
Abstract
Background
We aimed to describe the effect of preoperative sarcopenia on oncologic outcomes of organ-confined renal cell carcinoma (RCC) after radical nephrectomy.
Patients and Methods
A total of 632 patients with pT1–2 RCC who underwent radical nephrectomy between 2004 and 2014 were retrospectively analyzed. From preoperative computerized tomography (CT) scans, skeletal muscle index (SMI) was measured and gender-specific cutoff values at third lumbar vertebra of 52.4 cm2/m2 for men and 38.5 cm2/m2 for women were used to define sarcopenia. Survivals were compared and associations with sarcopenia were analyzed using Kaplan–Meier log rank tests and Cox proportional hazard regression models. Median follow-up was 83 months.
Results
Of 632 patients, 268 (42.4%) were classified as sarcopenic. The sarcopenic group was more advanced in age (57 versus 53 years) and more predominantly male (71.3% versus 59.9%). Sarcopenic patients had lower body mass index (BMI, 23.0 versus 25.9 kg/m2), but there was no difference in tumor size, stage, or nuclear grade. Sarcopenia was associated with poorer overall survival (OS) and cancer-specific survival (CSS; OS 94.0% versus 82.1%; p < 0.001 and CSS 97.5% versus 91.8%; p < 0.001). On multivariate analysis, sarcopenia was an independent risk factor for all-cause mortality [hazard ratio (HR) 2.58; 95% CI 1.02–6.54] and cancer-specific mortality (HR 3.07; 95% CI 1.38–6.83).
Conclusions
Sarcopenia at diagnosis was an independent risk factor for all-cause and cancer-specific mortality after radical nephrectomy for pT1–2 RCC. These findings underscore the importance of assessing presence of sarcopenia for risk stratification even among surgical candidates.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Renal cell carcinoma (RCC) is a fatal urologic malignancy that accounts for 2–3% of all adult malignancies. Statistical analysis conducted in the USA observed 58,000 newly diagnosed patients and approximately 13,000 deaths from RCC every year.1 Surgical resection is the standard treatment for localized RCCs. However, 30% of patients experience recurrence or metastasis after radical nephrectomy.2 Therefore, identifying prognostic factors for the recurrence and mortality of RCCs, and refining prognostic models to provide more accurate scope for patient follow-up and timely interventions, have been at the heart of RCC research.
Sarcopenia is defined as a progressive decline in skeletal muscle mass and is alleged to be associated with increased risk of falls and fractures, disabilities, and subsequent death.3 Recent studies have demonstrated that adverse outcomes of multiple malignancies, including breast, colorectal, pancreatic, and hepatobiliary cancer, as well as urothelial carcinoma of the bladder, were associated with sarcopenia.4,5,6 In RCC, the impact of sarcopenia on patients with metastatic disease undergoing cytoreductive nephrectomy, and its possible use as a prognostic factor, has been demonstrated in recent literature.7 In another study on patients with metastatic RCC treated with tyrosine-kinase inhibitors, sarcopenia and decreased muscle mass after initiation of the therapy were associated with poor survival and lower objective response rate.8 The prognostic implication of sarcopenia at diagnosis in nonmetastatic RCC patients undergoing radical nephrectomy has been described in one retrospective cohort study, in which sarcopenia was demonstrated to be associated with disease progression and RCC-related and all-cause mortality.9 However, the study cohort was a vastly heterogeneous group of patients including all patients from stage I to IV. To better understand the presence and significance of the impact of sarcopenia on RCC prognosis, we limited our cohort to localized RCC, and aimed to identify the impact of sarcopenia before surgery on oncologic outcomes after radical nephrectomy.
Patients and Methods
Patient Selection
Among 1623 patients who were diagnosed with stage I–II RCC following radical nephrectomy at our institution between January 2004 and December 2014, 756 patients with organ-confined RCC were identified. From this cohort, 16 patients without follow-up beyond 1 year, 28 patients undergoing hemodialysis due to end-stage renal disease, 76 patients with nondigital preoperative CT images not compatible with our digital imaging and communications in medicine (DICOM) system, and 4 patients with metal braces implanted in their lumbar spines hindering accurate measurement of the axial skeletal muscle area were excluded, leaving 632 patients in the final analysis (Supplementary Fig. 1). The design of this study and use of patient medical record data was approved by the institutional review board (IRB approval number 2019-0995).
Pathology was assigned according to 2009 UICC/AJCC TNM staging. Following surgery, patients were followed periodically according to the institutional protocol; physical examination, chest x-ray, CT scan of abdomen and pelvis, and blood tests were repeated biannually for the first two years, and yearly thereafter. In these patients, demographic (age, gender, BMI, performance status), clinical (diabetes, hypertension, chronic kidney disease, etc.), and surgical/pathologic characteristics were reviewed. In the follow-up data, disease progression, defined as tumor recurrence at nephrectomy site, lymph nodes, and/or distant metastasis on either radiographic or nuclear imaging studies, was investigated.
Skeletal Muscle Index
The areas of the lumbar skeletal muscle components (including the psoas, quadratus lumborum, erector spinae, bilateral internal, external, lateral oblique muscles, and rectus abdominis) were measured on a single axial CT image of third lumbar spine at the transverse process level, using attenuation thresholds of −29 to +150 Hounsfield units (Supplementary Fig. 2). Measurement was done by a single investigator (J.L.), in accordance with previously described standard methodology using CoreSlicer, an open-source web-based analytic morphomics tool.10,11 Cross-sectional areas (cm2) were normalized for height (m2) to calculate skeletal muscle index at L3 level (L3 SMI). A gender-specific criterion of 52.4 cm2/m2 for men and 38.5 cm2/m2 for women, which showed optimum stratification in a prior population-based study, was used to define sarcopenia.12
Statistical Analysis
Categorizing patients into sarcopenic and nonsarcopenic groups, Student’s t-test and Pearson’s chi-square and Fisher’s exact tests were used to compare continuous and categorical variables, respectively. Overall survival (OS), cancer-specific survival (CSS), and progression-free survival (PFS) after surgery were analyzed and compared using the Kaplan–Meier method with log-rank test. Associations of individual clinical covariates with disease progression and cancer-specific mortality were assessed by Cox proportional hazards regression model. For all-cause mortality, a cause-specific hazards model with competing risks analysis was done. All statistical analysis was performed with IBM SPSS Statistics version 25 (IBM SPSS, Armonk, NY), and p < 0.05 was considered significant.
Results
Patient Characteristics
Median L3 SMI of the 632 patients was 49.2 cm2/m2, and 268 (42.4%) patients were classified as sarcopenic (Table 1). The sarcopenic group was more advanced in age (57 versus 53 years) and predominantly male (71.3% versus 59.9%). Sarcopenic patients also had significantly lower BMI (23.0 versus 25.9 kg/m2). However, with respect to all other clinicopathological variables, including tumor size, stage, and nuclear grade, there was no difference between the groups.
Correlations of L3 SMI with Age and BMI
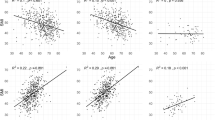
L3 SMI was correlated with several clinical values. Median L3 SMI was 53.4 cm2/m2 (IQR 48.7, 58.6 cm2/m2) in men and 42.3 cm2/m2 (IQR 37.4, 45.5 cm2/m2) in women. Mean L3 SMI was significantly higher in men (53.6 versus 41.7 cm2/m2), justifying gender-stratified analysis. On linear regression, significant negative correlation was observed between L3 SMI and age (R2 = 0.031, p < 0.001) and significant positive correlation was observed with BMI (R2 = 0.301, p < 0.001) (Fig. 1).

Relationship between L3SMI and age and BMI, in all (A1, A2), male (B1, B2), and female (C1, C2) patients
Survival Analysis
During median follow-up of 83 months (IQR 59, 111 months), 92 (14.6%) patients had experienced recurrence and 31 (4.9%) of those patients had died due to RCC-related causes. Actuarial 5- and 10-year OS were 97.1% and 96.7%, respectively, for the nonsarcopenic group. For the sarcopenic group, they were 90.6% and 89.0%, respectively, and significantly lower than for the nonsarcopenic group (Fig. 2). Similarly, 5- and 10-year CSS were significantly higher in the nonsarcopenic group (98.8% versus 92.0% at 5 years, 94.1% versus 93.4% at 10 years; p < 0.001). However, PFS was similar at both 5 and 10 years.

Survival of patients with organ-confined renal cell carcinoma following radical nephrectomy according to sarcopenia status: overall (A), cancer-specific (B), recurrence-free (C)
Prognostics of Survival
With respect to OS, age, BMI, L3 SMI, sarcopenia, pathologic stage, nuclear grade, and tumor size demonstrated statistical significance on univariate analysis. On multivariate analysis with competing risks model, sarcopenia was a significant predictor (HR, 2.58; 95% CI 1.02–6.54; p = 0.045), in addition to age and tumor size (Table 2; Supplementary Fig. 3). Similar results were obtained regarding CSS, and sarcopenia was an independent predictor after radical nephrectomy (HR, 3.07; 95% CI 1.38–6.83; p = 0.006) (Table 3). Prognostic factors regarding PFS were age, tumor size, and non-clear cell pathology, but not sarcopenia (Table 4).
Discussion
Sarcopenia is an emerging body composite indicator for risk assessment of multiple malignancies. The mechanisms and pathophysiology of sarcopenia are not yet clearly understood. Declines in hormones, numbers of neuromuscular junctions, activity, and adequate nutrition, as well as inflammation, have been suggested as possible causes. Risk factors for sarcopenia include age, gender, and level of physical activity.13 The European Working Group on Sarcopenia in Older People suggests that the diagnosis of sarcopenia be made with presence of low skeletal muscle mass and either low muscle strength or low muscle performance.3 Sarcopenia is easily measurable and is suggested to reflect relatively long-term changes of a patient’s medical condition.14
In the present study, we verified that, in patients with pT1–2 RCC, sarcopenia at diagnosis was an independent prognostic factor for overall and RCC-specific survival after radical nephrectomy. In our study, we confined the analysis to localized RCC to minimize potential confounding effects relating to advanced tumor invasiveness such as lymph node or distant metastasis, venous thrombosis, or perirenal invasion on patients’ oncologic outcomes, as several studies have suggested association between various advanced cancers and sarcopenia.15 We also excluded patients who underwent partial nephrectomy; although it is generally accepted that oncologic outcome following partial nephrectomy is comparable to radical nephrectomy, we strived to reduce confounding as controversy still persists regarding its role in patients with T1 or T2 tumors. In our cohort, we found that 42.4% of the patients classified as sarcopenic, which was in line with a previous study conducted by Prado and colleagues.9 Patients with sarcopenia tended to be older, more likely to be male, and less obese than those without sarcopenia in our study cohort.
To our knowledge, this was the first study to analyze the impact of sarcopenia in organ-confined RCC, in the largest study cohort. Psutka et al. had previously suggested poor overall and cancer-specific survival of sarcopenic patients with RCC.9 However, in their study, patients in all stages were included and advanced cancers comprised the majority (pT3 or beyond in 39% and pN1 in 8%) of the study cohort. As commented previously, the causal relationship between sarcopenia and poorer oncologic outcome in patients with advanced malignancy could entail different or additional elements; sarcopenia could be a manifestation of systemic disease and a representative of unmeasured oncologic burden, as in a paraneoplastic syndrome. We confined our analysis to pathologically organ-confined RCC patients to reduce such confounding. Alternatively, sarcopenia could be a reflection of poorer performance status representing patients unfit from receiving aggressive treatments. Treatment strategy and outcome vary significantly according to the patient performance status, especially in patients with metastatic disease.16 To eliminate this possibility, our analysis was done in a surgical cohort and all patients had Eastern Cooperative Oncology Group (ECOG) performance 0 or 1. Notably, even in our surgical cohort, 42.4% of the patients were classified as sarcopenic; 65 of the 289 patients with BMI > 25 kg/m2 were sarcopenic, suggesting that sarcopenia can be a more meaningful parameter in further discriminating the patients in the prognostication models.
Tumor stage and Fuhrman nuclear grade are thought to be the most important prognostic factors for patients with localized RCC. Unfortunately, studies revealed that TNM staging and Fuhrman nuclear grade alone are not sufficient to accurately predict outcomes of an individual patient.17 Several prognostic nomograms for localized RCC adding variables such as performance status, RCC-related symptoms, tumor necrosis, blood cell counts, and serum chemical markers have been proposed over the years to improve predictive accuracy up to 80–89% in validation studies.18,19,20,21 To further improve accuracy in predicting patient outcomes, inflammatory markers, including neutrophil–lymphocyte ratio and serum C-reactive protein (CRP), as well as various molecular biomarkers have been explored.19,20,22 BMI may be a similar parameter to sarcopenia, and its impact on overall and progression-free survival in patients with RCC has been previously documented.23 In our study, BMI was a significant prognostic of OS and CSS on univariate, but not on multivariate, analysis. We speculate that, while BMI showed a strong positive correlation with L3 SMI, a substantial portion of overweight patients (BMI > 25 kg/m2) were still classified as sarcopenic, underscoring the significance of muscle mass and its precise measurement.
The limitations of our study are mainly related to its retrospective study design; possible selection bias may have affected our results. Incomplete data precluded us from including into the analysis a systematic and detailed information on comorbidity burden. Also, pathological nuclear grading followed the Fuhrman system, which was the institutional protocol until after 2014 when it was replaced by the ISUP/WHO system. Our study cohort only included observations from a single tertiary referral center. As a tertiary institution, patients were often referred to local institutions for follow-ups, which may have caused underestimation of recurrence. Also, sarcopenia was defined only by the L3 skeletal muscle index. Muscle mass is only one of the original definitions of sarcopenia, and accurate diagnosis should include a decrease in physical performance as well. While the measurement method was the most widely accepted method, the gender-specific cutoffs we used to define sarcopenia was from the study by Prado and colleagues12 as there were no criteria for Asian or Korean populations except for studies with different muscle measurement24 or with different measurement methodology.25 Finally, we have failed to demonstrate the quantitative effect of sarcopenia on oncologic outcomes. Further study investigating dose relationship and validating optimal criteria for sarcopenia could help accurately define its role in oncologic outcomes of RCC.
Conclusions
Sarcopenia, assessed by preoperative CT imaging, in addition to age at surgery and tumor size, was an independent risk factor for survival in patients undergoing radical nephrectomy for pT1–2 RCC. Specifically, in surgical candidates with organ-confined cancers, sarcopenia could be a significant parameter to consider in addition to the preexisting prognostic models.
Abbreviations
- BMI:
-
Body mass index
- CSS:
-
Cancer-specific survival
- CT:
-
Computed tomography
- OS:
-
Overall survival
- PFS:
-
Progression-free survival
- RCC:
-
Renal cell carcinoma
- SMI:
-
Skeletal muscle index
References
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300.
Golimbu M, Joshi P, Sperber A, Tessler A, Al-Askari S, Morales P. Renal cell carcinoma: survival and prognostic factors. Urology. 1986;27:291–301.
Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on definition and diagnosis: report of the European Working Group on Sarcopenia in Older People. Age Ageing. 2010;39:412–23.
Psutka SP, Carrasco A, Schmit GD, et al. Sarcopenia in patients with bladder cancer undergoing radical cystectomy: impact on cancer-specific and all-cause mortality. Cancer. 2014;120:2910–8.
Mir O, Coriat R, Blanchet B, et al. Sarcopenia predicts early dose-limiting toxicities and pharmacokinetics of sorafenib in patients with hepatocellular carcinoma. PLoS ONE. 2012;7:e37563.
Del Fabbro E, Parsons H, Warneke CL, et al. The relationship between body composition and response to neoadjuvant chemotherapy in women with operable breast cancer. Oncologist. 2012;17:1240–5.
Sharma P, Zargar-Shoshtari K, Caracciolo JT, et al. Sarcopenia as a predictor of overall survival after cytoreductive nephrectomy for metastatic renal cell carcinoma. Urol Oncol. 2015;33(339):e317-323.
Ishihara H, Takagi T, Kondo T, et al. Effect of changes in skeletal muscle mass on oncological outcomes during first-line sunitinib therapy for metastatic renal cell carcinoma. Target Oncol. 2018;13:745–55.
Psutka SP, Boorjian SA, Moynagh MR, et al. Decreased skeletal muscle mass is associated with an increased risk of mortality after radical nephrectomy for localized renal cell cancer. J Urol. 2016;195:270–6.
Mullie L, Afilalo J. CoreSlicer: a web toolkit for analytic morphomics. BMC Med Imaging. 2019;19:15.
van der Werf A, Langius JAE, de van der Schueren MAE, et al. Percentiles for skeletal muscle index, area and radiation attenuation based on computed tomography imaging in a healthy Caucasian population. Eur J Clin Nutr. 2018;72:288–96.
Prado CM, Birdsell LA, Baracos VE. The emerging role of computerized tomography in assessing cancer cachexia. Curr Opin Support Palliat Care. 2009;3:269–75.
Santilli V, Bernetti A, Mangone M, Paoloni M. Clinical definition of sarcopenia. Clin Cases Miner Bone Metab. 2014;11:177–80.
Krishnan VS, White Z, McMahon CD, et al. A neurogenic perspective of sarcopenia: time course study of sciatic nerves from aging mice. J Neuropathol Exp Neurol. 2016;75:464–78.
Bauer JM, Sieber CC. Sarcopenia and frailty: a clinician’s controversial point of view. Exp Gerontol. 2008;43:674–8.
Ohno Y, Nakashima J, Ohori M, et al. Clinical variables for predicting metastatic renal cell carcinoma patients who might not benefit from cytoreductive nephrectomy: neutrophil-to-lymphocyte ratio and performance status. Int J Clin Oncol. 2014;19:139–45.
Kim HL, Seligson D, Liu X, et al. Using protein expressions to predict survival in clear cell renal carcinoma. Clin Cancer Res. 2004;10:5464–71.
Volpe A, Patard JJ. Prognostic factors in renal cell carcinoma. World J Urol. 2010;28:319–27.
Pichler M, Hutterer GC, Stoeckigt C, et al. Validation of the pre-treatment neutrophil-lymphocyte ratio as a prognostic factor in a large European cohort of renal cell carcinoma patients. Br J Cancer. 2013;108:901–7.
de Martino M, Klatte T, Seemann C, et al. Validation of serum C-reactive protein (CRP) as an independent prognostic factor for disease-free survival in patients with localised renal cell carcinoma (RCC). BJU Int. 2013;111:E348-353.
Crispen PL, Boorjian SA, Lohse CM, Leibovich BC, Kwon ED. Predicting disease progression after nephrectomy for localized renal cell carcinoma: the utility of prognostic models and molecular biomarkers. Cancer. 2008;113:450–60.
Nogueira M, Kim HL. Molecular markers for predicting prognosis of renal cell carcinoma. In: RM Bukowski, RA Figlin, RJ Motzer, editors. Renal cell carcinoma. Totowa, NJ: Humana Press; 2009. p. 449–71.
Albiges L, Hakimi AA, Xie W, et al. Body mass index and metastatic renal cell carcinoma: clinical and biological correlations. J Clin Oncol. 2016;34:3655–63.
Peng P, Hyder O, Firoozmand A, et al. Impact of sarcopenia on outcomes following resection of pancreatic adenocarcinoma. J Gastrointest Surg. 2012;16:1478–86.
Kim EY, Kim K, Kim YS, et al. Prevalence of and factors associated with sarcopenia in Korean cancer survivors: based on data obtained by the Korea National Health and Nutrition Examination Survey (KNHANES) 2008–2011. Nutr Cancer. 2017;69:394–401.
Acknowledgments
Source of Funding: None. This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
J.L.: data curation, formal analysis, and writing—original draft preparation. J.S.: statistical analysis, and revision draft preparation. C.S.: conceptualization, methodology, supervision, and writing—reviewing and editing. D.Y.: Methodology. I.G.J.: conceptualization. B.H.: methodology. J.H.H.: supervision. C.S.K.: validation. H.A.: conceptualization, validation, supervision, and visualization.
Corresponding author
Ethics declarations
Disclosure
None for all authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
10434_2021_10881_MOESM2_ESM.tif
Supplementary Figure 2. Examples of lumbar skeletal muscle measured on preoperative CT scans. Supplementary file 2 (TIF 944 kb)
10434_2021_10881_MOESM3_ESM.jpg
Supplementary Figure 3. Cumulative risk of all-cause mortality according to sarcopenic status. Supplementary file 3 (JPG 53 kb)
Rights and permissions
About this article

{kind=link}
Cite this article
Lee, J., Suh, J., Song, C. et al. Association Between Sarcopenia and Survival of Patients with Organ-Confined Renal Cell Carcinoma after Radical Nephrectomy. Ann Surg Oncol 29, 2473–2479 (2022). https://doi.org/10.1245/s10434-021-10881-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10881-7