
Abstract
Background
Management of patients undergoing cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CS/HIPEC) has historically favored liberal fluid administration owing to lengthy duration of surgery and hyperthermia. This practice has been challenged in recent years with studies demonstrating improved outcomes with restrictive fluid administration.
Methods
Patients who underwent CS/HIPEC between March 2010 and September 2018 were included for analysis. Patients who received an above-median fluid rate (high-IVF) versus below-median fluid rate (low-IVF) were compared, and multivariate analyses were performed for length of stay, 90-day unplanned readmissions, and major complications.
Results
The 167 patients had a mean age of 56.7 ± 11.4 years and body mass index of 29.5 ± 6.9 kg/m2. The median rate of total intraoperative crystalloid and colloid was 7.4 mL/kg/h. The low-IVF group had less blood loss (183 vs. 330 mL, p = 0.002), were less likely to need intraoperative vasopressor drip (2.4% vs. 11.9%, p = 0.018), and experienced fewer cardiac complications (2.4% vs. 10.7%, p = 0.031), pneumonias (0% vs. 6.0%, p = 0.024), and Clavien–Dindo grade 3–5 complications (14.5% vs. 33.3%, p = 0.004). Multivariate analyses identified bowel resection (HR 4.65, p = 0.0008) as a risk factor for 90-day unplanned readmission, while bowel resection, intraoperative fluid rate, and estimated blood loss were associated with increased length of stay.
Conclusion
Higher intraoperative fluid intake was associated with multiple postoperative complications and increased length of stay, and represents a potentially avoidable risk factor for morbidity in CS/HIPEC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CS/HIPEC) is performed for primary peritoneal malignancies, as well as peritoneal metastases, commonly from colorectal, appendiceal, ovarian cancers, and neoplasms, and selectively for other malignancies.1,2,3,4,5 Although these operations are now well accepted for select patients, they can be associated with high morbidity and mortality. Early results of patients undergoing CS/HIPEC at our center showed a median length of stay of 12 days, 60-day morbidity rate of 40%, and mortality rate of 2.7%,6 while data from the National Surgical Quality Improvement Program (NSQIP) found a mean hospital length of stay of 13 days, 30-day readmission rate of 11.4%, and 30-day mortality rate of 2.3%.7
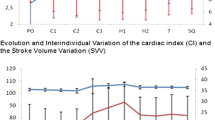
Despite gains that have resulted from refinements in technique and increasing experience at high-volume centers, these operations continue to be associated with significant morbidity. Much of the risk associated with CS/HIPEC is due to patient disease and cancer biology, which can dictate the extent of surgery and course of postoperative recovery. However, controllable factors such as fluid administration can play a role by causing tissue edema in the proinflammatory postoperative state, and result in end-organ dysfunction.8 Hemodynamic changes during CS/HIPEC can be expected as prominent fluid shifts occur as a result of resuscitation, especially during HIPEC.9,10,11,12 In vivo measurements have shown transient decrease in hepatic blood flow,13 increase in cardiac index, and decrease in stroke volume variation during HIPEC.9,10,11,12
The optimal strategy for intraoperative fluid management is a topic of substantial debate. An international survey of high-volume CS/HIPEC surgeons found that the most common measure for adequacy of intraoperative fluid optimization was urine output (95%), followed by blood pressure and heart rate (86%), while only 32% used FloTrac or Vigileo monitoring.14 In addition to affecting hemodynamic parameters, HIPEC has the potential to cause renal injury through intravascular depletion, as well as direct nephrotoxicity due to platinum agents.8 Practice patterns vary greatly, with some guidelines recommending intravenous fluid (IVF) rates of 9–12 mL/kg/h and titrating to urine output of 1 mL/kg/h intraoperatively and postoperatively.8 Single-institution data from multiple centers have shown a tendency towards liberal fluid administration, with mean intraoperative fluid rates ranging from 12.3 to 15.7 mL/kg/h in standard practice.9,12,15
The benefits of restrictive administration of intravenous fluid (IVF) have been demonstrated with use of both restrictive fluid protocols and goal-directed fluid therapy (GDFT). Restrictive protocols typically define a lower starting fluid rate than standard management, with adjustments per normal practice. GDFT aims to optimize hemodynamic management based on dynamic feedback throughout surgery. Meta-analyses of randomized trials in noncardiac surgery have found that GDFT compared with standard care was associated with fewer postoperative complications, including abdominal complications, wound infections, and hypotension, with no impact on length of stay or mortality.16 A Cochrane review of randomized trials showed no significant difference in outcomes between GDFT versus restrictive fluid protocols.17 The only randomized trial evaluating intraoperative fluid administration in CS/HIPEC found that GDFT resulted in decreased rate of major abdominal complications and length of stay compared with standard management.12
In this study, we evaluated the intraoperative IVF management at our institution to identify predictors of receipt of higher fluid rate and evaluate the impact on postoperative morbidity.
Methods
CS/HIPEC Patients
This study was a retrospective analysis completed at a National Cancer Institute designated comprehensive cancer center with approval from the Institutional Review Board.
All sequential patients who underwent CS/HIPEC between March 2010 and September 2018 were included for analysis. The CS/HIPEC program was established in 2003 at our institution, and all patients included in this study are thought to be beyond the learning curve. Surgeries were performed by three high-volume CS/HIPEC surgeons. Patients who underwent multiple CS/HIPEC were allowed, and each surgery and respective postoperative course was included separately.
Patient management and decision to offer CS/HIPEC was determined by each surgeon, with input from medical and radiation oncologists, and consensus at multidisciplinary tumor board. General criteria for CS/HIPEC included disease limited to the abdomen without hematogenous metastases, Eastern Cooperative Oncology Group (ECOG) Performance Status18 Grade ≤ 2, and ability to tolerate extensive surgery. Preoperative systemic therapy and duration and restaging studies were performed according to the standard of care at the time of treatment.
Intraoperative Management
No specific intraoperative fluid protocol was in place during the time period of the study. Management of intraoperative volume status and goals for resuscitation, including choice of crystalloid, colloid, vasopressors, and blood products, were determined by discussion between the anesthesiologist and surgeon for each case. In our practice, patients typically receive a small bolus at induction, and the fluid rate is adjusted to achieve hemodynamic parameters within 20% of baseline. Urine output goal is 1 mL/kg/h during hyperthermic perfusion and 0.5 mL/kg/h during other portions of the operation. Almost all patients had an arterial line placed to enable hemodynamic monitoring, including use of the FloTrac sensor (Edwards Lifesciences, Irvine, CA). Central venous lines were uncommonly used and placed on a case-by-case basis.
Most patients underwent preoperative epidural placement, with intraoperative use at the discretion of the anesthesiologist. Postoperative management was at the discretion of each operating surgeon but with similar principles, which was formalized in a clinical pathway (CPW) to streamline postoperative care at our institution in June 2016 (Fig. 1). In general, postoperative fluids were administered with a goal urine output of 0.5 mL/kg/h, and the IVF rate was adjusted accordingly. Nasogastric tubes (NGT) were maintained until return of bowel function. Diet and oral pain medications were started after NGT removal, epidural was removed after tolerance of oral pain medications, and Foley was maintained while epidural was in place due to potential for urinary retention.

Postoperative clinical pathway for CS/HIPEC patients. Three postoperative phases of recovery with specific components for each phase. POD postoperative day, PRN pre re nata (as needed), CLD clear liquid diet, MN midnight, NPO nil per os, BRAT bananas, rice, applesauce, toast, IV intravenous, LR lactated Ringer’s, MR maintenance rate, NS normal saline, UOP urine output, DC discontinue, CVC central venous catheter, NGT nasogastric tube, ROBF return of bowel function, PT/OT physical/occupational therapy, VTE venous thromboembolism, SQH subcutaneous heparin
Data Acquisition
Data were obtained from an institutional CS/HIPEC database, including patient demographics, oncologic and surgical history, operative details, pathology, and postoperative course. The indication for surgery was defined as primary resection if no prior surgery had been performed, residual disease if prior surgery was performed but complete cytoreduction was not achieved, recurrence if there had been a disease-free interval after the initial episode of treatment, palliative if extent of disease was not anticipated to be resectable to a completeness of cytoreduction (CC) score of 0 or 1, and neoadjuvant for those undergoing HIPEC without cytoreduction with goal of clearing peritoneal disease prior to resection of the primary cancer.
Data regarding intraoperative management, including intake and output, and vasopressor use were collected from the anesthesia record. Postoperative complications were tabulated based on review of provider documentation and primary sources within the medical record including laboratory and imaging results, and graded according to the Clavien–Dindo classification.19
Statistical Analysis
Total fluid rate was calculated for all patients, accounting for intraoperative crystalloid and colloid received, normalized to units of mL/kg/h. Patients who received an above-median fluid rate (high IVF) were compared with patients who received a below-median fluid rate (low IVF). Baseline and operative characteristics and postoperative outcomes were compared using the Mann–Whitney U and Fisher’s exact tests. Multivariable logistic regression models were created for clinical outcomes of Clavien–Dindo grade 3–5 complications and 90-day unplanned readmission, and linear regression for length of stay. The variables included in the multivariate models were significantly associated with one or more outcomes of interest on univariate analyses. The most clinically relevant variable was included when collinear variables were significant. The variables identified for inclusion were age, sex, body mass index (BMI), laparoscopic-assisted versus open approach, estimated blood loss (per 100 mL), small or large bowel resection, and total intraoperative intake rate (crystalloid, colloid, and blood products, per 5 mL/kg/h). All model assumptions were verified graphically. Multivariable models were also created for the open surgery subgroup. All tests were two-sided and performed at a significance level of 0.05 using SAS version 9.4 (SAS Institute, Cary, NC).
Results
Baseline Characteristics
A total of 167 patients were identified for inclusion. The median intraoperative fluid rate, including crystalloid and colloid, was 7.4 mL/kg/h. The low-IVF group included 83 patients who received less than 7.4 mL/kg/h, while the high-IVF group included 84 patients who received more than this rate. Fluid rate trend over time is shown in Fig. 2.

Total fluid rate including crystalloid and colloid over time
Demographic and preoperative characteristics are detailed in Table 1. The low-IVF group was slightly younger in age, more likely male, higher BMI, and less likely to be undergoing initial resection. In both groups, the most common primary site of pathology was the appendix, most common histology was adenocarcinoma, and most common peritoneal pathology was peritoneal mucinous carcinomatosis (PMCA).
Operative Data
Operative details including intake and output are reported in Table 2. The low-IVF group was more likely to have undergone laparoscopic-assisted HIPEC (13.3% vs. 0%, p < 0.001), more likely to have a CC score of 0 (91.6% vs. 64.3%, p < 0.001), and less likely to have undergone diaphragmatic stripping or splenectomy. Almost all patients received intraperitoneal mitomycin C (100% vs. 96.4%, p = 0.082).
The mean total intraoperative intake rate including crystalloid, colloid, and blood products was 5.3 ± 1.3 mL/kg/h in the low-IVF group and 11.1 ± 3.1 mL/kg/h in the high-IVF group (p < 0.001). The low-IVF group received less crystalloid and colloid, and was less likely to need red blood cell transfusion (0% vs. 14.3%, p < 0.001) or vasopressor drip (2.4% vs. 11.9%, p = 0.018). The low-IVF group had lower mean urine output (0.7 ± 0.4 vs. 1.1 ± 0.8 mL/kg/h, p < 0.001) and estimated blood loss (183 ± 148 vs. 330 ± 379 mL, p = 0.002).
Postoperative Outcomes
Univariate comparisons of the postoperative outcomes for the low-IVF and high-IVF groups are detailed in Table 3. Removal of NGT and timing of diet advancement was similar in the two groups. Foley catheter was removed earlier in the low-IVF group (6.2 vs. 8.0 days, p < 0.001).
The rate of 90-day complications of all grades was similar in the low-IVF and high-IVF groups (49.4% vs. 61.9%, p = 0.104). The rate of Clavien–Dindo grade 3–5 complications was lower in the low-IVF group (14.5% vs. 33.3%, p = 0.004). The low-IVF group had significantly fewer cardiac complications (myocardial infarction and new arrhythmia), less postoperative hypotension, fewer pneumonias, and fewer organ space surgical site infections. There were no statistically significant differences in acute renal failure, urinary tract infection, pleural effusion requiring intervention, anastomotic leak, ileus or small bowel obstruction, deep vein thrombosis, or pulmonary embolism.
There were nonsignificant trends favoring the low-IVF group in the rates of reoperation (6.0% vs. 11.9%, p = 0.184) and unplanned readmission (18.1% vs. 29.8%, p = 0.092) within 90 days of surgery. Hospital length of stay was shorter in the low-IVF group (9.6 vs. 12.1 days, p = 0.007).
Multivariable Models
Multivariate logistic regression models were created for 90-day readmission and 90-day major complications (Clavien–Dindo grade 3–5), and linear regression model was created for length of stay (Table 4).
Increased intraoperative fluid rate was significantly associated with increased length of stay (p = 0.029, estimate +1.52 days per 5 mL/kg/h increase in fluid rate, 95% CI 0.15–2.89), and association with unplanned readmission and major complications just missed significance (OR 1.86, p = 0.060, and OR 1.78, p = 0.072, respectively). Bowel resection was independently associated with increased risk of unplanned readmission and increased length of stay. The only independent predictor of major complication was higher estimated blood loss during surgery. Laparoscopic-assisted approach was associated with a shorter length of stay but higher rate of readmission.
Open Surgery Subgroup
Multivariable logistic regression and linear regression models were created for the same explanatory variables, including only the 156 patients who underwent open surgeries.
For 90-day unplanned readmission, only bowel resection was significantly associated (OR 5.53, 95% CI 2.05–14.92, p = 0.0007), while fluid rate had marginal significance (OR 1.82 per 5 mL/kg/h increase, CI 0.94–3.52, p = 0.075). For major complications, only EBL was significantly associated (OR 1.16 per 100 mL increase, CI 1.01–1.34, p = 0.034), while fluid rate was again marginal (OR 1.74, CI 0.93–3.25, p = 0.086). For length of stay, EBL (p = 0.016, estimate +0.37 days per 100 mL increase in EBL, CI 0.07–0.67) and fluid rate (p = 0.033, estimate +1.54 days in LOS per 5 mL/kg/h increase in fluid rate, CI 0.12–2.97) were significantly associated.
Discussion
Our current analysis of a large cohort of patients at an experienced CS/HIPEC center demonstrates that patients who received less IVF intraoperatively, at rates significantly lower than previously reported in similar patients, had fewer major complications, cardiac complications, pneumonias, and organ space surgical site infections. Lower IVF rate was independently associated with shorter length of stay in multivariable models.
Many risk factors for complications in CS/HIPEC are determined by disease biology and patient factors rather than clinical decisions. Patient age, sex, BMI, preoperative nutritional status, and medical comorbidities can be difficult or impossible to optimize. Extent of surgery can be altered by preoperative chemotherapy, but is often predetermined by cancer biology. Fluid administration is one of the few areas where active intent can be applied to change the complication profile of CS/HIPEC.
The overall outcomes reported in this study compare favorably with other high-volume centers. Outcomes at 90 days in this cohort showed one mortality (0.6%), 9.0% reoperation rate, and median length of stay of 9 days. By comparison, 30-day outcomes in a NSQIP analysis reported mortality rate of 1.1%, reoperation rate of 6.8% and median length of stay of 8 days,20 although these numbers likely underestimate the risk as that publication included patients who underwent cytoreduction with or without HIPEC.
Only a handful of studies have examined the impact of intraoperative IVF on outcomes in CS/HIPEC, and all have found increasing fluid rate to be a risk factor for complications. The only randomized trial examining this issue included 80 patients and compared goal-directed fluid therapy (GDFT) with standard care12. GDFT resulted in lower rates of major abdominal, cardiac, hepatic, and all complications, and shorter hospital length of stay (19 vs. 29 days, p < 0.0001). The mean total volume rate in the GDFT group was 8.54 mL/kg/h compared with 12.30 mL/kg/h in the control group (p < 0.0001). Notably, the fluid rate in the GDFT group in this randomized trial is higher than the median rate in our current study.
Comparison of our patients with other retrospective series from high-volume centers shows that our patients consistently received less fluid than restrictive or low-IVF groups from other centers. Given the favorable outcome demonstrated in this study, adopting an even more restrictive strategy than previously reported may represent an opportunity to further improve outcomes. In our patients, the mean total intraoperative fluid and product rate was 8.2 mL/kg/h, and blood transfusion was required in only 7.2%.
An analysis of 133 patients treated at the City of Hope National Medical Center showed a mean rate of 15.7 mL/kg/h and blood transfusion in 59.4%.15 Operative times and extent of organ resection were comparable at the two centers, but the key differences were blood loss (932 mL at City of Hope vs. 257 mL at Roswell) and perfusion with platinum-based agents (27.8% vs. 1.8%). Although chemotherapy agent was not significant on univariate analysis in either study, it may have impacted anesthetic management owing to anticipated nephrotoxicity associated with platinum-based agents. The rate of Clavien–Dindo grade 3–5 complications in the overall cohort was 31.6% at City of Hope, which is consistent with 33.3% in our high-IVF group, but substantially higher than 14.5% in our low-IVF group. On multivariate analysis, Eng et al. found that older age, higher fluid rate, and increased blood loss were associated with increased comprehensive complication index.
Another retrospective analysis of 169 patients from the University of Massachusetts examined outcomes after introduction of a restrictive intraoperative fluid protocol.21 Normalized fluid rates were not reported, but mean crystalloid received was 4.4 L in the restrictive group and 8.0 L in a historical group treated with a permissive strategy, with 89.9% receiving mitomycin C. The volume received by the restrictive protocol group in that study is slightly higher than the low-IVF group in our study (3.9 L). Multivariate logistic regression showed decreased risk of Clavien–Dindo grade 3–5 complications in the restrictive protocol arm. The addition of our current analysis to the results reported previously suggests that an ultra-restrictive fluid protocol in CS/HIPEC is safe and may be superior.
Additional evidence for detrimental effects of IVF comes from a multi-institutional study looking at risk factors for readmission amongst 2,017 HIPEC cases. The 30-day readmission rate was 15.9% overall, and the group of patients without readmission had lower total intraoperative IVF intake (6.5 vs. 7.2 L, p < 0.01).22
Our results show that intraoperative factors associated with high IVF use included diaphragmatic stripping and splenectomy, which may reflect the extent of disease. Since most patients had colorectal and appendiceal cancers, this finding likely represents patients with higher peritoneal cancer index (PCI) with disease extending to the upper abdomen.
There are multiple factors that may prompt an increasing IVF rate, such as length of surgery, extent of resection, and blood loss. In this study, these factors were accounted for to the best of our ability by multivariable and linear regression models. The duration of surgery was normalized by using the rate rather than volume of fluid received. The estimated blood loss and extent of surgery including gastrointestinal resections were included in the multivariate model, and other factors associated with differences in fluid administration were considered for the models. Baseline characteristics such as age, sex, and BMI were included in the regression models to compensate for unconscious decisions and to adjust for baseline differences between groups, but were not found to be significant predictors of complications. The high-IVF group was more likely to be undergoing primary resection, which may reflect greater disease burden as these patients would have been referred for CS/HIPEC prior to surgical exploration and may have had more extensive disease by imaging. Adjustments for these differences were made by use of regression models.
In the multivariate models, increased total intraoperative intake rate was independently associated with increased hospital length of stay, with near significance for association with 90-day readmission rate and major complications. The finding of higher readmission rate in the laparoscopic group was likely due to a small sample size of 11 patients, and two patients with planned readmission for second-look laparoscopy for repeat HIPEC in the neoadjuvant setting. Subgroup analysis in the open surgery group demonstrated similar risk factors to be independently associated with the three outcomes of interest.
Several limitations to our study should be noted. PCI scores were missing for the majority of patients and, therefore, were not included in the analysis; however, CC scores and extent of resections were included as surrogates for extent of disease. Data regarding FloTrac parameters and fluid adjustments were not captured and were unable to be correlated with the results of this study. Additionally, this series represents a single institution experience at an established program, and the outcomes reflect institutional anesthesia and surgery practices. The outcomes of restrictive fluid administration during the learning curve or at other institutions may be different. There are limitations to retrospective analysis in the absence of a strictly defined fluid protocol, and although potential confounders were explored and significant variables were adjusted for, it is possible that there is a factor that was not accounted for in the regression models. Postoperative care may also have had an impact on outcomes, although all patients were managed similarly according to institutional practice. Lastly, due to the heterogeneity of the patient population, survival analyses were not feasible.
Our experience demonstrates that a restrictive fluid rate, even lower than previously reported, is safe and may be superior to liberal fluid administration. Since we primarily used mitomycin C, the safety of this approach for patients who receive platinum-based chemotherapy is not clear. The relative rarity of CS/HIPEC procedures, and heterogeneity of surgery for each patient, makes it challenging to provide optimized care, but restrictive or goal-directed fluid management intraoperatively has been consistently shown to be beneficial.
Conclusion
The historical paradigm of liberal fluid administration during CS/HIPEC may be unnecessary and is potentially harmful. The outcomes in this study show that restrictive fluid use is associated with a reduction in length of stay and major postoperative complications.
References
Cao C, Yan TD, Black D, et al. A systematic review and meta-analysis of cytoreductive surgery with perioperative intraperitoneal chemotherapy for peritoneal carcinomatosis of colorectal origin. Ann Surg Oncol. 2009;16:2152–65.
Miner TJ, Shia J, Jaques DP, et al. Long-term survival following treatment of pseudomyxoma peritonei: an analysis of surgical therapy. Ann Surg. 2005;241:300–8.
Yan TD, Deraco M, Baratti D, et al. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for malignant peritoneal mesothelioma: multi-institutional experience. J Clin Oncol. 2009;27:6237–42.
Spiliotis J, Halkia E, Lianos E, et al. Cytoreductive surgery and HIPEC in recurrent epithelial ovarian cancer: a prospective randomized phase III study. Ann Surg Oncol. 2015;22:1570–5.
Seshadri RA, Glehen O. Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy in gastric cancer. World J Gastroenterol. 2016;22:1114–30.
Haslinger M, Francescutti V, Attwood K, et al. A contemporary analysis of morbidity and outcomes in cytoreduction/hyperthermic intraperitoneal chemoperfusion. Cancer Med. 2013;2:334–42.
Jafari MD, Halabi WJ, Stamos MJ, et al. Surgical outcomes of hyperthermic intraperitoneal chemotherapy: analysis of the American College of Surgeons National Surgical Quality Improvement Program. JAMA Surg. 2014;149:170–5.
Raspé C, Flöther L, Schneider R, et al. Best practice for perioperative management of patients with cytoreductive surgery and HIPEC. Eur J Surg Oncol. 2017;43:1013–27.
Esteve-Pérez N, Ferrer-Robles A, Gómez-Romero G, et al. Goal-directed therapy in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy: a prospective observational study. Clin Transl Oncol. 2019;21:451–8.
Schluerman CN, Hoeppner J, Benk C, et al. Intra-abdominal pressure, cardiac index and vascular resistance during hyperthermic intraperitoneal chemotherapy: a prospective observational study. Minerva Anestesiol. 2016;82:160–9.
Coccolini F, Corbella D, Finazzi P, et al. Time course of cytokines, hemodynamic and metabolic parameters during hyperthermic intraperitoneal chemotherapy. Minerva Anestesiol. 2016;82:310–9.
Colantonio L, Claroni C, Fabrizi L, et al. A randomized trial of goal directed vs. standard fluid therapy in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. J Gastrointest Surg. 2015;19:722–9.
Dupont S, Schiffer ERC, White MJ, et al. Changes in hepatic blood flow and liver function during closed abdominal hyperthermic intraperitoneal chemotherapy following cytoreduction surgery. Gastroenterol Res Pract. 2018;2018:8063097.
Maciver AH, Al-Sukhni E, Esquivel J, et al. Current delivery of hyperthermic intraperitoneal chemotherapy with cytoreductive surgery (CS/HIPEC) and perioperative practices: an international survey of high-volume surgeons. Ann Surg Oncol. 2017;24:923–30.
Eng OS, Dumitra S, O’Leary M, et al. Association of fluid administration with morbidity in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. JAMA Surg. 2017;152:1156–60.
Som A, Maitra S, Bhattacharjee S, et al. Goal directed fluid therapy decreases postoperative morbidity but not mortality in major non-cardiac surgery: a meta-analysis and trial sequential analysis of randomized controlled trials. J Anesth. 2017;31:66–81.
Wrzosek A, Jakowicka-Wordliczek J, Zajaczkowska R, et al. Perioperative restrictive versus goal-directed fluid therapy for adults undergoing major non-cardiac surgery. Cochrane Database Syst Rev. 2019;12:CD012767.
Oken MM, Creech RH, Tormey DC, et al. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am J Clin Oncol. 1982;5:649–55.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Foster JM, Sleightholm R, Patel A, et al. Morbidity and mortality rates following cytoreductive surgery combined with hyperthermic intraperitoneal chemotherapy compared with other high-risk surgical oncology procedures. JAMA Netw Open. 2019;2:e186847.
Hendrix RJ, Damle A, Williams C, et al. Restrictive intraoperative fluid therapy is associated with decreased morbidity and length of stay following hyperthermic intraperitoneal chemoperfusion. Ann Surg Oncol. 2019;26:490–6.
Lee TC, Wima K, Sussman JJ, et al. Readmissions after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy: a US HIPEC collaborative study. J Gastrointest Surg. 2020;24:165–76.
Acknowledgments
None.
Funding
This work was supported by National Cancer Institute (NCI) Grant P30 CA016056.
Author information
Authors and Affiliations
Contributions
J.S.P., K.W., K.A., and V.A.F. had access to all data in this study and take full responsibility for the integrity of the data and accuracy of the analysis. Study concept and design: all authors. Acquisition of data: J.S.P., J.L. Analysis and interpretation of the data: J.S.P., K.W., K.A., V.A.F. Drafting and manuscript: J.S.P., V.A.F. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: K.W., K.A.
Corresponding author
Ethics declarations
Disclosure
V.F., Consultant for Novartis. No other disclosures were reported.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Peng, J.S., LaPiano, J., Wang, K. et al. Restrictive Intraoperative Fluid Rate is Associated with Improved Outcomes in Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy. Ann Surg Oncol 29, 163–173 (2022). https://doi.org/10.1245/s10434-021-10556-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-021-10556-3