
Abstract
Background
In response to growing evidence that proper performance of operative techniques during cancer surgery is associated with improved patient outcomes, the American College of Surgeons (ACS) implemented six operative standards as part of Commission on Cancer (CoC) accreditation. This study aimed to assess surgeon familiarity with these standards when first introduced and 2 years after their adoption.
Methods
The ACS Cancer Surgery Standards Program distributed an anonymous 36-question survey to CoC-accredited cancer programs in 2021 and 2023. Questions specific to operative techniques determined the Surgery Score, and those specific to the accreditation standards determined the Standards Score. Mean scores were compared using one-way analysis of variance (ANOVA) and t tests.
Results
The survey was completed by 376 surgeons in 2021 and 380 surgeons in 2023. The Surgery Scores were higher than the Standards Scores in 2021 and 2023. The surgeons who practiced at institutions with CoC accreditation had significantly higher Standards Scores than the surgeons at non-accredited institutions in 2021 (p = 0.005) and 2023 (p = 0.004), but not significantly different Surgery Scores.
Conclusions
The baseline survey in 2021 demonstrated significant knowledge of technical aspects of cancer surgery among a broad surgeon base, but a need for greater understanding of the accreditation standards. The repeat survey distribution 2 years after rollout of the operative standards and associated educational programing showed increased awareness surrounding the operative standards in 2023 and a trend toward improvement in knowledge of the accreditation standards across all specialties. Further evaluation will be directed toward compliance with the accreditation standards.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Cancer outcomes are dependent on timely diagnosis, appropriate medical decision-making, and multidisciplinary care, often including surgical intervention. For solid tumors, surgery remains a mainstay in curative therapy, but until recently, guidelines outlining the critical technical elements associated with optimal oncologic outcomes had not been described.
The American College of Surgeons (ACS) Cancer Research Program defined evidence-based operative standards to guide cancer surgery, which were published in the Operative Standards for Cancer Surgery (OSCS) volumes 1, 2, and 3.1,2,3 This provided a framework for surgeons to reference regarding high-quality operative techniques with a known impact on oncologic outcomes. Furthermore, growing evidence supported this assertion in breast, gastric, and lung cancer, highlighting the importance of focusing on surgical techniques to promote quality cancer care.4,5,6
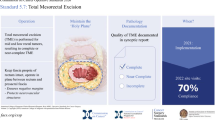
In June 2020, the American College of Surgeons (ACS) launched the Cancer Surgery Standards Program (CSSP) to further develop and implement operative standards to improve the quality of surgical cancer care in the United States. That same year, six of the operative standards were adopted by the Commission on Cancer (CoC) for program accreditation, thereby rapidly operationalizing and introducing the OSCS into direct patient care on a large scale. The CoC Operative Standards 5.3–5.8 (Fig. 1), describe technical elements required for specific operations as well as documentation of those elements in a synoptic format and refer to the following operations performed for curative intent: sentinel node biopsy for breast cancer, axillary dissection for breast cancer, wide local excision for melanoma, colon cancer resection, total mesorectal excision for low- to mid-rectal cancer, and pulmonary resection for lung cancer.3,7

Summary of the Commission on Cancer (CoC) Operative Standards 5.3-5.8.
During the past several decades, guidelines and algorithms have helped standardize multidisciplinary cancer care, and although the decision for or against surgical resection generally is covered in the treatment algorithms, the technical aspects of cancer surgery are often overlooked. The CoC Operative Standards fill this gap in cancer care by providing evidence-based guidelines for the technical aspects of cancer surgery. Because a large majority of hospitals across the United States are CoC-accredited, this comprises a large audience of surgeons who practice cancer surgery in the United States and may help set the standard of practice for cancer surgeons.
Understanding baseline awareness regarding the CoC Operative Standards will be critical to identify gaps in knowledge, improve implementation of the standards, and ultimately aid with standardizing surgical cancer care across institutions. Our group conducted a study to assess surgeon familiarity with the newly adopted CoC Operative Standards in 2021. The purpose of the current study was to evaluate the impact of ongoing standards-directed educational efforts through repeat familiarity assessment and to identify any change in surgeon familiarity with the standards between 2021 and 2023.
Methods
An anonymous 36-question electronic survey was distributed between April and May 2021, then again between April and May 2023 to surgeons performing cancer operations across the United States. The survey was distributed to all CoC-accredited programs (approximately 1400) in 2021 and 2023. The survey was distributed via email to cancer liaison physicians (physician quality leader of the Cancer Committee at each CoC-accredited facility who communicates with the CoC), registrars, and administrative staff at CoC-accredited cancer programs, who were asked to forward the email to surgeons at their facility. The survey also was shared via ACS Cancer Programs’ social media and promoted several times in the Cancer Programs News, a weekly newsletter with a distribution list that includes all registered staff at CoC-accredited cancer programs. Finally, the survey was promoted during meetings of the ACS state chairs and cancer liaison physicians.
Surgeons self-reported types of cancer treated in their practice (breast, melanoma, colorectal, and/or lung) and received questions relevant to their discipline(s). The survey included questions to assess overall perceptions of the standards as well as questions based on respondents’ specialty (melanoma, colorectal, breast, and/or lung) to test knowledge of particular operative techniques required for accreditation. Although each of the operative standards was developed using evidence-based guidelines for each operation, the CoC Operative Standards include additional reporting requirements for accreditation.
The questions in the survey pertaining to cancer surgery principles were used to calculate the Surgery Score, and questions pertaining to accreditation requirements were used to calculate the Standards Score. Survey responses and associated scores were compared between 2021 and 2023 to assess for any change over time in surgeon familiarity with the CoC Operative Standards.
Statistical Analysis
Surgeon demographics and surgeon perceptions regarding the CoC Operative Standards and knowledge of the standards were compared between the 2021 and 2023 surveys. Because the surveys were anonymous, the scores were not matched by surgeon. The chi-square test or Fisher’s exact test was used for univariate comparison of categorical variables. Average Surgery Scores, Standards Scores, and composite scores were compared between the 2021 and 2023 surveys. A Kruskal-Wallis equality-of-populations rank test was used to compare the median of continuous variables. The Wilcoxon rank-sum test was used to compare the median of continuous variables without equal variances.
Stata statistical software (SE 16.1; StataCorp LP, College Station, TX, USA) was used for statistical analyses. All p values were two-tailed, and a p value lower than 0.05 was considered significant.
Results
Surgeon Demographics
The survey was completed by 376 surgeons in 2021 and 380 surgeons in 2023. The demographics of the survey respondents did not differ significantly between the years (Table 1). The respondents had a wide distribution of years in practice, practice type, practice location, and geographic region of practice. Practice types were categorized as academic hospital-based (32.9% in 2021 vs 36.2% in 2023), non-academic hospital-based (49.1% in 2021 vs 47.9% in 2023), government/military (4.0% in 2021 vs 3.7% in 2023), and independent private practice (11.7% in 2021 vs 9.4% in 2023).
In terms of practice location, 43.8% of the surgeons in 2021 and 39.6% of the surgeons in 2023 practiced in an urban setting, 43.5% in 2021 and 45.6% in 2023 practiced in a suburban setting, and 12.2% in 2021 and 14.5% in 2023 practiced in a rural setting. Approximately 89% of the respondents practiced within a program that had ACS CoC accreditation (although the survey was distributed primarily to hospitals with CoC accreditation, some surgeons at non–CoC-accredited centers also accessed the survey through the ACS Cancer Program’s social media distribution). The majority of the respondents were members of their hospital’s cancer committee (72.9% in 2021 vs 69.5% in 2023) (Table 1).
Significant changes in surgeon awareness and perceptions regarding the CoC Operative Standards between 2021 and 2023 were observed (Table 2). In 2023, 87.2% responded that they were informed of the six operative standards versus 73.5% in 2021 (p < 0.001). When asked about the potential impact that the standards may have on their surgical practice, the answers showed no significant difference between the years, and the majority (55.2% in 2021 vs 56.4% in 2023) noted that the standards would result in minimal change to their surgical practice.
Surgery Scores and Standards Scores
When the survey was first distributed in 2021, the Surgery Scores pertaining to the technical aspects of the surgery and cancer surgery principles were significantly higher than the Standards Scores pertaining to the details of the accreditation standards among all specialties (84.4% vs. 62.0%; p < 0.001). The results of the survey in 2023 demonstrated that the Surgery Scores again were significantly higher than the Standards Scores (86.3% vs. 66.7%; p < 0.001), but overall improvement in the Standards Scores was observed between 2021 and 2023 (62.0% vs 66.7%; p = 0.04).
In a comparison between cancer specialties, melanoma surgeons had the highest Surgery Score in 2021 (90%), whereas breast surgeons had the highest Surgery Score in 2023 (90.5%) (Table 3). None of the Surgery Scores for any of the cancer specialties changed significantly between 2021 and 2023. Thoracic surgeons were found to have the highest Standards Score in both 2021 ((74.4%) and 2023 (86.0%), but breast surgeons (the specialty with the second highest Standards Scores in both years) represented the only specialty with significant improvement in the Standards Score between 2021 and 2023 (66.7% vs 70.2%; p < 0.001). Furthermore, the surgeons who answered the questions for only one specialty scored higher Surgery Scores and Standards Scores than the surgeons who answered the questions for multiple disease sites in both 2021 and 2023 (Tables 4 and 5).
A closer look at surgeon/practice demographics showed that years in practice, practice location, and geographic region of practice had no impact on the Surgery Scores or Standards Scores in 2021 or 2023 (Tables 4 and 5). Practice type, however, was found to have a significant association with the scores. Compared with non-academic practice, academic practice was associated with higher Surgery Scores in 2021 (83.3% vs 88.2%; p = 0.01) and in 2023 (85.3% vs 89.2%; p = 0.01). The Standards Scores were higher for those in academic practice in 2021 (58.0% vs 66.7%; p = 0.03), but were not significantly higher in 2023 (65.7% vs 69.2%; p = 0.40). The surgeons who practiced at institutions with ACS CoC accreditation had significantly higher Standards Scores than the surgeons at non-accredited institutions in both 2021 (p = 0.005) and 2023 (p = 0.004), but not significantly different Surgery Scores. Similarly, the surgeons who were members of their institution’s cancer committee had significantly higher Standards Scores in both 2021 (p = 0.04) and 2023 (p = 0.001).
Discussion
Following the 2021 survey of surgeons who performed cancer operations in the United States, we found that Surgery Scores representative of knowledge regarding technical aspects of cancer surgery were consistently high across specialties, but Standards Scores representative of knowledge regarding the COC accreditation standards were consistently lower and varied significantly across specialties. We recognized a clear need for improved understanding of the details of the CoC accreditation standards. These results informed the implementation of several educational tools, including webinars, editorials, visual abstracts, and other strategies, geared toward addressing this knowledge gap.
The survey results obtained 2 years after rollout of the CoC Operative Standards and the associated educational programing showed increased awareness among surgeons in 2023. Specifically, we saw a trend toward improvement in Standards Scores across all specialties, with a significant improvement observed when all the survey participants were evaluated. By 2023, we also were able to close the gap in the Standards Scores between surgeons at academic versus non-academic centers, with significant improvement in overall awareness of the CoC accreditation standards at non-academic centers. Our findings suggest that our educational programming and outreach efforts have been successful in reaching various practice types, and we hope the increased awareness of the CoC Operative Standards will ultimately improve standardization of cancer surgery.
Although these results are encouraging, there remain areas for improvement in our educational efforts. Both the 2021 and 2023 survey responses showed significant differences in performance between various cancer specialties. Colorectal surgeons scored significantly lower Surgery Scores and Standards Scores compared with other specialties in both 2021 and 2023. With regard to Standards Scores, thoracic surgeons had significantly higher Standards Scores compared to other specialties in both 2021 and 2023. Further investigation into how each of the CoC Operative Standards is implemented within each specialty and collaboration with specialty-specific societies may shed light on the differences in knowledge of the CoC standards among the various specialties.
Among each of the specialty groups, there was no significant difference in the Surgery Score between the 2021 and 2023 surveys, although the scores were quite high at baseline. Interestingly, the breast surgical oncology cohort showed a significant increase in the Standards Score from 2021 to 2023. This increase in awareness of the CoC accreditation standards within the breast specialty may have been due in part to the simultaneous rollout of the National Accreditation Program for Breast Centers (NAPBC) standards, which included CoC Standards 5.3 and 5.4 pertaining to breast cancer. We also found that the surgeons specializing in one disease site consistently had higher Surgery Scores and Standards Scores than the surgeons who work on multiple disease sites. Partnering with organizations within each specialty will be critical for widening our reach and improving awareness surrounding each of the standards.
The ACS Cancer Surgery Standards Program has led a large-scale effort to increase awareness of the CoC Operative Standards to aid with ultimate implementation of the standards across institutions. Understanding baseline awareness and perceptions regarding the CoC Operative Standards is critical to identifying gaps in knowledge and developing implementation strategies.
Implementation science is the study of methods and strategies to promote adoption of evidence-based practices into routine practice.8,9 The implementation science framework most often includes stages of exploration, installation, implementation, and expansion.8,9 The 2013 Institute of Medicine report deemed the system of cancer care delivery in a state of crisis given the increased demand for cancer care at a time of exponential advancement in cancer research and increasing complexity of management.10
Given the rapid changes in cancer treatment, translating important research into the health care setting is a slow and challenging process.11,12 The lack of significant change in the Surgery Scores and Standards Scores in our study between 2021 and 2023 highlights the challenging nature of integrating new practices into routine clinical care. The scores demonstrate a need for further education through both passive modes of implementation and dissemination of evidence-based practices such as publication in journals and development of consensus statements, as well as more active modes of dissemination such as webinars and interactive sessions that engage the target audience.
Our study had several limitations that must be taken into account. The study was survey-based, which resulted in inherent selection bias. The vast majority of respondents were from CoC-accredited centers, so the results may not be completely generalizable to the general population of surgeons across the United States. However, a large portion of U.S. hospitals have CoC accreditation for cancer care. Furthermore, the results may overestimate awareness of the CoC Operative Standards because surgeons unaware of the standards may have chosen not to complete the survey. It was encouraging that the survey was completed by a similar number of surgeons in 2021 and 2023, suggesting that interest in the topic did not wane. However, the same surgeons may not have completed the survey both years, so we cannot draw direct comparisons of changes in awareness and knowledge.
Finally, although the surveys were distributed to all CoC-accredited programs (approximately 1400) in 2021 and 2023), we do not have the data to note exactly what proportion of cancer programs across the country are accredited by the CoC or what proportion of cancer surgeons this study represents. However, the National Cancer Data Base (NCDB) holds a 74.3% coverage rate across all reported cancer cases within the United States,13 exemplifying a high level of representation, and because NCDB data are obtained primarily from CoC-accredited programs, we can extrapolate that the survey data provide a similar representation of cancer surgeons in the United States.
Conclusions
The CoC Operative Standards were established in an effort to standardize the technical aspects of cancer surgery across institutions such that patients may receive comparable quality, evidence-based cancer surgery regardless where they are treated. Our baseline survey in 2021 demonstrated significant knowledge of the technical aspects of cancer surgery among a broad surgeon base but a need for greater understanding of the details of the CoC accreditation standards. Repeat survey distribution 2 years after the rollout of the CoC Operative Standards and the associated educational programing showed increased awareness surrounding the Operative Standards in 2023 and a trend toward improvement in knowledge of the accreditation standards across all specialties.
These data will focus ongoing efforts to increase uptake of the Operative Standards among cancer surgeons more broadly in the U.S. surgical trainees and global partners and establish a standard of care for the technical aspects of cancer surgery. Further educational efforts and evaluation will be directed toward compliance with the accreditation standards supporting the standardization of cancer surgery across institutions and improved patient outcomes.
References
Operative Standards for Cancer Surgery: Volume 1: Breast, Lung, Pancreas, Colon. 1 ed. Vol. 1. 2015: Lippincott William & Wilkins.
Operative Standards for Cancer Surgery: Volume II: Thyroid, Gastric, Rectum, Esophagus, Melanoma. 1 ed. Vol. 2. 2018: Lippincott Williams & Wilkins.
Katz MHG, et al. Technical standards for cancer surgery: commission on Cancer Standards 5.3–5.8. Ann Surg Oncol. 2022;29:6549–58.
Zhao B, et al. Adherence to surgical and oncologic standards improves survival in breast cancer patients. J Surg Oncol. 2019;120:148–59.
Zhao B, et al. Adherence with operative standards in the treatment of gastric cancer in the United States. Gastric Cancer. 2020;23:550–60.
Osarogiagbon RU, et al. Prognostic value of National Comprehensive Cancer Network lung cancer resection quality criteria. Ann Thorac Surg. 2017;103:1557–65.
Surgeons ACo. Optimal Resources for Cancer Care (2020 Standards). 2023 June 2023 [cited 2023.
Eccles MP, et al. An implementation research agenda. Implement Sci. 2009;4:18.
Eccles MP, et al. Implementation science six years on: our evolving scope and common reasons for rejection without review. Implement Sci. 2012;7:71.
Spinks T, et al. Delivering high-quality cancer care: the critical role of quality measurement. Healthc Amst. 2014;2:53–62.
Nutbeam D. Improving the fit between research and practice in health promotion: overcoming structural barriers. Can J Public Health. 1996;87(Suppl 2):S18-23.
Green LW, et al. Diffusion theory and knowledge dissemination, utilization, and integration in public health. Annu Rev Public Health. 2009;30:151–74.
Palis BE, Janczewski LM, Browner AE, Cotler J, Nogueira L, Richardson LC, et al. National Cancer Database conforms with standardized framework for registry and data quality. Ann Surg Oncol. 2024. https://doi.org/10.1245/s10434-024-15393-8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Zaveri, S., Teshome, M., Reyna, C. et al. Assessing Surgeon Familiarity with the Commission on Cancer Operative Standards for Cancer Surgery. Ann Surg Oncol 31, 6378–6386 (2024). https://doi.org/10.1245/s10434-024-15624-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-024-15624-y