
Abstract
Background
Parkinson’s disease (PD) is the most common movement disorder and the second most common neurodegenerative disease. The aim of our study was to compare gray–white matter changes (GWC) between Parkinson's disease (PD) patients and age-matched healthy control group as well as comparing GWC between different stages of PD (early and complicated). Our study was prospective cross-sectional case–control observational study with analytic component conducted on twenty patients and ten controls without any signs or symptoms of PD or any history of PD in first-degree relatives. All patients and controls were tested for history taking with stress on resting tremors, rigidity, gait abnormalities, postural instability and any symptoms of cognitive impairment, clinical examination including general examination and neurological examination. Also diffusion tensor imaging (DTI) with fiber tracking (tractography) and susceptibility-weighted MR imaging were performed for all cases.
Results
As regards DTI and evaluation of fractional anisotropy (FA) and mean diffusivity (MD) values between PD cases and healthy controls, the cases group showed significant decrease in FA values at substantia nigra on both sides and left cingulum as well as significant increase in MD values at substantia nigra on both sides and corpus callosum. Also, there are significant decrease in FA values at substantia nigra on both sides and significant increase in MD values at substantia nigra on both sides and right cingulum in late parkinsonism when compared to early parkinsonism. A cutoff FA value of 0.945 at right substantia nigra and cutoff FA value of 0.585 at left substantia nigra showed significant AUC that could differentiate between cases and controls. Also cutoff MD value of 0.791 at right substantia nigra and cutoff MD value of 0.813 at left substantia nigra showed significant AUC that could differentiate between cases and controls.
Conclusions
Diffusion tensor imaging showed valuable role in evaluation of gray–white matter changes in Parkinson's disease. Also, it helps to assess degree of gray–white matter changes when comparing late parkinsonism to early parkinsonism through evaluation of FA and MD values at corpus callosum, substania nigra, and cingulum.
Similar content being viewed by others

Background
Parkinson's disease (PD) stands as the most prevalent movement disorder and the second most prevalent neurodegenerative disease. Parkinson's disease is diagnosed clinically based on the presence of motor symptoms including bradykinesia, rest tremor, rigidity, and postural instability. It is characterized by dysfunction in the body, while Parkinson's disease is primarily recognized for its motor symptoms. It is important to acknowledge the substantial influence of non-motor symptoms on a patient's overall quality of life. Cognitive impairments, for instance, are frequently observed in individuals with PD and may even manifest early on, although they tend to be more prevalent in the advanced stages of the disease [1, 2].
The course of Parkinson's disease, while unrelenting, exhibits significant variability and unpredictability. The deterioration observed in clinical symptoms is a manifestation of the continuous degeneration of the nigrostriatal system, yet its progression remains elusive and inconsistent. It remains uncertain whether the symptoms of Parkinson's disease are a result of age-related neuronal loss combined with a temporary neurodegenerative injury or an ongoing neurodegenerative process. Studies examining the progression of PD through pathological analysis have been restricted in their scope. The focus of clinical studies on the progression of Parkinson's disease (PD) has primarily been on patients in the early stages of the illness, while neglecting those with severe and long-lasting conditions. These studies have predominantly relied on cross-sectional data and utilized the Unified PD Ratings Scale (UPDRS) or similar clinical measures to track the advancement of the disease [3, 4].
The challenge in clinical studies lies in examining functional status while also considering the impact of anti-Parkinson drugs on symptoms, which can complicate the ability to attribute clinical changes solely to disease progression. This creates a difficulty in isolating the true effects of the disease on patients.
The assessment of white matter using DTI is a valuable tool that plays a critical role in the early diagnosis of Parkinson's disease, potentially having a significant impact on the quality of life for patients. The assessment of patients over time and the evaluation of disease progression and treatment response can be facilitated by examining abnormalities in white matter. It is worth noting that these markers can also provide interesting insights. The presence of iron differs across various regions affected by neurodegenerative diseases. Iron could potentially have a significant impact on the neuropathology associated with these diseases [5].
Hence, the concentration and distribution of iron in deep brain nuclei could serve as potential biomarkers in Parkinson's disease. Iron has the ability to alter the magnetic properties of tissues in which it accumulates. Susceptibility-weighted imaging (SWI), a new MRI technique, is capable of detecting the magnetic susceptibility of tissues, allowing for the identification of iron-related information in neurodegenerative parkinsonism. This makes SWI a promising tool for detecting Parkinson's disease [6].
The blurring between the boundaries of gray and white matter, known as gray–white matter contrast (GWC), is measured using T1-weighted MRI images. While the exact neurobiological reasons for this measure are not fully understood, some studies have suggested that GWC could indicate local differences in tissue integrity and myelin degradation. This could be due to increased water content in the white matter or iron deposition. Changes in GWC have been linked to aging, with a decrease in contrast observed mainly in the frontal and temporoparietal regions. GWC appears to be particularly associated with age-related variations in myelin content at the boundary between gray and white matter in lightly myelinated areas [7].
The authors suggested that GWC could potentially serve as a valuable method for monitoring myelin deterioration in important brain regions among patients in clinical settings. As a result, GWC could serve as an indirect indicator of alterations in the brain's histological characteristics that could greatly influence neurodegenerative processes. In individuals with Parkinson's disease (PD), MRI has shown cortical atrophy primarily through voxel-based morphometry and cortical thickness measurements, as well as changes in white matter using diffusion tensor imaging [8].
The aim of our study was comparison of GWC between PD and age-matched healthy controlled group as well as comparison of GWC between different stages of PD (early and complicated).
Methods
Our study included individuals with Parkinson's disease who were 30 years of age or older and exhibited at least two of the following symptoms: resting tremor, bradykinesia, rigidity, and postural instability (with one of the symptoms being resting tremor or bradykinesia). These individuals were examined on the same day as the MRI or within 1 week of the MRI, and had no history of surgical treatment or deep brain stimulation. Patients with claustrophobia or MRI artifacts were not included in our study.
All participants, both patients and healthy controls (senile with no clinical signs of parkinsonism), underwent a standardized protocol conducted by a single neurologist. This protocol included a thorough history taking focusing on resting tremors, rigidity, gait abnormalities, postural instability, and any signs of cognitive impairment. A clinical examination, which encompassed a general assessment and a neurological examination using the Unified Parkinson's disease rating scale [9] and Modified Hoehn and Yahr Scale [10], was also performed. Patients who were taking anti-Parkinson medications were assessed after being off the medication for 12 h to ensure they were in a “defined off” state.
Early Parkinson's disease (PD) is characterized by patients who receive a diagnosis of PD within 4.5 years of the disease's onset. On the other hand, complicated PD refers to patients who experience the typical motor symptoms of PD in addition to other motor or non-motor complications. These complications can be either related to the disease itself (such as freezing) or to the treatment (such as dyskinesias or hallucinations) [11, 12].
The disease severity was evaluated through MR imaging, which included non-contrast conventional sequences such as T1-weighted, T2-weighted, and FLAIR sequences in axial, sagittal, and coronal planes. Additionally, diffusion tensor imaging (DTI) with fiber tracking (tractography) and susceptibility-weighted imaging were performed. The MR imaging system used was the Intera Achieva by Philips-Netherlands, operating at 1.5 Tesla with an 8-channel head coil.
The diffusion tensor imaging (DTI) protocol consisted of axial plane imaging with 3D T2 (TR: 4700, TE: 85) and 3D PD (TR: 3400, TE: 13), slice thickness of 2 mm, spacing of 0, matrix size of 256 × 256, FOV of 24 cm, and NEX of 2. DTI was performed with 12 directions (TR: 8000, TE: min), slice thickness of 5 mm, spacing of 1, matrix size of 128 × 128, and FOV of 26 cm.
Post-processing of DTI involved measuring FA and MD at substantia nigra, corpus callosum, and cingulum in both case and control groups. Two experienced neuro-radiologists of 10 and 25 years’ experience at the way of conjoint reading performed manual region of interest (ROI) analysis and tractography. ROI analysis allowed for the measurement of FA and MD at specific locations on MRI slices.
Two methods of determining regional FA and MD in specific tracts were manual region of interest (ROI) analysis and tractography. Region of interest analysis enables the measurement of FA and MD at predefined locations on particular slices of a magnetic resonance image.
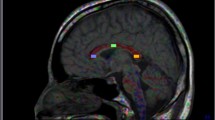
Regions of interest (ROIs) were manually positioned over the substantia nigra, corpus callosum tractography, and cingulum tractography. The cingulum was split into two regions on both sides. Fiber tracts had to pass through the furthest points of each segment and a point in the middle. The left and right tracts were examined individually, and the values were averaged across the specified area of interest. For the substantia nigra, the left and right tracts were also analyzed separately, and the values were averaged over the defined area of interest (Figs. 1, 2, 3, 4).

A 60-year-old senile female. A DTT of corpus callosum revealed FA value = 0.492 and MD value = 0.967. B DTT of cingulum revealed FA value = 0.468 and MD value = 0.831 at right side, FA value = 0.438 and MD value = 0.838 at left side C DTT of SN revealed FA value = 0.917and MD value = 0.429 at right side, FA value = 0.529 and MD value = 0.867 at left side

A 64-year-old senile male patient with late parkinsonian disease complained of resting tremors and dyskinesia. A Sagittal T2-colored image with DTT of corpus callosum revealed: thinning of anterior part of body of corpus with lost cortical fibers at genu, body, and splenium (FA = 0.381, MD = 0.995). B DTT of cingulum revealed: mild thinning of both tracts (right cingulum FA = 0.316, MD = 0.843 and Left cingulum FA = 0.308, MD = 0.878). C SWI of substantia nigra revealed: mild thinning of SN on both sides with irregular borders and lost swallow tail sign. D Axial T2 DTI of SN revealed: reduced FA value on both sides (right SN FA = 0.2, MD = 0.858 and left SN FA = 0.123, MD = 1.120)

A 68-year-old senile female patient with late parkinsonian disease complained of bradykinesia and rigidity. A Sagittal T2-colored image with DTT of corpus callosum revealed: lost cortical fibers of corpus callosum, more evident at body (FA = 0.349, MD = 1.079). B DTT of cingulum revealed: thinning of right tract and mild thinning at left tract (right cingulum FA = 0.308, MD = 0.838 and Left cingulum FA = 0.312, MD = 0.861). C Axial T2 DTI of SN revealed: reduced FA value on both sides (right SN FA = 0.485, MD = 0.989, and left SN FA = 0.455, MD = 1.130)

A 54-year-old male patient with early parkinsonian disease complained of resting tremors. A Sagittal T2-colored image with DTT of corpus callosum revealed: thinning of corpus callosum, more evident at body with lost cortical fibers (FA = 0.458, MD = 0.987). B DTT of cingulum revealed: thinning of both tracts, more evident at left side (right cingulum FA = 0.363, MD = 0.778, and left cingulum FA = 0.305, MD = 0.774). C DTT of SN revealed: mild reduced FA value on both sides (right SN FA = 0.510, MD = 1.038, and left SN FA = 0.502, MD = 0.901)
Statistical analysis
Data analysis was conducted using SPSS software, version 25 (SPSS Inc., PASW statistics for windows version 25. Chicago: SPSS Inc.). Qualitative data were presented using number and percentage. Quantitative data were described using median (minimum and maximum) for non-normally distributed data and mean ± standard deviation for normally distributed data after checking for normality using the Kolmogorov–Smirnov test. The significance of the results was considered at the level of ≤ 0.05. Chi-square, Fischer exact test, and Monte Carlo tests were utilized to compare qualitative data between groups as appropriate. Kruskal–Wallis and Mann–Whitney U tests were used to compare between two studied groups and more than two studied groups, respectively, for non-normally distributed data. Wilcoxon signed-rank test and Friedman test were employed to compare between more than two studied periods. Student t-test was used to compare two independent groups for normally distributed data. Spearman's rank-order correlation was used to determine the strength and direction of a linear relationship between two non-normally distributed continuous variables and/or ordinal variables. Receiver operating characteristics curve (ROC curve) was utilized to calculate the validity (sensitivity and specificity) of continuous variables with the calculation of the best cut off point. Predictive values and accuracy were assessed using cross-tabulation.
Results
The current research involved 20 patients diagnosed with PD and 10 healthy individuals who were matched with the patient group in terms of age and sex.
The cases group showed significant decrease in right substantia nigra FA, left substantia nigra FA, left cingulate FA and significant increase in right substantia nigra MD, left substantia nigra MD and corpus callosum MD. No significant difference was found between studied cases regarding right cingulate FA, right cingulate MD, left cingulate MD and corpus callosum FA (Table 1).
There were significant decrease in right substantia nigra FA, left substantia nigra FA and significant increase in right substantia nigra MD, left substantia nigra MD and right cingulate MD in late parkinsonism when compared to early parkinsonism. However, no significant difference was found regarding left cingulate FA and MD as well as corpus callosum FA and MD between two groups (Table 2).
Receiver operating characteristic (ROC) curve was conducted to assess validity of corpus callosum MD and left cingulate FA in differentiating between cases and control groups. Only corpus callosum MD at cutoff value of 0.926 showed significant AUC that could differentiate between cases and controls with sensitivity 95% and specificity 80% (Table 3). Also, ROC curve was conducted to assess validity of right cingulate FA in differentiating between early and late stage of Parkinson. Right cingulate MD had nonsignificant AUC (Table 4).
MUPRDS showed significant positive correlation with left cingulate MD and left substantia nigra MD among cases group. Also, it showed significant negative correlation with right and left substantia nigra FA among cases group. However, no significant correlation was found between MUPRDS and other parameters (Table 5).
Disease duration showed significant positive correlation with right and left substantia nigra MD among cases group. Also, it showed significant negative correlation with right and left substantia nigra FA among cases group. However, no significant correlation was found between disease duration and other parameters (Table 6).
Receiver operating characteristic (ROC) curve was conducted to assess validity of right and left substantia nigra FA in differentiating between cases and controls. At cutoff value of 0.945, the right substantia nigra FA showed significant AUC that could differentiate between cases and controls sensitivity 90% and specificity 80%. Also, at cutoff value of 0.585, the left substantia nigra FA showed significant AUC that could differentiate between cases and controls with sensitivity 95% and specificity 90%. ROC curve was conducted to assess validity of right substantia nigra MD and left substantia nigra MD in differentiating between cases and controls. At cutoff value of 0.791, the right substantia nigra MD showed significant AUC that could differentiate between cases and controls sensitivity 80% and specificity 90%. Also, at cutoff value of 0.813, the left substantia nigra MD showed significant AUC that could differentiate between cases and controls with sensitivity 80% and specificity 70% (Table 7).
As regards SWI, about 20% of cases of parkinsonism revealed morphological changes at substantia nigra in the form mild thinning, irregular margins, and lost swallow tail sign.
Discussion
Parkinson's disease (PD) is a progressive and chronic degenerative neurological disorder. It is characterized by the degeneration of dopamine neurons in the substantia nigra (SN) along with the loss of their axons that connect to the striatum through the nigrostriatal pathway. This results in a deficiency of the neurotransmitter dopamine, leading to the primary motor symptoms of PD [13].
In early stages of PD, structural brain imaging using conventional MRI (cMRI) with visual assessment of T2- and T1-weighted sequences typically appears normal. Therefore, its main purpose is to identify or rule out other underlying conditions that may be causing parkinsonism [14].
Diffusion tensor imaging (DTI) is a non-invasive neuroimaging technique based on MRI that can analyze the diffusivity of brain tissues based on motion of water molecules, particularly along axons. Fractional anisotropy (FA) measures diffusivity in different directions and provides insight into the microstructural organization of the brain's tensors. Mean diffusivity (MD) indicates the overall movement of water molecules in the brain. DTI is commonly used to identify changes in white matter, but it can also detect abnormalities in gray matter. It may be able to detect these changes earlier than traditional MRI methods. Studies using DTI have shown changes in diffusivity in subcortical structures and decreased FA in the substantia nigra in individuals with Parkinson's disease [15, 16].
The aim of the present study was to compare GWC between PD and age-matched healthy control group and also compare GWC between different stages of PD (early and complicated).
The present study was cross-sectional case–control observational study with analytic component. Data were obtained prospectively from twenty patients and ten controls presented to the outpatient clinic of the neurology department at our institution. All patients and control were matched in age, sex, residence, risk factors, and disease duration; thus, no other factors can affect scope of our results.
The present study showed that the mean age of the cases and controls was 60.40 ± 11.09, most of them were males (75%).
In line with our research, the average age at previous study of both cases and controls was around 63.7 years. There was an equal distribution of gender in both groups, with 59.5% males and 40.5% females [17].
Parkinson’s disease is characterized by a clinical syndrome known as parkinsonism from the motor standpoint. This syndrome universally includes four cardinal features: bradykinesia, rest tremor, rigidity, and postural and gait impairment [18].
The current research demonstrated a notable distinction between the subjects and controls in terms of Hoehn and Yahr and MDS-UPDRS. Consistent with our results, Uribe et al. [19] found no significant variations between the groups in terms of age, gender, or education. Patients with Parkinson's disease scored notably lower than healthy individuals in cognition and memory. Mild cognitive impairment was present in 44% of the patients, with 8% of the PD sample exhibiting deficits in the language domain.
Schrag et al. [20] demonstrated that tremor was the predominant symptom of PD, with 41% of patients reporting it to their GP, compared to less than 1% of controls. Constipation was experienced by 37% of PD patients versus 23% of controls, depression by 18% versus 10%, fatigue by 15% versus 8%, dizziness by 14% versus 9%, anxiety by 12% versus 7%, and shoulder stiffness or pain by 12% versus 9%.
Previous research has also indicated that bradykinesia, rest tremor, rigidity, and loss of postural reflexes are the motor symptoms most frequently associated with Parkinson's disease. However, as the disease progresses, other clinical features may also become apparent, including bulbar dysfunction, neuro-ophthalmological abnormalities, and respiratory disturbances [21].
In terms of fractional anisotropy (FA) and mean diffusivity (MD) values among the groups under study, Hope et al. [22] stated that elevated MD levels are typically attributed to an increase in extracellular space, the impact of atrophy, demyelination, or loss of structural organization. Their research findings suggested a rise in MD levels in regions associated with Parkinson's disease pathology.
Our current study revealed that MDS-UPRDS showed significant positive correlation with left cingulate MD and left substantia nigra MD among cases group. Also, it showed significant negative correlation with right substantia nigra FA and left substantia nigra FA among cases group. However, no significant correlation was found between MDS-UPRDS and other parameters.
In line with our findings, previous studies observed that high MD of the SN [23], contralateral Put [24], GP [25, 26], Genu corrected with motor dysfunction. Low FA of the SN (7–12), NST [27], thalamic tract (anterior nucleus) [28] correlated with motor dysfunction (UPDRS-III).
Several studies, including those using PPMI data, have found strong correlations between reduced FA in the substantia nigra and the worsening of motor symptoms, as measured by the motor exams (part-III -UPDRS) [29,30,31,32,33].
Youn et al. [34] demonstrated that Parkinson's disease patients experiencing freezing of gait exhibited elevated MD values in subcortical regions like the basal ganglia in comparison to those without gait freezing.
In line with our findings, a study conducted by Zhan et al. [35] examined 12 patients with Parkinson's disease and 20 healthy individuals using the DTI technique. The study revealed that the FA values in the right and left substantia nigra, right and left internal capsule, and left putamen were lower in Parkinson's disease patients compared to the control group, which aligns with our findings. Additionally, their study found that the MD values in the substantia nigra and putamen were higher in Parkinson's disease patients than in the healthy control group.
In a study conducted by Schwarz et al. [36], it was discovered that the mean diffusivity (MD) in the substantia nigra (SN) region was elevated in patients with Parkinson's disease compared to the control group.
Kamagata et al. [37] showed that FA was significantly lower in patients with PD than in healthy controls in the anterior cingulate fiber tract. There were no significant mean diffusivity differences among the groups.
Contrarily, Vogt [38] showed that diffusion tensor imaging shows reduced fractional anisotropy throughout the entire cingulum bundle in parkinsonian disease.
It has been shown that the deterioration of the corpus callosum genu is linked to PD dementia [39], as well as executive and attention dysfunctions [40]. DTI of the corpus callosum (in the body and the splenium) can help differentiating PD patients according to their cognitive status (normal, mild cognitive impairment, or dementia).
Receiver operating characteristic (ROC) curve was conducted to assess validity of corpus callosum MD and left cingulate FA in differentiating between cases and control groups. Only corpus callosum MD at cutoff value of 0.926 showed significant AUC that could differentiate between cases and controls.
Wiltshire et al. [41] have also found that using DTI to examine the corpus callosum, specifically in the body and splenium, can assist in distinguishing between PD patients based on their cognitive abilities (normal, mild cognitive impairment, or dementia). In this regard, MD was shown to be more precise than FA.
Moreover, we found that with increased disease duration, there is significant positive correlation with right and left substantia nigra MD and Rt cingulate MD in late parkinsonism when compared to early parkinsonism. Also, it showed significant negative correlation with right and left substantia nigra FA among cases group. However, no significant correlation was found between disease duration and other parameters.
Based on our research, a recent longitudinal study using DTI found an increased rate of abnormalities in the substantia nigra (SN) of patients with Parkinson's disease (PD) over a 19.3-month period. Ofori and colleagues [42] also observed significant increases in free water (FW) in the posterior SN after 1 year of follow-up in PD patients. This increase in FW was further confirmed using data from the Parkinson's Progression Markers Initiative (PPMI) study, which showed consistent FW increases in PD patients over the course of 4 years compared to no changes in the control group.
Contrarily, some studies have found the opposite that the FA of SN is not a diagnostic biomarker of PD [43].
In our study, ROC curve was conducted to assess validity of right and left substantia nigra FA in differentiating between cases and controls. At cutoff value of 0.945, the right substantia nigra FA showed significant AUC that could differentiate between cases and controls sensitivity 90% and specificity 80%. At cutoff value of 0.585, the left substantia nigra FA showed significant AUC that could differentiate between cases and controls with sensitivity 95% and specificity 90%. As long as showing that at cutoff value of 0.791, the right substantia nigra MD showed significant AUC that could differentiate between cases and controls sensitivity 80% and specificity 90%. At cutoff value of 0.813, the left substantia nigra MD showed significant AUC that could differentiate between cases and controls with sensitivity 80% and specificity 70%. Measures of diffusivity were less frequently reported, and often no significant overall differences were detected.
In the same way, Huang and colleagues [44] examined FA in diagnosing PD and found that the results indicate a low diagnostic accuracy with an area under the curve of 0.516 (P = 0.880). The cutoff value is 0.311, with a sensitivity of 56.3% and specificity of 62.5%.
Vaillancourt et al. [45] also demonstrated that by utilizing high-resolution DTI, they were able to identify greater reductions in FA in the caudal regions of the substantia nigra (SN) compared to the middle or rostral regions. This distinction allowed for the differentiation between individuals with Parkinson's disease (PD) and controls with 100% sensitivity and specificity.
Limitations
Limitations of study included small sample size. Also, some cases of parkinsonism were unable to complete MRI examination.
Conclusions
Diffusion tensor imaging showed valuable role in evaluation of gray–white matter changes in Parkinson's disease. Also, it helps to assess degree of gray–white matter changes when comparing late parkinsonism to early parkinsonism through evaluation of FA and MD values at corpus callosum, substania nigra, and cingulum. PD patients showed significant decrease in right and left substantia nigra FA and left cingulate FA as well as significant increase in right and left substantia nigra MD and corpus callosum MD. Also, there are significant decrease in right and left substantia nigra FA and significant increase in right and left substantia nigra MD and right cingulate MD in late parkinsonism when compared to early parkinsonism. SWI had also additional role in evaluation of morphological changes of SN in Parkinson's disease.
Availability of data and materials
Available on request with the corresponding author.
Abbreviations
- PD:
-
Parkinson’s disease
- MRI:
-
Magnetic resonance imaging
- GWC:
-
Gray–white matter contrast
- DTI:
-
Diffusion tensor imaging
- FA:
-
Fractional anisotropy
- MD:
-
Mean diffusivity
- FLAIR:
-
Fluid attenuation inversion recovery
- 3D:
-
Three-dimensional
- MDS-UPDRS:
-
Movement Disorder Society-sponsored Unified Parkinson’s Disease Rating Scale
- SWI:
-
Susceptibility-weighted imaging
- ROI:
-
Region of interest
- ROC:
-
Receiver operating characteristic curve
- AUC:
-
Area under the curve
- SN:
-
Substantia nigra
- cMRI:
-
Conventional MRI
- HC:
-
Healthy control
- Put:
-
Putamen
- GP:
-
Globus pallidus
- NST:
-
Nigro-striatal tract
- PPMI:
-
Parkinson's progression markers initiative
- FW:
-
Free water
References
Rocca WA, Bower JH, Ahlskog JE, Elbaz A, Grossardt BR, McDonnell SK, Schaid DJ, Maraganore DM (2007) Risk of cognitive impairment or dementia in relatives of patients with Parkinson disease. Arch Neurol 64(10):1458–1464
Leverenz JB, Quinn JF, Zabetian C, Zhang J, Montine KS, Montine TJ (2009) Cognitive impairment and dementia in patients with Parkinson disease. Curr Top Med Chem 9(10):903–912
Rajput AH, Voll A, Rajput ML, Robinson CA, Rajput A (2009) Course in Parkinson disease subtypes: a 39-year clinicopathologic study. Neurology 73(3):206–212
Rascol O, Brooks DJ, Korczyn AD, De Deyn PP, Clarke CE, Lang AE (2000) A five-year study of the incidence of dyskinesia in patients with early Parkinson’s disease who were treated with ropinirole or levodopa. N Engl J Med 342(20):1484–1491
Ward RJ, Zucca FA, Duyn JH, Crichton RR, Zecca L (2014) The role of iron in brain ageing and neurodegenerative disorders. Lancet Neurol 13(10):1045–1060
Boelmans K, Holst B, Hackius M, Finsterbusch J, Gerloff C, Fiehler J, Münchau A (2012) Brain iron deposition fingerprints in Parkinson’s disease and progressive supranuclear palsy. Mov Disord 27(3):421–427
Uribe C, Segura B, Baggio HC, Abos A, Garcia-Diaz AI, Campabadal A, Marti MJ, Valldeoriola F, Compta Y, Bargallo N (2018) Gray/white matter contrast in Parkinson’s disease. Front Aging Neurosci 10:89
Thomas B, Somasundaram S, Thamburaj K, Kesavadas C, Gupta AK, Bodhey NK, Kapilamoorthy TR (2008) Clinical applications of susceptibility weighted MR imaging of the brain: a pictorial review. Neuroradiology 50:105–116
Martinez-Martin P, Rodriguez-Blazquez C, Alvarez-Sanchez M (2013) Expanded and independent validation of the Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS). J Neurol 260:228–236
Zhao YJ, Wee HL, Chan YH, Seah SH, Au WL, Lau PN, Pica EC, Li SC, Luo N, Tan LC (2010) Progression of Parkinson’s disease as evaluated by Hoehn and Yahr stage transition times. Mov Disord 25(6):710–716
Oertel W, Berardelli A, Bloem B, Bonuccelli U, Burn D, Deuschl G, Dietrichs E, Fabbrini G, Ferreira J, Friedman A (2011) Early (uncomplicated) Parkinson’s disease. Eur Handb Neurol Manag 1:217–236
Oertel W, Berardelli A, Bloem B, Bonuccelli U, Burn D, Deuschl G, Dietrichs E, Fabbrini G, Ferreira J, Friedman A (2011) Late (complicated) Parkinson’s disease. Eur Handb Neurol Manag 1:237–267
Nyatega CO, Qiang L, Adamu MJ, Kawuwa HB (2022) Gray matter, white matter and cerebrospinal fluid abnormalities in Parkinson’s disease: a voxel-based morphometry study. Front Psych 13:1027907
Heim B, Krismer F, De Marzi R, Seppi K (2017) Magnetic resonance imaging for the diagnosis of Parkinson’s disease. J Neural Transm (Vienna) 124(8):915–964
Deng X-Y, Wang L, Yang T-T, Li R, Yu G (2018) A meta-analysis of diffusion tensor imaging of substantia nigra in patients with Parkinson’s disease. Sci Rep 8(1):2941
Hall JM, Ehgoetz Martens KA, Walton CC, O’Callaghan C, Keller PE, Lewis SJ, Moustafa AA (2016) Diffusion alterations associated with Parkinson’s disease symptomatology: a review of the literature. Parkinsonism Relat Disord 33:12–26
Ng YF, Ng E, Lim EW, Prakash KM, Tan LCS, Tan EK (2021) Case-control study of hypertension and Parkinson’s disease. NPJ Parkinsons Dis 7(1):63
Etienne G, Hung N, Sarah B, Pierre B, Erwan B, Claude V, Mélanie L, Christian D (2018) Cardinal motor features of parkinson’s disease coexist with peak-dose choreic-type drug-induced dyskinesia. J Parkinsons Dis 8(2):323–331
Uribe C, Segura B, Baggio HC, Abos A, Garcia-Diaz AI, Campabadal A, Marti MJ, Valldeoriola F, Compta Y, Bargallo N, Junque C (2018) Gray/white matter contrast in Parkinson’s disease. Front Aging Neurosci 10:89
Schrag A, Anastasiou Z, Ambler G, Noyce A, Walters K (2019) Predicting diagnosis of Parkinson’s disease: a risk algorithm based on primary care presentations. Mov Disord 34(4):480–486
Váradi C (2020) Clinical features of Parkinson’s disease: the evolution of critical symptoms. Biology (Basel) 9(5):103
Hope TR, Selnes P, Rektorová I, Anderkova L, Nemcova-Elfmarkova N, Balážová Z, Dale A, Bjørnerud A, Fladby T (2019) Diffusion tensor and restriction spectrum imaging reflect different aspects of neurodegeneration in Parkinson’s disease. PLoS ONE 14(5):e0217922
Scherfler C, Esterhammer R, Nocker M, Mahlknecht P, Stockner H, Warwitz B, Spielberger S, Pinter B, Donnemiller E, Decristoforo C, Virgolini I, Schocke M, Poewe W, Seppi K (2013) Correlation of dopaminergic terminal dysfunction and microstructural abnormalities of the basal ganglia and the olfactory tract in Parkinson’s disease. Brain 136(10):3028–3037
Wang J, Yang QX, Sun X, Vesek J, Mosher Z, Vasavada M, Chu J, Kanekar S, Shivkumar V, Venkiteswaran K, Subramanian T (2015) MRI evaluation of asymmetry of nigrostriatal damage in the early stage of early-onset Parkinson’s disease. Parkinsonism Relat Disord 21(6):590–596
Esterhammer R, Seppi K, Reiter E, Pinter B, Mueller C, Kremser C, Zitzelsberger T, Nocker M, Scherfler C, Poewe W, Schocke M (2015) Potential of diffusion tensor imaging and relaxometry for the detection of specific pathological alterations in Parkinson’s disease (PD). PLoS ONE 10(12):e0145493
Wen MC, Heng HS, Ng SY, Tan LC, Chan LL, Tan EK (2016) White matter microstructural characteristics in newly diagnosed Parkinson’s disease: an unbiased whole-brain study. Sci Rep 6(1):35601
Zhang Y, Wu IW, Buckley S, Coffey CS, Foster E, Mendick S, Seibyl J, Schuff N (2015) Diffusion tensor imaging of the nigrostriatal fibers in Parkinson’s disease. Mov Disord 30(9):1229–1236
Planetta PJ, Schulze ET, Geary EK, Corcos DM, Goldman JG, Little DM, Vaillancourt DE (2013) Thalamic projection fiber integrity in de novo Parkinson disease. AJNR Am J Neuroradiol 34(1):74–79
Schuff N, Wu IW, Buckley S, Foster ED, Coffey CS, Gitelman DR, Mendick S, Seibyl J, Simuni T, Zhang Y, Jankovic J, Hunter C, Tanner CM, Rees L, Factor S, Berg D, Wurster I, Gauss K, Sprenger F, Seppi K, Poewe W, Mollenhauer B, Knake S, Mari Z, McCoy A, Ranola M, Marek K (2015) Diffusion imaging of nigral alterations in early Parkinson’s disease with dopaminergic deficits. Mov Disord 30(14):1885–1892
Langley J, Huddleston DE, Merritt M, Chen X, McMurray R, Silver M, Factor SA, Hu X (2016) Diffusion tensor imaging of the substantia nigra in Parkinson’s disease revisited. Hum Brain Mapp 37(7):2547–2556
Wei X, Yan R, Chen Z, Weng R, Liu X, Gao H, Xu X, Kang Z, Liu Z, Guo Y, Liu Z, Larsen JP, Wang J, Tang B, Hallett M, Wang Q (2016) Combined diffusion tensor imaging and arterial spin labeling as markers of early Parkinson’s disease. Sci Rep 6(1):33762
Kamagata K, Hatano T, Okuzumi A, Motoi Y, Abe O, Shimoji K, Kamiya K, Suzuki M, Hori M, Kumamaru KK, Hattori N, Aoki S (2016) Neurite orientation dispersion and density imaging in the substantia nigra in idiopathic Parkinson disease. Eur Radiol 26(8):2567–2577
Kamagata K, Zalesky A, Hatano T, Di Biase MA, El Samad O, Saiki S, Shimoji K, Kumamaru KK, Kamiya K, Hori M, Hattori N, Aoki S, Pantelis C (2018) Connectome analysis with diffusion MRI in idiopathic Parkinson’s disease: evaluation using multi-shell, multi-tissue, constrained spherical deconvolution. Neuroimage Clin 17:518–529
Youn J, Lee J-M, Kwon H, Kim JS, Son TO, Cho JW (2015) Alterations of mean diffusivity of pedunculopontine nucleus pathway in Parkinson’s disease patients with freezing of gait. Parkinsonism Relat Disord 21(1):12–17
Zhan W, Kang GA, Glass GA, Zhang Y, Shirley C, Millin R, Possin KL, Nezamzadeh M, Weiner MW, Marks WJ Jr, Schuff N (2012) Regional alterations of brain microstructure in Parkinson’s disease using diffusion tensor imaging. Mov Disord 27(1):90–97
Schwarz ST, Abaei M, Gontu V, Morgan PS, Bajaj N, Auer DP (2013) Diffusion tensor imaging of nigral degeneration in Parkinson’s disease: a region-of-interest and voxel-based study at 3T and systematic review with meta-analysis. NeuroImage Clin 3:481–488
Kamagata K, Motoi Y, Abe O, Shimoji K, Hori M, Nakanishi A, Sano T, Kuwatsuru R, Aoki S, Hattori N (2012) White matter alteration of the cingulum in Parkinson disease with and without dementia: evaluation by diffusion tensor tract-specific analysis. AJNR Am J Neuroradiol 33(5):890–895
Vogt BA (2019) Chapter 13: cingulate cortex in Parkinson’s disease. In: Vogt BA (ed) Handbook of clinical neurology, vol 166. Elsevier, Amsterdam, pp 253–266
Kamagata K, Tomiyama H, Motoi Y, Kano M, Abe O, Ito K, Shimoji K, Suzuki M, Hori M, Nakanishi A (2013) Diffusional kurtosis imaging of cingulate fibers in Parkinson disease: comparison with conventional diffusion tensor imaging. Magn Reson Imaging 31(9):1501–1506
Zheng Z, Shemmassian S, Wijekoon C, Kim W, Bookheimer SY, Pouratian N (2014) DTI correlates of distinct cognitive impairments in Parkinson’s disease. Hum Brain Mapp 35(4):1325–1333
Wiltshire K, Concha L, Gee M, Bouchard T, Beaulieu C, Camicioli R (2010) Corpus callosum and cingulum tractography in Parkinson’s disease. Can J Neurol Sci 37(5):595–600
Ofori E, Pasternak O, Planetta PJ, Li H, Burciu RG, Snyder AF, Lai S, Okun MS, Vaillancourt DE (2015) Longitudinal changes in free-water within the substantia nigra of Parkinson’s disease. Brain 138(8):2322–2331
Hirata FCC, Sato JR, Vieira G, Lucato LT, Leite CC, Bor-Seng-Shu E, Pastorello BF, Otaduy MCG, Chaim KT, Campanholo KR, Novaes NP, Melo LM, Gonçalves MR, do Nascimento FBP, Teixeira MJ, Barbosa ER, Amaro E Jr, Cardoso EF (2017) Substantia nigra fractional anisotropy is not a diagnostic biomarker of Parkinson’s disease: a diagnostic performance study and meta-analysis. Eur Radiol 27(6):2640–2648
Huang S, Dong Y, Zhao J (2022) The mean kurtosis (MK) is more sensitive diagnostic biomarker than fractional anisotropy (FA) for Parkinson’s disease: a diagnostic performance study and meta-analysis. Medicine (Baltimore) 101(45):e31312
Vaillancourt D, Spraker M, Prodoehl J, Abraham I, Corcos D, Zhou X, Comella C, Little D (2009) High-resolution diffusion tensor imaging in the substantia nigra of de novo Parkinson disease. Neurology 72(16):1378–1384
Acknowledgements
Not applicable.
Funding
Not applicable (no funding received for this study).
Author information
Authors and Affiliations
Contributions
MM and AA designed the research. MM and NA performed the research and wrote the manuscript. AA (20 years’ experience of neuroradiology) and MM (10 years’ experience of neuroradiology) analyzed the collected data. MM, AT, and AS revised data and manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was approved by the research ethics committee of the Department of neurology faculty of Medicine Mansoura University on 30/5/2021, Reference number of approval: MS.21.05.1494. All patients included in this study gave a written informed consent to participate in the research.
Consent for publication
All patients included in this study gave a written informed consent to publish the data contained in this study.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mohsen, M., Mohamed, N.A.E., Bedir, A.ET.M. et al. Advanced MRI-based evaluation of gray and white matter changes in Parkinson’s disease. Egypt J Radiol Nucl Med 55, 165 (2024). https://doi.org/10.1186/s43055-024-01340-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43055-024-01340-w