
Abstract
Purpose
To determine the causes of failure of epidural analgesia during labour and delivery.
Methods
During six months, pregnant patients receiving epidural analgesia and delivering vaginally were studied prospectively. Bupivacaine 0.125% was used for the initial bolus dose and subsequent continuous infusion. Top-ups of the same solution were used for inadequate pain relief assessed using a visual analogue pain score (VAPS) and/or by clinical examination. Inadequate pain relief was defined as the need for ≥ 2 top-ups in addition to epidural infusion and failure during delivery as VAPS ≥ 30 mm during the expulsion phase.
Results
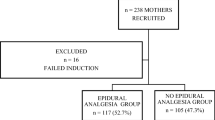
1009 patients delivered during this period, 596 had epidural analgesia for vaginal delivery of a live infant and data were complete in 456. Inadequate pain relief during labour and during delivery were found in 5.3% and 19.7% of patients. Risk factors of inadequate pain relief included: inadequate analgesic efficacy of the first dose (Odds ratio: 3.5, P = 0.001) and posterior presentation (Odds ratio: 5.6, P = 0.001). Radicular pain during epidural placement was associated with failure during labour (Odds ratio: 3.9, P = 0.05). Duration of epidural analgesia > six hours (Odds ratio: 9.1, P = 0.001) was a risk factor for insufficient pain relief during labour whereas duration of epidural analgesia < one hour was associated with pain during delivery (Odds ratio: 18.3, P = 0.001).
Conclusion
Several obstetrical and epidural-related factors increase the risk of inadequate epidural analgesia. For some, simple changes of practice pattern may lead to improved pain relief.
Résumé
Objectif
Déterminer les causes d’insuffisance de l’analgésie péridurale obstétricale.
Méthodes
Pendant 6 mois, toutes les patientes en travail ayant reçu une analgésie péridurale ont été évaluées prospectivement. La bupivacaïne 0,125 % a été utilisée pour l’injection péridurale initiale et pour la perfusion continue de même que pour les réinjections qui ont suivi l’évaluation de la douleur par l’échelle visuelle analogique (EVA) et la vérification du bloc. Une insuffisance d’analgésie pendant le travail a été définie par le besoin d’au moins deux réinjections (en plus de la perfusion péridurale continue) et lors de l’accouchement par une EVA 30 mm.
Résultats
Parmi les 1009 patientes étudiées, 596 ont reçu une analgésie péridurale pour donner naissance à un enfant vivant par voie vaginale et les données étaient complètes pour 456 d’entre elles (76,5 %). Une insuffisance d’analgésie a été constatée pendant le travail chez 5,3 % des patientes et, lors de l’accouchement, chez 19,7 %. Plusieurs facteurs de risque d’insuffisance d’analgésie ont été communs aux phases de dilatation et d’expulsion: insuffisance analgésique du premier bolus (coefficient de risque CR: 3,5; P = 0,001) et présentation postérieure (CR: 5,6; P = 0,001). La survenue d’une radiculalgie pendant la ponction était associée à un risque d’analgésie insuffisante pendant le travail (CR: 3,9; P = 0,05). Une durée d’analgésie péridurale > 6 h (CR: 9,1; P = 0,001) était un facteur de risque d’insuffisance pendant le travail alors qu’une durée < I h était associée à un risque accru d’échec lors de l’expulsion (CR: 18,3; P = 0,001).
Conclusion
Plusieurs facteurs obstétricaux ou liés à la technique péridurale sont asssociés à un risque accru d’analgésie inadéquate. Pour certains facteurs techniques, des modifications simples des pratiques pourraient conduire à une amélioration notable de l’analgésie.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Morgan B, Bulpitt CJ, Clifton P, Lewis PJ. Effectiveness of pain relief in labour: survey of 1000 mothers. BMJ 1982; 285: 689–90.
Robinson JO, Rosen M, Evans JM, Revill SI, David H, Rees GAD. Maternal opinion about analgesia for labour. A controlled trial between epidural block and intramuscular pethidine combined with inhalation. Anaesthesia 1980; 35: 1173–81.
D’Angela R, Berkebile BL, Gerancher JC. Prospective examination of epidural catheter insertion. Anesthesiology 1996; 84: 88–93.
Collier CB. Why obstetric epidurals fail: a study of epidurograms. International Journal of Obstetric Anesthesia 1996; 5: 19–31.
Cruchley PM, Rose K. Supplemental analgesic requirements with continuous epidural infusion: patient profiles. Can J Anaesth 1994; 41: A30.
D’Angelo R, Foss ML, Livesay CH. A comparison of multiport and uniport epidural catheters in laboring patients. Anesth Analg 1997; 84: 1276–9.
Tanaka K, Watanabe R, Harada T, Dan K. Extensive application of epidural anesthesia and analgesia in a University Hospital: incidence of complications related to technique. Reg Anesth 1993; 18: 34–8.
Sharrock NE, Urquhart B, Mineo R. Extradural anaesthesia in patients with previous lumbar spine surgery. Br J Anaesth 1990; 65: 237–9.
Valentine SJ, Jarvis AP, Shutt LE. Comparative study of the effects of air or saline to identify the extradural space. Br J Anaesth 1991; 66: 224–7.
Narang VPS, Linter SPK. Failure of extradural blockade in obstetrics. A new hypothesis. Br J Anaesth 1988; 60: 402–4.
Withington DE, Weeks SK. Repeat epidural analgesia and unilateral block. Can J Anaesth 1994; 41: 568–71.
Ueda W, Kataoka Y, Takimoto E, et al. Ephedrine-induced increases in arterial blood pressure accelerate regression of epidural block. Anesth Analg 1995; 81: 703–5.
Mogensen T, Simonsen L, Scott NB, Henriksen JH, Kehlet H. Tachyphylaxis associated with repeated epidural injections of lidocaine is not related to changes in distribution or the rate of elimination from the epidural space. Anesth Analg 1989; 69: 180–4.
Savolaine ER, Pandya JB, Greenblatt SH, Conover SR. Anatomy of the human lumbar epidural space: new insights using CT-epidurography. Anesthesiology 1988; 68: 217–20.
Dalens B, Bazin J-E, Haberer J-P. Epidural bubbles as a cause of incomplete analgesia during epidural anesthesia. Anesth Analg 1987; 66: 679–83.
Bonica JJ, McDonald JS. The pain of childbirth.In: Bonica JJ (Ed.). The Management of Pain, Vol II, 2nd ed. Philadelphia: Lea & Febiger, 1990: 1313–43.
Lysak SZ, Eisenach JC, Dobson CE II. Patient-controlled epidural analgesia during labor: a comparison of three solutions with a continuous infusion control. Anesthesiology 1990; 72: 44–9.
Russell R, Quinlan J, Reynolds F. Motor block during epidural infusions for nulliparous women in labour. A randomized double-blind study of plain bupivacaine and low dose bupivacaine with fentanyl. International Journal of Obstetric Anaesthesia 1995; 4: 82–8.
Russell R, Groves P, Reynolds F. Is opioid loading necessary before opioid/local anaesthetic epidural infusions? A randomized double-blind study in labour. International Journal of Obstetric Anaesthesia 1993; 2: 78–84.
Eappen S, Segal S, Blinn A, Datta S. Replacement rate and etiologic factors associated with inadequate block during epidural analgesia in parturients (Abstract). Reg Anesth 1995; 20(Suppl): 69.
Morgan B. Analgesia in labour.In: Morgan BM (Ed.). Foundations of Obstetric Anaesthesia. London: Farrand Press, 1987: 50–68.
Wuitchik M, Bakal D, Lipshitz J. The clinical significance of pain and cognitive activity in latent labor. Obstet Gynecol 1989; 73: 35–42.
Curatolo M, Orlando A, Zbinden AM, Scaramozzino P, Venuti FS. A multifactorial analysis to explain inadequate surgical analgesia after extradural block. Br J Anaesth 1995; 75: 274–81.
Melzack R. The myth of painless childbirth (The John J. Bonica lecture). Pain 1984; 19: 321–37.
Ranta F, Jouppila P, Spalding M, Jouppila R. The effect of maternal obesity on labour and labour pain. Anaesthesia 1995; 50: 322–6.
Janes EF, McCrory JW. The loading dose in continuous infusion extradural analgesia in obstetrics. Br J Anaesth 1991; 67: 323–5.
Cohen SE, Tan S, Albright GA, Halpern J. Epidural fentanyl/bupivacaine mixtures for obstetric analgesia. Anesthesiology 1987; 67: 403–7.
Van Steenberge A, Debroux HC, Noorduin H. Extradural bupivacaine with sufentanil for vaginal delivery. A double-blind study. Br J Anaesth 1987; 59: 1518–22.
Dubost T, Coltat JC, Roulier JP, et al. Maternal satisfaction with patient-controlled extradural analgesia during labour: results of a 6-month survey (500 questionnaires) (Abstract). Br J Anaesth 1996; 76(Suppl 2): A328.
Collis RE, Davies DWL, Aveling W. Randomised comparison of combined spinal-epidural and standard epidural analgesia in labour. Lancet 1995; 345: 1413–6.
Abouleish A, Abouleish E, Camann W. Combined spinalepidural analgesia in advanced labour. Can J Anaesth 1994; 41: 575–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Le Coq, G., Ducot, B. & Benhamou, D. Risk factors of inadequate pain relief during epidural analgesia for labour and delivery. Can J Anaesth 45, 719–723 (1998). https://doi.org/10.1007/BF03012140
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012140