countries the areas were, in average, larger than in others. It is usually recommended to use the smallest units possible—the use of large geographical areas can “wash away” (gerrymander) differences in covariates and outcomes. Consequently, despite Hierarchical Bayesian models accounting for the different population size of the areas, we might have underestimated the true dimension of the effect of deprivation on survival and ultimately failed to detect significant associations. For instance, in France, where larger geographical units were employed, the gap between the most and least deprived areas was smaller. Nonetheless, in the UK, the mean population per area was also relatively large and substantial differences between the most and least deprived areas were observed. Our study was also grounded on the assumption that people have lived in the same area for 10 years. Migration of population aged 75 years or more, although infrequent, remains a possibility and can constitute a substantial source of error. Yet, we have a number of reasons to believe that our results were not driven by migration patterns. Firstly, according to Tatsiramos and colleagues, migration of those aged ≥ 75 years is infrequent, ranging (for the period 1994–2001) from roughly 1–1.5% in Southern European countries to approximately 2–3% in Western European countries such as France and the UK (Tatsiramos 2006). Moreover, among the oldest-old, local mobility (within short distances) to seek assistance in nursing homes and near relatives is the most common form of migration (Meyer and Speare 1985; Port et al. 2001). These figures, combined with the fact that we have used relatively large geographical units, suggest that the error introduced by migration later in life is expected to be small. Furthermore, evidence suggests that residential mobility is most likely to cause an underestimation of spatial inequalities and socioeconomic effects (Bryere et al. 2015).
Our study has numerous strengths as well. We were able to collect homogeneous and internationally comparable data at local area-level for five countries and derived a measure of old-age survival that can be used as an alternative to life expectancy in older ages. This is especially relevant since building internationally comparable datasets to monitor health inequalities is a top priority. Moreover, we have employed a transnational multivariate index of socioeconomic deprivation to quantify the association with old-age survival. This has not been done before at least to such a Europe-wide extent (the INEQ-Cities project followed similar approach but only covered metropolitan areas Borrell et al. 2014; Gotsens et al. 2013; Hoffmann et al. 2014; Mari-Dell’Olmo et al. 2015). Cross-national studies on the impact of socioeconomic factors have been using single indicators of socioeconomic deprivation (education, income, or occupation), which do not fully capture the multifactorial nature and the context specificity of deprivation.
Concluding, socioeconomic deprivation seems to shape the survival probability of the moderately-to-oldest-old from five European countries. These results highlight the need to implement actions to reduce of the socioeconomic gap between European areas and regions, as this reduction may improve and render more uniform the chances of survival among the oldest-old. Furthermore, because we observed significant cross-national differences in the effect of deprivation, it is crucial to better understand why socioeconomic gradients in survival vary so much across these European countries—is welfare provision acting as a buffer against the detrimental effects of deprivation, or are there other forces (informal support networks, culture) performing in parallel?
References
Asada Y (2010) On the choice of absolute or relative inequality measures. Milbank Q 88:616–622. https://doi.org/10.1111/j.1468-0009.2010.00614.x
Bambra C (2011) Health inequalities and welfare state regimes: theoretical insights on a public health ‘puzzle’. J Epidemiol Community Health 65:740–745. https://doi.org/10.1136/jech.2011.136333
Borrell C, Mari-Dell’olmo M, Palencia L, Gotsens M, Burstrom BO, Dominguez-Berjon F, Rodriguez-Sanz M, Dzurova D, Gandarillas A, Hoffmann R, Kovacs K, Marinacci C, Martikainen P, Pikhart H, Corman D, Rosicova K, Saez M, Santana P, Tarkiainen L, Puigpinos R, Morrison J, Pasarin MI, Diez E (2014) Socioeconomic inequalities in mortality in 16 European cities. Scand J Public Health 42:245–254. https://doi.org/10.1177/1403494814522556
Brennenstuhl S, Quesnel-Vallee A, McDonough P (2012) Welfare regimes, population health and health inequalities: a research synthesis. J Epidemiol Community Health 66:397–409. https://doi.org/10.1136/jech-2011-200277
Bryere J, Pornet C, Dejardin O, Launay L, Guittet L, Launoy G (2015) Correction of misclassification bias induced by the residential mobility in studies examining the link between socioeconomic environment and cancer incidence. Cancer Epidemiol 39:256–264. https://doi.org/10.1016/j.canep.2014.12.008
Dahl E, van der Wel KA (2013) Educational inequalities in health in European welfare states: a social expenditure approach. Soc Sci Med 81:60–69. https://doi.org/10.1016/j.socscimed.2012.12.010
Dalstra J, Kunst A, Geurts J, Frenken F, Mackenbach J (2002) Trends in socioeconomic health inequalities in the Netherlands, 1981–1999. J Epidemiol Community Health 56:927–934. https://doi.org/10.1136/jech.56.12.927
Eayres D, Williams E (2004) Evaluation of methodologies for small area life expectancy estimation. J Epidemiol Community Health 58:243–249. https://doi.org/10.1136/jech.2003.009654
Engelman M, Canudas-Romo V, Agree EM (2010) The implications of increased survivorship for mortality variation in aging populations. Popul Dev Rev 36:511–539. https://doi.org/10.1111/j.1728-4457.2010.00344.x
Fouweather T, Gillies C, Wohland P, Van Oyen H, Nusselder W, Robine J-M, Cambois E, Jagger C (2015) Comparison of socio-economic indicators explaining inequalities in healthy life years at age 50 in Europe: 2005 and 2010. Eur J Public Health. https://doi.org/10.1093/eurpub/ckv070
Gotsens M et al (2013) Socioeconomic inequalities in injury mortality in small areas of 15 European cities. Health Place 24:165–172. https://doi.org/10.1016/j.healthplace.2013.09.003
Green MA (2013) The equalisation hypothesis and changes in geographical inequalities of age based mortality in England, 2002–2004 to 2008–2010. Soc Sci Med 87:93–98. https://doi.org/10.1016/j.socscimed.2013.03.029
Guillaume E, Pornet C, Dejardin O, Launay L, Lillini R, Vercelli M, Marí-Dell’Olmo M, Fernández Fontelo A, Borrell C, Ribeiro AI, Pina MFd, Mayer A, Delpierre C, Rachet B, Launoy G (2015) Development of a cross-cultural deprivation index in five European countries. J Epidemiol Community Health. https://doi.org/10.1136/jech-2015-205729
Hoffmann R et al (2014) Social differences in avoidable mortality between small areas of 15 European cities: an ecological study. Int J Health Geogr 13:8. https://doi.org/10.1186/1476-072x-13-8
House JS, Lepkowski JM, Kinney AM, Mero RP, Kessler RC, Herzog AR (1994) The social stratification of aging and health. J Health Soc Behav 35:213–234. https://doi.org/10.2307/2137277
Huisman M, Kunst AE, Andersen O, Bopp M, Borgan JK, Borrell C, Costa G, Deboosere P, Desplanques G, Donkin A, Gadeyne S, Minder C, Regidor E, Spadea T, Valkonen T, Mackenbach JP (2004) Socioeconomic inequalities in mortality among elderly people in 11 European populations. J Epidemiol Community Health 58:468–475
Huisman M, Read S, Towriss CA, Deeg DJ, Grundy E (2013) Socioeconomic inequalities in mortality rates in old age in the world health organization Europe region. Epidemiol Rev 35:84–97. https://doi.org/10.1093/epirev/mxs010
Jakubowski E, Busse R, Chambers GR (1998) Health Care Systems in The EU a Comparative Study. European Parliament
Kim J (2014) Association between social factors of health ageing and longevity: determinants of the Longevity Index (LI) in OECD Countries. Ageing Int 39:97–105. https://doi.org/10.1007/s12126-012-9178-8
Koskinen S, Martelin T (1994) Why are socioeconomic mortality differences smaller among women than among men? Soc Sci Med 38:1385–1396
Kringos DS, Boerma WGW, van der Zee J, Groenewegen PP (2013) Political, cultural and economic foundations of primary care in Europe. Soc Sci Med 99:9–17. https://doi.org/10.1016/j.socscimed.2013.09.017
Lundberg O, Yngwe MÅ, Stjärne MK, Elstad JI, Ferrarini T, Kangas O, Norström T, Palme J, Fritzell J (2008) The role of welfare state principles and generosity in social policy programmes for public health: an international comparative study. Lancet 372:1633–1640. https://doi.org/10.1016/S0140-6736(08)61686-4
Mackenbach JP, Kunst AE (1997) Measuring the magnitude of socio-economic inequalities in health: an overview of available measures illustrated with two examples from Europe. Soc Sci Med 44:757–771. https://doi.org/10.1016/S0277-9536(96)00073-1
Mackenbach JP, Stirbu I, Roskam AJ, Schaap MM, Menvielle G, Leinsalu M, Kunst AE (2008) Socioeconomic inequalities in health in 22 European countries. N Engl J Med 358:2468–2481. https://doi.org/10.1056/NEJMsa0707519
Mackenbach JP, Hu Y, Artnik B, Bopp M, Costa G, Kalediene R, Martikainen P, Menvielle G, Strand BH, Wojtyniak B, Nusselder WJ (2017) Trends in inequalities in mortality amenable to health care In 17 European Countries Health affairs (Project Hope) 36:1110-1118 https://doi.org/10.1377/hlthaff.2016.1674
Mari-Dell’Olmo M, Gotsens M, Palencia L, Burstrom B, Corman D, Costa G, Deboosere P, Diez E, Dominguez-Berjon F, Dzurova D, Gandarillas A, Hoffmann R, Kovacs K, Martikainen P, Demaria M, Pikhart H, Rodriguez-Sanz M, Saez M, Santana P, Schwierz C, Tarkiainen L, Borrell C (2015) Socioeconomic inequalities in cause-specific mortality in 15 European cities. J Epidemiol Community Health 69:432–441. https://doi.org/10.1136/jech-2014-204312
Martino S, Rue H (2009) Implementing approximate bayesian inference using integrated nested laplace approximation: a manual for the inla program https://www.mathntnuno/~hrue/GMRFsim/manualpdf
Meyer JW, Speare A (1985) Distinctively elderly mobility: types and determinants. Econ Geogr 61:79–88
Mustard C, Etches J (2003) Gender differences in socioeconomic Inequality in mortality. J Epidemiol Community Health 57:974–980. https://doi.org/10.1136/jech.57.12.974
Niedzwiedz CL, Pell JP, Mitchell R (2015) The relationship between financial distress and life-course socioeconomic inequalities in well-being: cross-national analysis of European Welfare States. Am J Public Health 105:2090–2098. https://doi.org/10.2105/ajph.2015.302722
OECD (2017) Net pension replacement rates (indicator). https://doi.org/10.1787/4b03f028-en (Accessed on 26 November 2017)
Port CL, Gruber-Baldini AL, Burton L, Baumgarten M, Hebel JR, Zimmerman SI, Magaziner J (2001) Resident contact with family and friends following nursing home admission. Gerontologist 41:589–596
Ribeiro AI, Krainski ET, Carvalho MS, Pina MDFD (2016) Where do people live longer and shorter lives? An ecological study of old-age survival across 4404 small areas from 18 European countries. J Epidemiol Community Health. https://doi.org/10.1136/jech-2015-206827
Ribeiro AI, Mayer A, Miranda A, Pina MF (2017) The portuguese version of the European Deprivation Index: an instrument to study health inequalities. Acta Médica Portuguesa 30:17–25
Richardson EA, Pearce J, Mitchell R, Shortt NK, Tunstall H (2013) Have regional inequalities in life expectancy widened within the European Union between 1991 and 2008? Eur J Public Health 24:357–363
Rockhill B, Newman B, Weinberg C (1998) Use and misuse of population attributable fractions. Am J Public Health 88:15–19
Rue H, Held L, Raton B (2005) Gaussian Markov random fields: theory and applications. Chapman & Hall/CRC, Boca Raton
Rue H, Martino S, Lindgren F, Simpson D, Riebler A (2009) INLA: Functions which allow to perform full Bayesian analysis of latent Gaussian models using Integrated Nested Laplace Approximaxion. R Package Version
Stringhini S et al (2017) Socioeconomic status and the 25 × 25 risk factors as determinants of premature mortality: a multicohort study and meta-analysis of 1 7 million men and women. Lancet 389:1229–1237. https://doi.org/10.1016/S0140-6736(16)32380-7
Susser M (1993) Health as a human right: an epidemiologist’s perspective on the public health. Am J Public Health 83:418–426
Tatsiramos K (2006) Residential Mobility and Housing Adjustment of Older Households in Europe IZA Discussion Papers p 1–27
Taulbut M, Walsh D, McCartney G, Parcell S, Hartmann A, Poirier G, Strniskova D, Hanlon P (2014) Spatial inequalities in life expectancy within postindustrial regions of Europe: a cross-sectional observational study. BMJ Open. https://doi.org/10.1136/bmjopen-2013-004711
Wohland P, Rees P, Gillies C, Alvanides S, Matthews FE, O’Neill V, Jagger C (2014) Drivers of Inequality in disability-free expectancy at birth and age 85 across space and time in Great Britain. J Epidemiol Community Health 68:826–833. https://doi.org/10.1136/jech-2014-204083
Acknowledgements
This work was supported by Portuguese funds through FCT—Fundação para a Ciência e a Tecnologia in the framework of project UID/BIM/04293/2013. AIR and MFP would also like to thank to FC—Fundação para a Ciência e a Tecnologia for the Grants PTDC/SAU-EPI/113424/2009 and SFRH/BD/82529/2011. MSC was supported by CNpQ (309692/2013-0) and FAPERJ (E-26/203.557/2014).We are very grateful to the National Statistic Offices for sending us the required data and to all the members of the European Deprivation Index (EDI) team. The authors would like to thank Rogério Ribeiro for the help in preparing visual supports, Alexandra Guttentag for her work as language editor, and the anonymous reviewers for their highly valuable corrections and suggestions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Ribeiro, A.I., Krainski, E.T., Carvalho, M.S. et al. Does community deprivation determine longevity after the age of 75? A cross-national analysis. Int J Public Health 63, 469–479 (2018). https://doi.org/10.1007/s00038-018-1081-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00038-018-1081-y